You might also like
- Surveillance Prevention and Control of Infection PlanDocument11 pagesSurveillance Prevention and Control of Infection Plansony kurniawanNo ratings yet
- Introduction To Nursing: Pamela M. Llana, MSN, RNDocument40 pagesIntroduction To Nursing: Pamela M. Llana, MSN, RNhelen brock100% (1)
- Treatment, Prevention and Control of Intestinal Parasitic InfectionDocument49 pagesTreatment, Prevention and Control of Intestinal Parasitic InfectiononilaNo ratings yet
- 2 Infection ControlDocument34 pages2 Infection ControlMustapha S. MintehNo ratings yet
- Needle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiDocument4 pagesNeedle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiAdvanced Research PublicationsNo ratings yet
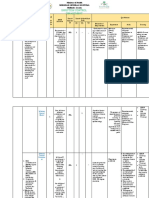
- Lesson Plan Fonn S.1Document10 pagesLesson Plan Fonn S.1Sandeep MeenaNo ratings yet
- CLM.20 Microbiology Specimen CollectionDocument19 pagesCLM.20 Microbiology Specimen Collectionfldos universeNo ratings yet
- Patient SafetyDocument30 pagesPatient Safetyariffk10No ratings yet
- Minutes of Committee On GSCASH at AMUDocument6 pagesMinutes of Committee On GSCASH at AMUAdil HossainNo ratings yet
- Infection PreventionDocument38 pagesInfection PreventionAmanda ScarletNo ratings yet
- Family Case Study FormatDocument3 pagesFamily Case Study FormatkasjdkasNo ratings yet
- Recording and Reporting in The HospitalDocument12 pagesRecording and Reporting in The HospitaltrisiavironikaNo ratings yet
- I Am Writing To Refer Patient MsDocument1 pageI Am Writing To Refer Patient MsShaira Grace Mateo-CalderonNo ratings yet
- Circulatory System FrogDocument9 pagesCirculatory System FrogLeticiaNo ratings yet
- Revised SNCU Mentoring ChecklistDocument6 pagesRevised SNCU Mentoring Checklistrani26octNo ratings yet
- Needle Stick InjuriesDocument24 pagesNeedle Stick InjuriesSarthak LaboratoryNo ratings yet
- Nursing As A Profession: Agung Setiyadi Middle East UniversityDocument33 pagesNursing As A Profession: Agung Setiyadi Middle East UniversityNise Mon KuriakoseNo ratings yet
- Source of Infections 1. Endogenous SourceDocument6 pagesSource of Infections 1. Endogenous SourceDeepu VijayaBhanuNo ratings yet
- Module 1 Case StudyDocument7 pagesModule 1 Case StudyDivine ParagasNo ratings yet
- Specimen CollectionDocument27 pagesSpecimen CollectionJohny Joseph100% (1)
- Family Care StudyDocument13 pagesFamily Care StudyLavanya ChNo ratings yet
- Needle Stick Injury Lesson PlanDocument16 pagesNeedle Stick Injury Lesson PlanJyoti Sidhu100% (1)
- Unit PlanDocument9 pagesUnit PlanMradul PrajapatiNo ratings yet
- 1-Collection, Storage and Transportataion of MicrobiologicalDocument49 pages1-Collection, Storage and Transportataion of MicrobiologicalSummi NizNo ratings yet
- Master Rotation Plan For ANM (As Per Revised Syllabus 2013)Document10 pagesMaster Rotation Plan For ANM (As Per Revised Syllabus 2013)akritiNo ratings yet
- Communicable Disease LectureDocument49 pagesCommunicable Disease LectureBernnadeth DelectorNo ratings yet
- Objective Structured Clinical Examination (OSCE) : Perceptions of Nursing Students in Tuberculosis DiagnosisDocument8 pagesObjective Structured Clinical Examination (OSCE) : Perceptions of Nursing Students in Tuberculosis DiagnosisIJAERS JOURNAL100% (1)
- Records and ReportDocument4 pagesRecords and ReportAnusikta PandaNo ratings yet
- Procedure Checklist With Rating Form Hand Hygiene Using Soap and WaterDocument4 pagesProcedure Checklist With Rating Form Hand Hygiene Using Soap and WaterRachel VillanuevaNo ratings yet
- Format of Case PresentationDocument5 pagesFormat of Case PresentationKyle DapulagNo ratings yet
