You might also like
- Auerbach's Wilderness Medicine PDFDocument1,672 pagesAuerbach's Wilderness Medicine PDFKieran D90% (10)
- MCU 2019 Blueprints Neurology 5th EditionDocument464 pagesMCU 2019 Blueprints Neurology 5th EditionPermata GBKP Runggun Surabaya100% (2)
- Grotime - Norway InstructionsDocument7 pagesGrotime - Norway InstructionsNat NivlaNo ratings yet
- Nursing Care Plan For AIDS/HIVDocument3 pagesNursing Care Plan For AIDS/HIVderic81% (16)
- Ebook Medicine in A Day Revision Notes For Medical Exams Finals Ukmla and Foundation Years PDF Full Chapter PDFDocument67 pagesEbook Medicine in A Day Revision Notes For Medical Exams Finals Ukmla and Foundation Years PDF Full Chapter PDFregina.white324100% (26)
- 0 - 16 03 24 Provincial PEWS Nursing Power Point MarchDocument30 pages0 - 16 03 24 Provincial PEWS Nursing Power Point MarchfannyNo ratings yet
- Fundamentals of Nursing No RatioDocument15 pagesFundamentals of Nursing No RatioMeiJoyFlamianoIINo ratings yet
- ANTEPARTUM HEMORRHAGE - Afina RazibDocument11 pagesANTEPARTUM HEMORRHAGE - Afina Razibرفاعي آكرمNo ratings yet
- Fetal Surveillance: By: Kristine R. Niñonuevo-Dayao, M.DDocument43 pagesFetal Surveillance: By: Kristine R. Niñonuevo-Dayao, M.DSanjay Kumar SanjuNo ratings yet
- MODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsDocument7 pagesMODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsalliahjaneadlawanNo ratings yet
- Twin Anemia Polycythemia SyndromesDocument67 pagesTwin Anemia Polycythemia SyndromesBhupendra GuptaNo ratings yet
- October 2017 Ed Infant Fever 29-60 DaysDocument4 pagesOctober 2017 Ed Infant Fever 29-60 DaysAbdi KebedeNo ratings yet
- Perioperative Management of Massive Bleeding In-Birth Delivery (Case Series)Document1 pagePerioperative Management of Massive Bleeding In-Birth Delivery (Case Series)tikaNo ratings yet
- Clinical Pathway: Rs Medirossa 2 CibarusahDocument24 pagesClinical Pathway: Rs Medirossa 2 CibarusahOngko PriyantoNo ratings yet
- Hydrocephalus Clinical Pathway: James L. PatigayonDocument6 pagesHydrocephalus Clinical Pathway: James L. PatigayonJayson OlileNo ratings yet
- Jose RDocument17 pagesJose RMineTagraNo ratings yet
- e Obgyn อยากสอนDocument187 pagese Obgyn อยากสอนSurasit SukseeluangNo ratings yet
- G Epl PDFDocument39 pagesG Epl PDFSaenab AminNo ratings yet
- Nrg203: Care of Mother, Child, and Adolescent: (StudentDocument6 pagesNrg203: Care of Mother, Child, and Adolescent: (Studentmikhaela sencilNo ratings yet
- Importance of Ductus Venosus Doppler in Prediction of Perinatal Morbidity and MortalityDocument6 pagesImportance of Ductus Venosus Doppler in Prediction of Perinatal Morbidity and MortalityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Wnhs Og SgaiugrDocument18 pagesWnhs Og SgaiugrPoldo ReinaldoNo ratings yet
- Prospective Evaluation of Individual Cardiotocography Parameters in Predicting A Nonasphyxiated FetusDocument4 pagesProspective Evaluation of Individual Cardiotocography Parameters in Predicting A Nonasphyxiated FetusSanjay GoleNo ratings yet
- History First Prenatal VisitDocument8 pagesHistory First Prenatal VisitNadine BacalangcoNo ratings yet
- Antepartum Fetal Surveillance - SpoorthiDocument20 pagesAntepartum Fetal Surveillance - SpoorthiashwiniNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- Miscarriage or Early Pregnancy Loss-Diagnosis and ManagementDocument22 pagesMiscarriage or Early Pregnancy Loss-Diagnosis and ManagementherryNo ratings yet
- NRP 8 Edition in Canada: A Review of New Recommendations and Their RationaleDocument32 pagesNRP 8 Edition in Canada: A Review of New Recommendations and Their RationaleRavikiran Suryanarayanamurthy100% (1)
- Diagnosis and Management of Complete Kawasaki Disease in ChildrenDocument13 pagesDiagnosis and Management of Complete Kawasaki Disease in ChildrenJ SNo ratings yet
