You might also like
- Mclain JCDocument7 pagesMclain JCkenjiNo ratings yet
- Sedation - AyunoDocument7 pagesSedation - AyunoNADIA VICUÑANo ratings yet
- Effects of Oral Intake of WateDocument11 pagesEffects of Oral Intake of WateChenNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofFarizka Dwinda HNo ratings yet
- Swallowing Dysfunction After Critical IllnessDocument9 pagesSwallowing Dysfunction After Critical IllnessGisele DiasNo ratings yet
- Could Patient Controlled Thirst Driven Fluid Administration 2018 British JouDocument7 pagesCould Patient Controlled Thirst Driven Fluid Administration 2018 British JouSeveNNo ratings yet
- 192 Pulmonary Aspiration of Gastric Contents - 2Document6 pages192 Pulmonary Aspiration of Gastric Contents - 2ade_liaNo ratings yet
- Nutrition in The Post-Surgical Patient: Myths and MisconceptionsDocument7 pagesNutrition in The Post-Surgical Patient: Myths and MisconceptionsJuLian Neofatra SpNo ratings yet
- Gastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Document11 pagesGastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Giselle Pezoa WattsonNo ratings yet
- Mendelson Syndrome - StatPearls - NCBI BookshelfDocument8 pagesMendelson Syndrome - StatPearls - NCBI Bookshelfcesar aNo ratings yet
- 13 BaruDocument9 pages13 BaruAnditha Namira RSNo ratings yet
- Guidelance PostpreoperativeDocument5 pagesGuidelance PostpreoperativerafendyfendyNo ratings yet
- Diuretico en DBPDocument10 pagesDiuretico en DBPUriel MartzNo ratings yet
- Early Feeding After Digestive Surgery Is 43f243f3Document4 pagesEarly Feeding After Digestive Surgery Is 43f243f3sarahsamaliaNo ratings yet
- Lung Ultrasound A “ Biomarker” For FDocument8 pagesLung Ultrasound A “ Biomarker” For Flegap27No ratings yet
- Dysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Document7 pagesDysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Jihan FaadhilahNo ratings yet
- Konstipasi ICUDocument7 pagesKonstipasi ICUHusna LathiifaNo ratings yet
- 12 Impact of Spinal Anesthesia On Bladder FunctionDocument4 pages12 Impact of Spinal Anesthesia On Bladder FunctionAna-Maria CroitoruNo ratings yet
- Timing of Oral Intake After Esophagectomy A Narrative Review ofDocument19 pagesTiming of Oral Intake After Esophagectomy A Narrative Review ofAna RosiNo ratings yet
- A Therapeutic Maneuver For Oropharyngeal Dysphagia in Patients With PDDocument6 pagesA Therapeutic Maneuver For Oropharyngeal Dysphagia in Patients With PDmajid mirzaeeNo ratings yet
- Regurgitation and Aspiration: Learning ObjectivesDocument4 pagesRegurgitation and Aspiration: Learning ObjectivesGabriella Fritzie TanNo ratings yet
- Sek ResiDocument6 pagesSek ResiFadlan SeptiawanNo ratings yet
- Effect of Intraoperative Fluid Management On Outcome After Intraabdominal SurgeryDocument8 pagesEffect of Intraoperative Fluid Management On Outcome After Intraabdominal Surgeryade_liaNo ratings yet
- @anesthesia - Books - 2019 - A - Practice ExportDocument67 pages@anesthesia - Books - 2019 - A - Practice ExportMalexandra S CandoNo ratings yet
- Postoperative Ileus: Cristina R. Harnsberger, MD Justin A. Maykel, MD Karim Alavi, MD, MPHDocument5 pagesPostoperative Ileus: Cristina R. Harnsberger, MD Justin A. Maykel, MD Karim Alavi, MD, MPHfatima chrystelle nuñalNo ratings yet
- Preoperative Fasting GuidelinesDocument4 pagesPreoperative Fasting GuidelinesLuis Alberto BuendiaNo ratings yet
- 1 s2.0 S1836955319301262 Main PDFDocument8 pages1 s2.0 S1836955319301262 Main PDFAdilson Skalski ZabielaNo ratings yet
- Safety Pilot Study On DoctorsDocument4 pagesSafety Pilot Study On DoctorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Does A Water Protocol ImproveDocument11 pagesDoes A Water Protocol ImproveChenNo ratings yet
- Preoperative Fasting in Children: Ahmed Mesbah MB BCH Fcai Frca and Mark Thomas BSC (Hons) MB Bchir Frca FFFPM FaomedDocument5 pagesPreoperative Fasting in Children: Ahmed Mesbah MB BCH Fcai Frca and Mark Thomas BSC (Hons) MB Bchir Frca FFFPM FaomedSurya BugisNo ratings yet
- Auscultation For Bowel Sounds in Patients With Ileus: An Outdated Practice in The ICU?Document5 pagesAuscultation For Bowel Sounds in Patients With Ileus: An Outdated Practice in The ICU?andiNo ratings yet
