You might also like
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Factors Affecting Prescribing BHR - Dar EselamDocument7 pagesFactors Affecting Prescribing BHR - Dar EselamWassie GetahunNo ratings yet
- Archive of SIDDocument5 pagesArchive of SIDSurya WijayaNo ratings yet
- 654b PDFDocument11 pages654b PDFAzarudeenNo ratings yet
- 24 East and Central African Journal of Pharmaceutical Sciences Vol. 16 (2013) 24-30Document7 pages24 East and Central African Journal of Pharmaceutical Sciences Vol. 16 (2013) 24-30afvxfNo ratings yet
- Article 7yCODocument11 pagesArticle 7yCOAychluhm TatekNo ratings yet
- Multifunctional Medication Mishap Rca 1Document4 pagesMultifunctional Medication Mishap Rca 1MUNSIF JAWEEDNo ratings yet
- Pone 0241082Document12 pagesPone 0241082ochi rossyNo ratings yet
- 11 Thomas2020 Article InvestigatingTheIncidenceNaturDocument8 pages11 Thomas2020 Article InvestigatingTheIncidenceNaturmehakNo ratings yet
- The Impact of Clinical Pharmacists InterDocument7 pagesThe Impact of Clinical Pharmacists Interahmed1fkwnNo ratings yet
- Pharmacy Informatics (PHAR 110) : Activity 2Document10 pagesPharmacy Informatics (PHAR 110) : Activity 2Karylle RiveroNo ratings yet
- Value of A Community-Based Medication ManagementDocument12 pagesValue of A Community-Based Medication ManagementGetrudeNo ratings yet
- 64 Iajps64012018 PDFDocument7 pages64 Iajps64012018 PDFBaru Chandrasekhar RaoNo ratings yet
- Knowledge About The Administration and Regulation of High Alert Medications Among Nurses in Palestine: A Cross-Sectional StudyDocument17 pagesKnowledge About The Administration and Regulation of High Alert Medications Among Nurses in Palestine: A Cross-Sectional StudyRachel CalditoNo ratings yet
- Hospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionDocument9 pagesHospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionNisa SundariNo ratings yet
- Strengthening Pharmacy Practice in Vietnam: Findings of A Training Intervention StudyDocument9 pagesStrengthening Pharmacy Practice in Vietnam: Findings of A Training Intervention StudySarahNo ratings yet
- JPPR 1345Document6 pagesJPPR 1345Omar Nassir MoftahNo ratings yet
- Status of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiDocument8 pagesStatus of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiSagaram ShashidarNo ratings yet
- Response of Community Pharmacists To The Presentation of Back Pain: A Simulated Patient StudyDocument8 pagesResponse of Community Pharmacists To The Presentation of Back Pain: A Simulated Patient Studymia amaliaNo ratings yet
- Knowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruDocument8 pagesKnowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruShiuMan LimNo ratings yet
- Article 6yCODocument14 pagesArticle 6yCOAychluhm TatekNo ratings yet
- 89-Article Text-178-1-10-20160626Document5 pages89-Article Text-178-1-10-20160626TSuep TUtestyoNo ratings yet
- Pharmacy 07 00128 v2 PDFDocument8 pagesPharmacy 07 00128 v2 PDFMr XNo ratings yet
- Patient Satisfaction at The Muhimbili National Hospital in Dar Es Salaam, TanzaniaDocument7 pagesPatient Satisfaction at The Muhimbili National Hospital in Dar Es Salaam, TanzaniaAmirahShaleha100% (1)
- Pharmaceutical Care Services in Hospitals of Kuwait: Abdelmoneim Awad, Shareefa Al-Ebrahim, Eman AbahussainDocument9 pagesPharmaceutical Care Services in Hospitals of Kuwait: Abdelmoneim Awad, Shareefa Al-Ebrahim, Eman AbahussainPen KinhNo ratings yet
- 1 s2.0 S1319016421001407 MainDocument8 pages1 s2.0 S1319016421001407 MainarafathNo ratings yet
- Avoiding Medication Errors Caused by Nurses in The Emergency Department in Saudi ArabiaDocument5 pagesAvoiding Medication Errors Caused by Nurses in The Emergency Department in Saudi Arabiaeditorial.boardNo ratings yet