- Causes of DiseaseDocument36 pagesCauses of DiseaseEdel CarlosNo ratings yet
- Master Rotation Plan For GNMDocument9 pagesMaster Rotation Plan For GNMAnanya HatiNo ratings yet
- Nursing Process: Ns. Nuning Khurotul Af'ida, S.Kep.,M.KepDocument91 pagesNursing Process: Ns. Nuning Khurotul Af'ida, S.Kep.,M.KepDindaaNo ratings yet
- Format For Periodical Report On Anti Ragging 2016 17Document3 pagesFormat For Periodical Report On Anti Ragging 2016 17anbuelectricalNo ratings yet
- Unit 8 Career PlanningDocument7 pagesUnit 8 Career PlanningVishnu LataNo ratings yet
- Management-Institutional Records & ReportsDocument18 pagesManagement-Institutional Records & ReportsmagieNo ratings yet
- Oxygen InhalationDocument4 pagesOxygen InhalationJasdeep KaurNo ratings yet
- Nursing StandardDocument22 pagesNursing StandardSudhanshu PandeyNo ratings yet
- Differences Between Benign and Malignant TumourDocument5 pagesDifferences Between Benign and Malignant TumourHanif GandohNo ratings yet
- Protein Energy Malnutrition - 2Document32 pagesProtein Energy Malnutrition - 2J V SamuelNo ratings yet
- Factors Related To Health PromotionDocument25 pagesFactors Related To Health PromotionKillian SibzNo ratings yet
- Notes On Infection PreventionDocument9 pagesNotes On Infection PreventionDipti PunjalNo ratings yet
- Infection Control DepartmentDocument3 pagesInfection Control DepartmentSherina EddingNo ratings yet
- Lesson Plan On: DocumentationDocument8 pagesLesson Plan On: DocumentationNehaNo ratings yet
- Sterilization and DisinfectionDocument24 pagesSterilization and DisinfectionMrs RehanNo ratings yet
- Clinical Evaluation FormDocument1 pageClinical Evaluation FormAndalNo ratings yet
- Colour Master PlanDocument1 pageColour Master PlanMichael BurnsNo ratings yet
- Quotation For Books in Nursing CollegeDocument12 pagesQuotation For Books in Nursing CollegeIshfaq LoneNo ratings yet
- MSC Nursing SyllabusDocument196 pagesMSC Nursing SyllabusShivani100% (2)
- HAIDocument27 pagesHAIBharath G MahendrakarNo ratings yet
- National Health Policy and PlanDocument92 pagesNational Health Policy and PlanChetan BhattaNo ratings yet
- Professional OrganisationsDocument19 pagesProfessional OrganisationsMonika100% (1)
- Nosocomial Infections in NewbornsDocument10 pagesNosocomial Infections in NewbornsAntony Rose AbyNo ratings yet
- Patient EnvironmentDocument34 pagesPatient EnvironmentSILUVERU SALOMINo ratings yet
- Application of Theory in Nursing ProcessDocument19 pagesApplication of Theory in Nursing ProcessCurly AngehNo ratings yet
- Blood Components Dosage and Their Administration (Compatibility Mode)Document7 pagesBlood Components Dosage and Their Administration (Compatibility Mode)Chandra SekarNo ratings yet
- Methods of Prevention and Control of InfectionDocument5 pagesMethods of Prevention and Control of InfectionDauda Muize AdewaleNo ratings yet
- B M W M: IO Edical Aste AnagementDocument23 pagesB M W M: IO Edical Aste AnagementJishnu JohnNo ratings yet
- PCBSC Script 23082012 1411Document8 pagesPCBSC Script 23082012 1411Santhosh.S.UNo ratings yet
- 1 s2.0 S2352396421001535 MainDocument13 pages1 s2.0 S2352396421001535 MainAmy Lalringhluani ChhakchhuakNo ratings yet
- Common: Physical CauseDocument7 pagesCommon: Physical CauseAmy Lalringhluani ChhakchhuakNo ratings yet
- Cpms College of Nursing: Assignment ON Colonic IrrigationDocument3 pagesCpms College of Nursing: Assignment ON Colonic IrrigationAmy Lalringhluani ChhakchhuakNo ratings yet
- Data Collection Procedure ContentDocument19 pagesData Collection Procedure ContentAmy Lalringhluani Chhakchhuak100% (2)