- 25 RDSDocument7 pages25 RDSFinty ArfianNo ratings yet
- The Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionDocument7 pagesThe Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionPablo Segales BautistaNo ratings yet
- Perioperative Fluid Therapy For Major Surgery: Clinical Focus ReviewDocument8 pagesPerioperative Fluid Therapy For Major Surgery: Clinical Focus ReviewAbhishek LonikarNo ratings yet
- Terapia Hidrica para Cirugia MayorDocument8 pagesTerapia Hidrica para Cirugia MayorAbisaid Jonathan Salinas MemijeNo ratings yet
- Fluidtherapyinlung Disease: Elizabeth Rozanski,, Alex LynchDocument10 pagesFluidtherapyinlung Disease: Elizabeth Rozanski,, Alex LynchrianperoNo ratings yet
- Dev Roe 2015Document7 pagesDev Roe 2015nanang hidayatullohNo ratings yet
- Oral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementDocument9 pagesOral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementSasmira JamalNo ratings yet
- An Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaDocument7 pagesAn Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaMaria DemetriouNo ratings yet
- Duration of Fasting During Acute Variceal BleedingDocument4 pagesDuration of Fasting During Acute Variceal Bleedingannisa edwarNo ratings yet
- GerdDocument10 pagesGerdMulia NtiNo ratings yet
- Aex 091Document9 pagesAex 091enriquegarciagalianaNo ratings yet
- Lassen 2008Document9 pagesLassen 2008Kaliane BCNo ratings yet
- 74 Anaesthesia For Intestinal Obstruction in Children 1Document6 pages74 Anaesthesia For Intestinal Obstruction in Children 1Dr. Anish GolchhaNo ratings yet
- A Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionDocument6 pagesA Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionSantosh BabuNo ratings yet
- Bronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016Document2 pagesBronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016nathalia_pastasNo ratings yet
- Perioperative Fluid Therapy For Major SurgeryDocument8 pagesPerioperative Fluid Therapy For Major SurgeryYuda PrawiraNo ratings yet
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 pagesPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesNo ratings yet
- Tuberculous Pleural Effusion - Relapse or Re-Infection? Follow Up of A Case Report and Review of The LiteratureDocument3 pagesTuberculous Pleural Effusion - Relapse or Re-Infection? Follow Up of A Case Report and Review of The LiteraturetiaanastaNo ratings yet
- Rehabilitation of Swallowing by Exercise in Tube-Fed Patients With Pharyngeal Dysphagia Secondary To Abnormal..Document9 pagesRehabilitation of Swallowing by Exercise in Tube-Fed Patients With Pharyngeal Dysphagia Secondary To Abnormal..VickyHurtadoNo ratings yet
- Hemorragia Digestiva Alta: Manejo Actual Diagnostico y TratmientoDocument2 pagesHemorragia Digestiva Alta: Manejo Actual Diagnostico y TratmientoLuis Rafael Suárez U.No ratings yet
- Why So Many Patients With Dysphagia Have Normal Esophageal Function TestingDocument13 pagesWhy So Many Patients With Dysphagia Have Normal Esophageal Function Testingdraanalordonezv1991No ratings yet
- Pattern of Acute Intestinal Obstruction: Is There A Change in The Underlying Etiology?Document4 pagesPattern of Acute Intestinal Obstruction: Is There A Change in The Underlying Etiology?neildamiNo ratings yet
- Effects of A Free Water Protocol On Inpatients inDocument7 pagesEffects of A Free Water Protocol On Inpatients inCamila Jaque RamosNo ratings yet
- Antireflux Surgery 2015 PDFDocument247 pagesAntireflux Surgery 2015 PDFDiego Andres VasquezNo ratings yet
- Laparoscopy in The Acute AbdomenDocument15 pagesLaparoscopy in The Acute AbdomenDragoiu AlexandraNo ratings yet
- Konstipasi Aha AsaDocument7 pagesKonstipasi Aha AsaClaudia TiffanyNo ratings yet
- Noninvasive Ventilation For Prevention of Post-Extubation Respiratory Failure in Obese PatientsDocument8 pagesNoninvasive Ventilation For Prevention of Post-Extubation Respiratory Failure in Obese PatientsLestat80No ratings yet
- Pathophysiologic, Translational and Clinical Aspects of Postoperative Ileus - A ReviewDocument15 pagesPathophysiologic, Translational and Clinical Aspects of Postoperative Ileus - A ReviewRebecca BlackburnNo ratings yet
