You might also like
- System ProjweDocument1 pageSystem ProjweRam CharlieNo ratings yet
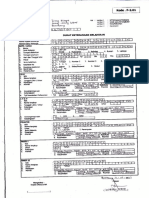
- Medical Report MR Ibrahim AktasDocument6 pagesMedical Report MR Ibrahim AktasNiraNo ratings yet
- Syarat Akte KelahiranDocument7 pagesSyarat Akte KelahiranWuryan AkbarNo ratings yet
- BMS34A146Document3 pagesBMS34A146Rohit Parmar (Computer Operator, Bangalore)No ratings yet
- Dgs IsmDocument7 pagesDgs IsmDelta MaritimeNo ratings yet
- Fuf/R0Bq - 1"'Hql-: Jhgbob-3-J-8F), T) ')Document1 pageFuf/R0Bq - 1"'Hql-: Jhgbob-3-J-8F), T) ')Bhabuk AryalNo ratings yet
- HP Application Form FrontDocument1 pageHP Application Form FrontexpeNo ratings yet
- C/o, /TR 5l: Sizq PDocument2 pagesC/o, /TR 5l: Sizq Pchandra kanta ghoshNo ratings yet
- 911 Taxpayer AssistanceDocument1 page911 Taxpayer Assistanceapi-3826089No ratings yet
- Img 20230105 0002Document1 pageImg 20230105 0002A2Z in TamilNo ratings yet
- Snoop Dogg Copyright Infringement LawsuitDocument5 pagesSnoop Dogg Copyright Infringement LawsuitIsThisLegit.comNo ratings yet
- Img S2 P.1Document1 pageImg S2 P.1larrybecker59No ratings yet
- Details of Nominee RegistrationDocument1 pageDetails of Nominee RegistrationSandy MNo ratings yet
- Notification SMS Medical College Jaipur SR Medical Officer PostsDocument4 pagesNotification SMS Medical College Jaipur SR Medical Officer PostsNeha SharmaNo ratings yet
- Notification SMS Medical College Jaipur SR Medical Officer PostsDocument4 pagesNotification SMS Medical College Jaipur SR Medical Officer PostsNeha SharmaNo ratings yet
- X NPW 116789489370Document4 pagesX NPW 116789489370Ravin JangraNo ratings yet
- Obrazac Zahtjeva Za Izdavanje VizeDocument4 pagesObrazac Zahtjeva Za Izdavanje VizeajanovicasimaNo ratings yet
- Certificate of Live Birth detailsDocument1 pageCertificate of Live Birth detailsXander ReyesNo ratings yet
- Health talk report Burn InjuryDocument2 pagesHealth talk report Burn InjuryAli Ramadhan AksodiNo ratings yet
- Admission FormDocument3 pagesAdmission FormpepperdasNo ratings yet
- Fr/ffi: (Vost Qrglefr OrqffiqDocument10 pagesFr/ffi: (Vost Qrglefr OrqffiqgirrajshakyaNo ratings yet
- Btech - Mtech Registration Document1Document2 pagesBtech - Mtech Registration Document1Ashish KRNo ratings yet
- BMS34A00222Document3 pagesBMS34A00222Rohit Parmar (Computer Operator, Bangalore)No ratings yet
- FR', e /s /": Ea PP - NGDocument2 pagesFR', e /s /": Ea PP - NGZach EdwardsNo ratings yet
- UFO Files From The UK Government DEFE 24/2027Document280 pagesUFO Files From The UK Government DEFE 24/2027Exit ExitNo ratings yet
- Img 20220311 0002 PDFDocument2 pagesImg 20220311 0002 PDFJame SonNo ratings yet
- Po 81Document1 pagePo 81leanne clariesNo ratings yet
- Islamic HPformDocument2 pagesIslamic HPformjeogilaniNo ratings yet