- Slide Dr. Irene OS Eria 24 Juni 2021Document39 pagesSlide Dr. Irene OS Eria 24 Juni 2021wawanNo ratings yet
- 920 FullDocument5 pages920 FullLee Chun XiangNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- MX SummaryDocument4 pagesMX SummaryPratzNo ratings yet
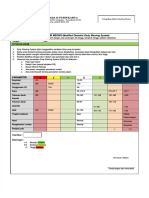
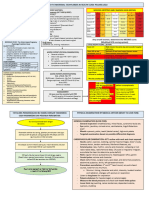
- Formulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )Document2 pagesFormulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )miraNo ratings yet
- OB Care Plan: Assessment DataDocument8 pagesOB Care Plan: Assessment Dataapi-520744935No ratings yet
- Maternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Document2 pagesMaternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Yash atriNo ratings yet
- Update On Neonatal Resuscitation Program 7 EditionDocument44 pagesUpdate On Neonatal Resuscitation Program 7 EditionRina FeronikaNo ratings yet
- Post Term PregnancyDocument12 pagesPost Term PregnancyRizky Putra Ismeldi100% (1)
- Journal Reading Neurovaskuler BanuDocument16 pagesJournal Reading Neurovaskuler BanuBanu Eko SusantoNo ratings yet
- Pro Common Pediatric EmergenciesDocument36 pagesPro Common Pediatric EmergenciesyasuyahyajpnNo ratings yet
- Early Warning Score (EWS) Procedure 239155Document10 pagesEarly Warning Score (EWS) Procedure 239155Jessica Seunghye ParkNo ratings yet
- New GAP Algorithm Draft 4-7-19Document1 pageNew GAP Algorithm Draft 4-7-19Umber AgarwalNo ratings yet
- Clinical Confrence: Neurology Division (New Case)Document20 pagesClinical Confrence: Neurology Division (New Case)Sukma SusantiNo ratings yet
- PRETERMDocument27 pagesPRETERMblatchujosephNo ratings yet
- 2020 ESC Guidelines For The Diagnosis and Management of Atrial FibrillationDocument22 pages2020 ESC Guidelines For The Diagnosis and Management of Atrial FibrillationFerry KrisnamurtiNo ratings yet
- Dapa Brief Data (14271)Document24 pagesDapa Brief Data (14271)Adel SALLAM100% (1)
- NCP Term 2Document3 pagesNCP Term 2Cassandra Grace Muerong Dela CruzNo ratings yet
- Course in The Ward 2Document17 pagesCourse in The Ward 2ABBEYGALE JOYHN GALANNo ratings yet
- Fru Sba PostersDocument17 pagesFru Sba PostersKinjal VasavaNo ratings yet
- Haemorrhage ProtocolDocument1 pageHaemorrhage ProtocolHerwinda GeraldineNo ratings yet
- Guideline For Management of Paediatric Sepsis UKDocument23 pagesGuideline For Management of Paediatric Sepsis UKLawrence SarsamNo ratings yet
- 3 - Ob Orders, or Tech, MaterialsDocument14 pages3 - Ob Orders, or Tech, MaterialsJC GoodLifeNo ratings yet
- Antepartum HaemorrhageDocument19 pagesAntepartum HaemorrhageKvy OngNo ratings yet
- DTG - TLD Presentation For National Roll Out Training - NigeriaDocument45 pagesDTG - TLD Presentation For National Roll Out Training - NigeriaOlayinka AwofoduNo ratings yet
- EMS Alphabet SoupDocument3 pagesEMS Alphabet SoupCourtney0% (1)
- Ultrasound Features in Early PregnancyDocument10 pagesUltrasound Features in Early Pregnancymadimadi11No ratings yet
- Early Warning ScoreDocument8 pagesEarly Warning ScoremalleshmadeshNo ratings yet
- WNHS Og AntepartumHaemorrhageDocument17 pagesWNHS Og AntepartumHaemorrhagelydia amaliaNo ratings yet
- Delayed Cord Clamping in Intrauterine GDocument12 pagesDelayed Cord Clamping in Intrauterine GKevin Howser T. ViNo ratings yet
- TBH IolDocument12 pagesTBH IolCheska MalubayNo ratings yet
- Protocl Posters From FRU To MC-1-1Document17 pagesProtocl Posters From FRU To MC-1-1poongodi c100% (1)
- VATER Association ChecklistDocument4 pagesVATER Association ChecklistSuzanneNo ratings yet
- Rhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Document10 pagesRhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Luis PadillaNo ratings yet
- Yamada Et Al 2023 2023 American Heart Association and American Academy of Pediatrics Focused Update On NeonatalDocument10 pagesYamada Et Al 2023 2023 American Heart Association and American Academy of Pediatrics Focused Update On NeonatalKarine SchmidtNo ratings yet