- OUTPUT Normality ND HomogenDocument1 pageOUTPUT Normality ND Homogentaupik rahmanNo ratings yet
- Mindy Millard DKK Thirst and Hydration Status in Everyday Life 2012 2 International Life Sciences InstituteDocument5 pagesMindy Millard DKK Thirst and Hydration Status in Everyday Life 2012 2 International Life Sciences Institutetaupik rahmanNo ratings yet
- Preoperative Fasting 2011Document6 pagesPreoperative Fasting 2011taupik rahmanNo ratings yet
- MANAJEMEN PASIEN JANTUNG UNTUK OPERASI NON JANTUNG Dr. SuhadiDocument63 pagesMANAJEMEN PASIEN JANTUNG UNTUK OPERASI NON JANTUNG Dr. SuhadiAnestesi RSUD Ansari SalehNo ratings yet
- Practice Guidelines For Preoperative FastingDocument18 pagesPractice Guidelines For Preoperative FastingTaufik RachmanNo ratings yet
- Asuhan Kepenataan Anestesi Anak AsmaDocument47 pagesAsuhan Kepenataan Anestesi Anak Asmataupik rahmanNo ratings yet
- Perioperative Fasting in Adults and Children .4Document14 pagesPerioperative Fasting in Adults and Children .4taupik rahmanNo ratings yet
- Kamar OperasiDocument23 pagesKamar Operasitaupik rahmanNo ratings yet
- 1 SM 1Document7 pages1 SM 1Rivanli PoliiNo ratings yet
- Maternal and Child Health: How To Achieve An Optimum Health Necessary For The Mother and BabyDocument5 pagesMaternal and Child Health: How To Achieve An Optimum Health Necessary For The Mother and BabyjanikkakristalNo ratings yet
- School Action Plan On Adopt-A-School ProgramDocument4 pagesSchool Action Plan On Adopt-A-School ProgramTitser Rock Son89% (9)
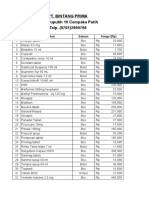
- Daftar Harga Tiap PBFDocument3 pagesDaftar Harga Tiap PBFSiti MaisyarahNo ratings yet
- Session Plan Lo2Document4 pagesSession Plan Lo2abegail capistranoNo ratings yet
- Laboratory ManagementDocument6 pagesLaboratory ManagementJamille CarayuganNo ratings yet
- 에티오피아 제약 의료기기 인허가 절차 소개 - 영문Document39 pages에티오피아 제약 의료기기 인허가 절차 소개 - 영문Kidist TesfayeNo ratings yet
- Australian Beverages OHS FINALDocument41 pagesAustralian Beverages OHS FINALPauline VukiNo ratings yet
- Affirmations PDFDocument9 pagesAffirmations PDFAlex MoonNo ratings yet
- Smart Bodyweight Training - How - Schifferle, MattDocument324 pagesSmart Bodyweight Training - How - Schifferle, MattDaniel Carballo100% (8)
- Ms SEEMABALAYAN 9 24 2022 7 04 10 PMDocument9 pagesMs SEEMABALAYAN 9 24 2022 7 04 10 PMMohammad Ali NPNo ratings yet
- Risk List TemplateDocument3 pagesRisk List Templatemanjunathaug3No ratings yet
- Troponin T Hs (High Sensitive)Document6 pagesTroponin T Hs (High Sensitive)hairiNo ratings yet
- Incident Reporting Process VisioDocument1 pageIncident Reporting Process Visiopjtx100No ratings yet
- PersonalityDocument19 pagesPersonalityMergelou LatayadaNo ratings yet
- Set1 (Answer? English) std10Document10 pagesSet1 (Answer? English) std10Saiyam JainNo ratings yet
- PCM AssignmentDocument3 pagesPCM AssignmentRUTUJA DILIP GADENo ratings yet
- Guidance Program Matrix For University TeachersDocument8 pagesGuidance Program Matrix For University TeachersAlexandra AlasNo ratings yet
- Guidance & Counselling TechniquesDocument24 pagesGuidance & Counselling TechniquessyedmirsyedNo ratings yet
- Miller - The Drama of The Gifted ChildDocument3 pagesMiller - The Drama of The Gifted ChildTopan Setiadi83% (6)
- Issues and ConcernsDocument2 pagesIssues and Concernscristina maquintoNo ratings yet
- Pharm: Building A Biopharma CompanyDocument40 pagesPharm: Building A Biopharma CompanyGeoby George100% (1)
- PEP For NetballDocument40 pagesPEP For Netballsaiqa67% (3)
- Sophia Guy ResumeDocument3 pagesSophia Guy Resumeapi-677670066No ratings yet
- WS00Q563 02gbDocument6 pagesWS00Q563 02gbRuwan Susantha PelawattaNo ratings yet
- Chapter 1-OMFS Interns 2020-Book Club (Corona Edition) PDFDocument49 pagesChapter 1-OMFS Interns 2020-Book Club (Corona Edition) PDFMGCNo ratings yet
- Shutter IslandDocument2 pagesShutter IslandMinh KhuêNo ratings yet
- Tle Grade8 2ndDocument5 pagesTle Grade8 2ndJessaRicoNo ratings yet
- Module 1 Exam - NabazaDocument4 pagesModule 1 Exam - NabazaSecret PersonNo ratings yet
- Assignment: 2C - Complete Report: Team 16Document118 pagesAssignment: 2C - Complete Report: Team 16Shuja SafdarNo ratings yet
- 10.1.1.120.2749 5Document55 pages10.1.1.120.2749 5Achulendra Ji PushkarNo ratings yet