- 10 11648 J SJCM 20150405 16Document8 pages10 11648 J SJCM 20150405 16djianNo ratings yet
- 111 506 1 PBDocument12 pages111 506 1 PBAHSAN MUNEEBNo ratings yet
- 9132 32717 3 PBDocument10 pages9132 32717 3 PBVidho RiveraNo ratings yet
- Preventing Ventilator-Associated ICHEDocument8 pagesPreventing Ventilator-Associated ICHEFelix Brian FelixNo ratings yet
- Pharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessDocument7 pagesPharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessAnnafiatu zakiahNo ratings yet
- University of Birmingham: Implementing Clinical Governance in Iranian HospitalsDocument9 pagesUniversity of Birmingham: Implementing Clinical Governance in Iranian HospitalssunnyNo ratings yet
- Benefits - and - Challenges - of - Ele 6Document7 pagesBenefits - and - Challenges - of - Ele 6silfianaNo ratings yet
- Jurnal Pharmaceutical Care 3Document8 pagesJurnal Pharmaceutical Care 3Sindi CarenaNo ratings yet
- Drug Utilization Patterns in The Emergency Department A Retrospective StudyDocument6 pagesDrug Utilization Patterns in The Emergency Department A Retrospective StudyNiranjan ChapagainNo ratings yet
- Drug Utilisation Pattern and Risk Factor Assessment On Abnormal Uterine Bleeding in Reproductive Aged Women in A Tertiary Care HospitalDocument5 pagesDrug Utilisation Pattern and Risk Factor Assessment On Abnormal Uterine Bleeding in Reproductive Aged Women in A Tertiary Care Hospitaluday shekarNo ratings yet
- Ebp 1Document4 pagesEbp 1sabitaNo ratings yet
- Research ArticleDocument6 pagesResearch ArticlesirawNo ratings yet
- Barriers To The Implementation of Pharmaceutical CDocument8 pagesBarriers To The Implementation of Pharmaceutical CRoaaNo ratings yet
- Utilizing Health Analytics in ImprovingDocument9 pagesUtilizing Health Analytics in ImprovingLikithaNo ratings yet
- Drug Prescribing Pattern in Surgical Wards of A TeDocument6 pagesDrug Prescribing Pattern in Surgical Wards of A TeNiranjan ChapagainNo ratings yet
- Comparing The Quality of Private and Public Hospitals: Naceur Jabnoun and Mohammed ChakerDocument10 pagesComparing The Quality of Private and Public Hospitals: Naceur Jabnoun and Mohammed ChakerGethaLGNo ratings yet
- Medication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudyDocument18 pagesMedication Error Patients Admitted To Medical Ward in Primary Hospital, Ethiopia: Prospective Obserbetional StudybezieNo ratings yet
- Com Phar PercepDocument5 pagesCom Phar PercepDHIVYANo ratings yet
- DiscussionDocument3 pagesDiscussionMominah MayamNo ratings yet
- #26 Lamigo, Lara Elize T. 2Cph Hospital Pharmacy February 29, 2012 AssignmentDocument12 pages#26 Lamigo, Lara Elize T. 2Cph Hospital Pharmacy February 29, 2012 AssignmentLara Elize LamigoNo ratings yet
- Operating Room Nurses Knowledge and Practice of Sterile Technique 2167 1168.1000113Document5 pagesOperating Room Nurses Knowledge and Practice of Sterile Technique 2167 1168.1000113mlbrown8No ratings yet
- Barriers To Telemed-RogoveDocument6 pagesBarriers To Telemed-RogoveBoy PenangNo ratings yet
- Jac-Antimicrobial ResistanceDocument10 pagesJac-Antimicrobial ResistancenovatuschingoroNo ratings yet
- European Journal of Integrative Medicine: Research PaperDocument8 pagesEuropean Journal of Integrative Medicine: Research PaperSiti FadhillahNo ratings yet
- 2021 Article 1684Document15 pages2021 Article 1684Bala KrishnianNo ratings yet
- Ambulatory Care Groups: A Categorization of Diagnoses For Research and ManagementDocument22 pagesAmbulatory Care Groups: A Categorization of Diagnoses For Research and ManagementbrskopjeNo ratings yet