- COURAGE TrialDocument39 pagesCOURAGE TrialRirin ChandrikaNo ratings yet
- AKI Pathway (Nottingham University Hospitals April 2015)Document3 pagesAKI Pathway (Nottingham University Hospitals April 2015)Yadi SupriyadiNo ratings yet
- Pediatric Liver Intensive CareFrom EverandPediatric Liver Intensive CareNaresh ShanmugamNo ratings yet
- BW 130 OmDocument20 pagesBW 130 OmNat NivlaNo ratings yet
- Cop Vig 0519Document69 pagesCop Vig 0519Nat NivlaNo ratings yet
- SMB All Support ModelDocument15 pagesSMB All Support ModelvinhnguyenNo ratings yet
- Activity: (If The Space Is Not Enough, You May Use The Blank Space at The Back of This Paper)Document2 pagesActivity: (If The Space Is Not Enough, You May Use The Blank Space at The Back of This Paper)Jordan CruzNo ratings yet
- Notre Dame of Educational Association.Document10 pagesNotre Dame of Educational Association.Maui TingNo ratings yet
- Admintrationofmedications1 Copy 181202173921Document186 pagesAdmintrationofmedications1 Copy 181202173921Karl RobleNo ratings yet
- Hydatid DiseaseDocument9 pagesHydatid DiseaseAjinkya GaikwadNo ratings yet
- Medical Management of in Children: A Delphi Consensus: BlepharokeratoconjunctivitisDocument8 pagesMedical Management of in Children: A Delphi Consensus: Blepharokeratoconjunctivitisriskab123No ratings yet
- Health Certificate For COVID-19: Roshan Kumar Shah Male 29 04/04/1992 Nepal 11247987Document1 pageHealth Certificate For COVID-19: Roshan Kumar Shah Male 29 04/04/1992 Nepal 11247987Roshan ShahNo ratings yet
- ADHD Psychoeducation Information For Parents Schools and CliniciansDocument2 pagesADHD Psychoeducation Information For Parents Schools and CliniciansJudit BerkiNo ratings yet
- Core Conflict in PT ResearchDocument13 pagesCore Conflict in PT ResearchArooj MushtaqNo ratings yet
- Yusnida FuroidaDocument7 pagesYusnida FuroidahaseosamaNo ratings yet
- SDL Abruptio Placenta Vs Placenta PreviaDocument3 pagesSDL Abruptio Placenta Vs Placenta PreviaVannesa TarifaNo ratings yet
- CMS Statement of Deficiencies On Parkland After Failing Reinspection On 8/31/11 Printed On 9/9/11Document164 pagesCMS Statement of Deficiencies On Parkland After Failing Reinspection On 8/31/11 Printed On 9/9/11Marshall HayworthNo ratings yet
- Kashmir Healthline - IIDocument20 pagesKashmir Healthline - IIKashmir WatchNo ratings yet
- Chevannese Ellis - Circ Class WorkDocument3 pagesChevannese Ellis - Circ Class WorkChevannese EllisNo ratings yet
- Travel NurseDocument1 pageTravel NursegiangNo ratings yet
- Control of Cardiac CycleDocument16 pagesControl of Cardiac CycleazwelljohnsonNo ratings yet
- 1 Ait Abdellah Et. Al.Document11 pages1 Ait Abdellah Et. Al.Sreeja CherukuruNo ratings yet
- Persentasi Laporan Barang Keluar PT Biocare Tahun 2020Document20 pagesPersentasi Laporan Barang Keluar PT Biocare Tahun 2020FityanFathurahmanNo ratings yet
- NCP Otitis MediaDocument2 pagesNCP Otitis MediaHanz Alec100% (2)
- DeathDocument42 pagesDeathEunice ChavezNo ratings yet
- cc2019b1 SampleDocument27 pagescc2019b1 SampletanjudinNo ratings yet
- Cardiorespiratory Fitness in First Year MBBS Students: Original ArticleDocument6 pagesCardiorespiratory Fitness in First Year MBBS Students: Original ArticleTony AndersonNo ratings yet
- Factors Affecting Tendency For Drug Abuse in People Attending Addiction Treatment CentresDocument3 pagesFactors Affecting Tendency For Drug Abuse in People Attending Addiction Treatment CentresDessa Patiga IINo ratings yet
- Fetal Cystic Hygroma The Importance of Natural HistoryDocument7 pagesFetal Cystic Hygroma The Importance of Natural HistoryNGUYỄN XUÂN SangNo ratings yet
- Non Communicable DiseasesDocument28 pagesNon Communicable DiseasesPositive Infinity TutorialsNo ratings yet
- Carbetocin: 100 MCG/MLDocument2 pagesCarbetocin: 100 MCG/MLgracesimanjuntakNo ratings yet