- Data Collection Sem OldDocument62 pagesData Collection Sem OldAmy Lalringhluani ChhakchhuakNo ratings yet
- CPR SeminarDocument73 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (6)
- Scrub Nurse1Document50 pagesScrub Nurse1Amy Lalringhluani Chhakchhuak100% (1)
- The Challenged ChildDocument17 pagesThe Challenged ChildAmy Lalringhluani Chhakchhuak50% (2)
- PSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Document43 pagesPSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Amy Lalringhluani Chhakchhuak100% (1)
- Cpms College of Nursing Assignment ON Bilimeter: Subject: Child Health Nursing DATED:23 JUNE 2021Document5 pagesCpms College of Nursing Assignment ON Bilimeter: Subject: Child Health Nursing DATED:23 JUNE 2021Amy Lalringhluani Chhakchhuak100% (3)
- Cpms College of Nursing: Assignment ON Setting, Use and Maintainance of Centrifuge MachineDocument6 pagesCpms College of Nursing: Assignment ON Setting, Use and Maintainance of Centrifuge MachineAmy Lalringhluani ChhakchhuakNo ratings yet
- KANGAROO MOTHER CARE ContentDocument6 pagesKANGAROO MOTHER CARE ContentAmy Lalringhluani Chhakchhuak100% (2)
- Kangaroo Mother CareDocument22 pagesKangaroo Mother CareAmy Lalringhluani Chhakchhuak100% (1)
- Administration of Nasogastric Tube FeedingDocument3 pagesAdministration of Nasogastric Tube FeedingAmy Lalringhluani Chhakchhuak100% (1)
- Family AssessmentDocument31 pagesFamily AssessmentAmy Lalringhluani ChhakchhuakNo ratings yet
- Family and Nutri AssmntDocument47 pagesFamily and Nutri AssmntAmy Lalringhluani ChhakchhuakNo ratings yet
- CPR SeminarDocument76 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (3)
- Nutritional Requirements Throughout The LifecycleDocument22 pagesNutritional Requirements Throughout The LifecycleAmy Lalringhluani ChhakchhuakNo ratings yet
- Index: SL - No Content Page NoDocument3 pagesIndex: SL - No Content Page NoAmy Lalringhluani ChhakchhuakNo ratings yet
- Child Abuse AND Battered Child SyndromeDocument90 pagesChild Abuse AND Battered Child SyndromeAmy Lalringhluani ChhakchhuakNo ratings yet
- Factors Affecting Growth and DevelopmentDocument9 pagesFactors Affecting Growth and DevelopmentAmy Lalringhluani Chhakchhuak100% (1)
- Seminar On Role of Professional Associations and UnionsDocument50 pagesSeminar On Role of Professional Associations and UnionsAmy Lalringhluani ChhakchhuakNo ratings yet
- Child Abuse ContentDocument28 pagesChild Abuse ContentAmy Lalringhluani Chhakchhuak100% (1)
- Child AbuseDocument51 pagesChild AbuseAmy Lalringhluani Chhakchhuak100% (5)
- Cpms College of Nursing: Assignment ON Electrocardiogram (ECG)Document6 pagesCpms College of Nursing: Assignment ON Electrocardiogram (ECG)Amy Lalringhluani ChhakchhuakNo ratings yet
- FTT SeminarDocument16 pagesFTT SeminarAmy Lalringhluani ChhakchhuakNo ratings yet
- Faktor-Faktor Yang Memengaruhi Kegagalan Inisiasi Menyusui Dini Pada Ibu Post Sectio Caesarea Di Rumah Sakit Tentara Binjai Tahun 2018Document14 pagesFaktor-Faktor Yang Memengaruhi Kegagalan Inisiasi Menyusui Dini Pada Ibu Post Sectio Caesarea Di Rumah Sakit Tentara Binjai Tahun 2018Salma AzzahraNo ratings yet
- 2 Programme Specification Mhpe Ugm RevDocument5 pages2 Programme Specification Mhpe Ugm RevLaksana AdijayaNo ratings yet
- Transmission of Dengue Hemorrhagic Fever in An Age Structured PopulationDocument13 pagesTransmission of Dengue Hemorrhagic Fever in An Age Structured PopulationRohan sharmaNo ratings yet
- Case Study SMALLPOX ERADICATIONDocument3 pagesCase Study SMALLPOX ERADICATIONSimran WaghelaNo ratings yet
- Guide To Female Soldier ReadinessDocument81 pagesGuide To Female Soldier Readinessasmith2005No ratings yet