- How To Change Nurses' Behavior Leading To Medication Administration Errors Using A Survey Approach in United Christian HospitalDocument10 pagesHow To Change Nurses' Behavior Leading To Medication Administration Errors Using A Survey Approach in United Christian HospitalyyNo ratings yet
- Use of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelDocument7 pagesUse of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelEndahNo ratings yet
- Original Research Paper Public Health Care SystemDocument13 pagesOriginal Research Paper Public Health Care Systemkaniz fatemaNo ratings yet
- Patient Satisfaction On The Utilization of Traditional and Complementary Medicine Services at Public Hospitals in MalaysiaDocument9 pagesPatient Satisfaction On The Utilization of Traditional and Complementary Medicine Services at Public Hospitals in MalaysiaNurul AnnisaNo ratings yet
- Practice of Hospital Pharmacy in Bangladesh: Current PerspectiveDocument6 pagesPractice of Hospital Pharmacy in Bangladesh: Current PerspectiveMonalia Sadia Rahman Chowdhury 1811886649No ratings yet
- The Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaDocument4 pagesThe Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaAdibaNo ratings yet
- Implementation of Total Quality Management in HospitalsDocument6 pagesImplementation of Total Quality Management in HospitalsAhmed Mashaly100% (1)
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- Hobfoll Et Al., 2018 PDFDocument28 pagesHobfoll Et Al., 2018 PDFQundeel HaiderNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- The Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipDocument15 pagesThe Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Current Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDDocument9 pagesCurrent Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDmehakNo ratings yet
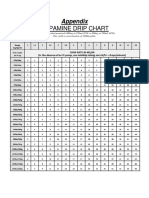
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
- Relationship Between Corporate Governance, Corporate Sustainability and Financial PerformanceDocument21 pagesRelationship Between Corporate Governance, Corporate Sustainability and Financial PerformancemehakNo ratings yet
- Michel On 2010Document33 pagesMichel On 2010Tawsif HasanNo ratings yet
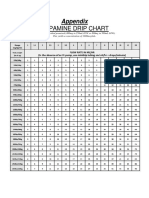
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- Guias Del Uso de Albumina e IgGDocument19 pagesGuias Del Uso de Albumina e IgGRonny Muñoz AcuñaNo ratings yet
- 2742 - OC - Doc-Smart RX Tool Fliers v2Document2 pages2742 - OC - Doc-Smart RX Tool Fliers v2Akila Shehan NilupulNo ratings yet
- Price List 2017Document4 pagesPrice List 2017Ay u Purnama WijayantiNo ratings yet
- Antidepressant Efficacy For Depression in Children and Adolescents: Industry-And NIMH-Funded StudiesDocument8 pagesAntidepressant Efficacy For Depression in Children and Adolescents: Industry-And NIMH-Funded StudiesResidentes dieciocho veintidósNo ratings yet
- Caustinerf Deciduous Bahan Devital Desidui PDFDocument1 pageCaustinerf Deciduous Bahan Devital Desidui PDFNuri AugustiniNo ratings yet
- Recurrent Herpes LabialisDocument25 pagesRecurrent Herpes LabialisGarry B GunawanNo ratings yet
- The Government of Pakistan Ministry of Health and Social WelfareDocument3 pagesThe Government of Pakistan Ministry of Health and Social Welfarefysi mackNo ratings yet
- AndaDocument64 pagesAndaShubham SuleNo ratings yet
- Introduction To Science and Risk Based Cleaning Validation Using ASTM E3106 E3219Document9 pagesIntroduction To Science and Risk Based Cleaning Validation Using ASTM E3106 E3219nsk79inNo ratings yet
- Insitu GelDocument96 pagesInsitu Gelvinsijuvin555No ratings yet
- Aspire HIMS Suite - Pushpagiri HospitalDocument58 pagesAspire HIMS Suite - Pushpagiri HospitalArun RajanNo ratings yet
- 30271-Article Text-80870-1-10-20190629 PDFDocument23 pages30271-Article Text-80870-1-10-20190629 PDFNauraNo ratings yet
- OPM ProjectDocument65 pagesOPM ProjectMohammad FaheemNo ratings yet
- Updated Product List On 24.03.2023Document24 pagesUpdated Product List On 24.03.2023Jas AyyapakkamNo ratings yet
- RA 10918 - Philippine Pharmacy ActDocument78 pagesRA 10918 - Philippine Pharmacy ActMark Tristan Asuncion86% (7)
- Astm D7709 - 12Document7 pagesAstm D7709 - 12Tanmay MandloiNo ratings yet
- Herbal DrugDocument33 pagesHerbal Drugdeepak_143No ratings yet
- Patent Term Extension Strategies in The Pharmaceutical IndustryDocument14 pagesPatent Term Extension Strategies in The Pharmaceutical IndustryRushi PatelNo ratings yet
- Drug Study PNPGHDocument6 pagesDrug Study PNPGHFaustine SalasNo ratings yet
- (2009) Cymbopogon Essential Oils Chemical Compositions and BioactivitiesDocument10 pages(2009) Cymbopogon Essential Oils Chemical Compositions and BioactivitiesshakynaNo ratings yet
- Presentation (Company Update)Document16 pagesPresentation (Company Update)Shyam SunderNo ratings yet
- II 2015 3Document301 pagesII 2015 3tuni santeNo ratings yet
- Bilayer Tablet Formulation ThesisDocument6 pagesBilayer Tablet Formulation Thesisbseb81xq100% (2)
- HPLC Analysis of Acetaminophen Tablets With Waters Alliance and Agilent SuppliesDocument6 pagesHPLC Analysis of Acetaminophen Tablets With Waters Alliance and Agilent SuppliesAman TiwariNo ratings yet
- Tablet ProblemsDocument5 pagesTablet ProblemsAnup Bajracharya75% (8)
- Employee Benefits Enrollment Expert in Chicago IL Resume Paulette BarrettDocument2 pagesEmployee Benefits Enrollment Expert in Chicago IL Resume Paulette BarrettPauletteBarrettNo ratings yet
- Aloe Vera gel-WHO Herbal Monograph PDFDocument7 pagesAloe Vera gel-WHO Herbal Monograph PDFpatelchetuNo ratings yet
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Financial Performance of Indian Pharmaceutical IndustryDocument15 pagesFinancial Performance of Indian Pharmaceutical IndustryRupal MuduliNo ratings yet
- Data Bu ShellaDocument114 pagesData Bu Shellaruri nur indahNo ratings yet
- AZT JurnalDocument7 pagesAZT JurnalRomi MaharNo ratings yet
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsFrom EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsRating: 4.5 out of 5 stars4.5/5 (6)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenFrom EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenRating: 5 out of 5 stars5/5 (62)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Little Red Book: Alcoholics AnonymousFrom EverandLittle Red Book: Alcoholics AnonymousRating: 5 out of 5 stars5/5 (20)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionFrom EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionRating: 4.5 out of 5 stars4.5/5 (117)
- Blood Orange Night: My Journey to the Edge of MadnessFrom EverandBlood Orange Night: My Journey to the Edge of MadnessRating: 4 out of 5 stars4/5 (42)
- You Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugFrom EverandYou Are More Than This Will Ever Be: Methamphetamine: The Dirty DrugNo ratings yet
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- Healing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureFrom EverandHealing the Scars of Addiction: Reclaiming Your Life and Moving into a Healthy FutureRating: 4.5 out of 5 stars4.5/5 (7)
- Guts: The Endless Follies and Tiny Triumphs of a Giant DisasterFrom EverandGuts: The Endless Follies and Tiny Triumphs of a Giant DisasterRating: 4 out of 5 stars4/5 (99)
- Addictions: A Banquet in the Grave: Finding Hope in the Power of the GospelFrom EverandAddictions: A Banquet in the Grave: Finding Hope in the Power of the GospelRating: 4.5 out of 5 stars4.5/5 (11)