- A History of Caesarean Section: From Ancient World To The Modern EraDocument5 pagesA History of Caesarean Section: From Ancient World To The Modern EraGeorgiana DNo ratings yet
- Risk Factors Associated With Diarrhea Disease Among Children Under-Five Years of Age in Kawangware Slum in Nairobi County, KenyaDocument6 pagesRisk Factors Associated With Diarrhea Disease Among Children Under-Five Years of Age in Kawangware Slum in Nairobi County, KenyaReuben MutamaNo ratings yet
- Eming Report Precipitous LaborDocument11 pagesEming Report Precipitous LaborJudeLaxNo ratings yet
- Infection Control and Covid SafetyDocument41 pagesInfection Control and Covid SafetyAdeuga ADEKUOYENo ratings yet
- Letter To ParentsDocument1 pageLetter To ParentsWSETNo ratings yet
- Audio Visual Media For Education of Washing Hands PDFDocument3 pagesAudio Visual Media For Education of Washing Hands PDFastrid berlianNo ratings yet
- Concepts of Causation of DiseasesDocument39 pagesConcepts of Causation of Diseasessunielgowda100% (1)
- Kangaroo Mother CareDocument23 pagesKangaroo Mother CarePrashant KoiralaNo ratings yet
- Bouma 2016Document16 pagesBouma 2016Eugenia BocaNo ratings yet
- Otbs LeafletDocument11 pagesOtbs LeafletlaitNo ratings yet
- All India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicDocument12 pagesAll India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicFarheen khanNo ratings yet
- Salpingitis Pleno Minggu 2 Blok 3.1Document10 pagesSalpingitis Pleno Minggu 2 Blok 3.1mustikaweniNo ratings yet
- Proforma For Registration of Subject For Dissertation Dissertation ProposalDocument11 pagesProforma For Registration of Subject For Dissertation Dissertation Proposalkuruvagadda sagarNo ratings yet
- Safety of COVID-19 Vaccines - CDCDocument3 pagesSafety of COVID-19 Vaccines - CDCkelvinkinergyNo ratings yet
- Post Cesarean Care For Mothers Attending Arua Regional Referral Hospital Drivers and ChallengesDocument16 pagesPost Cesarean Care For Mothers Attending Arua Regional Referral Hospital Drivers and ChallengesKIU PUBLICATION AND EXTENSIONNo ratings yet
- Icds, School NutritionDocument6 pagesIcds, School NutritionSrishti BajajNo ratings yet
- Acog Practice Bulletin Summary: Prelabor Rupture of MembranesDocument5 pagesAcog Practice Bulletin Summary: Prelabor Rupture of Membranesasm obgin100% (1)
- Accomplishment ReportDocument8 pagesAccomplishment ReportKevin Fernandez MendioroNo ratings yet
- 2020 American College of Rheumatology Guideline For The Management of Reproductive Health in Rheumatic and Musculoskeletal DiseasesDocument28 pages2020 American College of Rheumatology Guideline For The Management of Reproductive Health in Rheumatic and Musculoskeletal Diseasessanty ayu puspita perdhanaNo ratings yet
- FAESGraduateSchoolAtNIH2014 2015Document124 pagesFAESGraduateSchoolAtNIH2014 2015Anonymous hK9rR30No ratings yet
- Coronavirus and COVIDDocument14 pagesCoronavirus and COVIDMJ Villamor AquilloNo ratings yet
- Internal and External Vacancy Announcement (S e N I o R M & E O F F I C e R)Document2 pagesInternal and External Vacancy Announcement (S e N I o R M & E O F F I C e R)Phr InitiativeNo ratings yet
- Schemes (Part 4) - HealthDocument17 pagesSchemes (Part 4) - HealthbwerNo ratings yet
- AP U.S. HISTORY Brinkley Chapter 18 OutlinesDocument10 pagesAP U.S. HISTORY Brinkley Chapter 18 OutlinesLauren BustilloNo ratings yet
- V V V V Nonpurulent: Keflex (Cephalexin) or Cefadroxil V Purulent: I & D Gold Standard If Systemic MRSA CoverageDocument1 pageV V V V Nonpurulent: Keflex (Cephalexin) or Cefadroxil V Purulent: I & D Gold Standard If Systemic MRSA CoverageCyndiNo ratings yet