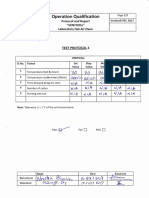
- Evaluating SOP DocumentationDocument2 pagesEvaluating SOP DocumentationFirman NugrohoNo ratings yet
- Hemlata Sangwai PrescriptionDocument2 pagesHemlata Sangwai Prescriptionanup2believeNo ratings yet
- Img 20170712 0002Document1 pageImg 20170712 0002DebashisNo ratings yet
- Rej CSFDocument1 pageRej CSF2022104625No ratings yet
- White Disclosure 5 1 07 To 6 30 07Document10 pagesWhite Disclosure 5 1 07 To 6 30 07A. KleinheiderNo ratings yet
- Customer Request FormDocument2 pagesCustomer Request FormAmarpreet SinghNo ratings yet
- Sand & Gravel Project IEE ReportDocument15 pagesSand & Gravel Project IEE ReportUml LmuNo ratings yet
- Med 328 05aug NonpDocument1 pageMed 328 05aug NonpAbhikmondal Roll-40No ratings yet
- Overtime Claim Form ProcedureDocument2 pagesOvertime Claim Form ProcedureMalar MuthiahNo ratings yet
- P2 P6 ClaimformDocument5 pagesP2 P6 ClaimformDevesh KhandareNo ratings yet
- '$#F, ?+ L, T I' Eu Oi "TFF HFDocument1 page'$#F, ?+ L, T I' Eu Oi "TFF HFZach EdwardsNo ratings yet
- Covld-Lg: Kinil'Y1 Il ,,. I PZ T:1Document4 pagesCovld-Lg: Kinil'Y1 Il ,,. I PZ T:1Mac Cristian A. CaraganNo ratings yet
- Formulir Kiriman: FL FL LLDocument2 pagesFormulir Kiriman: FL FL LLVtrock The'IlectraNo ratings yet
- Field Trip Form - Kenzi 2Document1 pageField Trip Form - Kenzi 2Alinda Nurul BadriyahNo ratings yet
- $Ur3Ugnut Ilrm @NNFHNDT Iln Tüilu (. $tudlrngrmduilr: Loqrsons ' 4/L-!Document3 pages$Ur3Ugnut Ilrm @NNFHNDT Iln Tüilu (. $tudlrngrmduilr: Loqrsons ' 4/L-!octronoNo ratings yet
- Pengisian CPPT21062019115116 PDFDocument2 pagesPengisian CPPT21062019115116 PDFChindra IrfanNo ratings yet
- Apprenticeship_training_Registration__Contract_formDocument2 pagesApprenticeship_training_Registration__Contract_formnayandeb777No ratings yet
- 01 Hora Staccato Dinicu Violin PDFDocument3 pages01 Hora Staccato Dinicu Violin PDFZain ZainNo ratings yet
- Dinicu-Heifetz - Hora StaccatoDocument3 pagesDinicu-Heifetz - Hora Staccatobustrofa100% (2)
- Form-V Certificate of Good StandingDocument2 pagesForm-V Certificate of Good StandingAsma SaleemNo ratings yet
- JN - Wo 7227 - Pt. Profab IndonesiaDocument1 pageJN - Wo 7227 - Pt. Profab IndonesiaPTSBatam TechNo ratings yet
- Analysis of temporary staging for BR #231Document33 pagesAnalysis of temporary staging for BR #231Tanvir Shahrier MahmudNo ratings yet
- Galibramed: Cdae$nlDocument4 pagesGalibramed: Cdae$nlnabila quasimahNo ratings yet
- (T& "FF Ewif: Duxr So - ReklDocument29 pages(T& "FF Ewif: Duxr So - ReklpialambkedahNo ratings yet
- Building Insurance Till 20.04.2023 (1) (1)Document5 pagesBuilding Insurance Till 20.04.2023 (1) (1)Ashmi NeupaneNo ratings yet
- Dewey PDFDocument2 pagesDewey PDFAnonymous 6qEEU3DdNo ratings yet
- Final Seniority List 8 of SDEs(T) issued by BSNLDocument1 pageFinal Seniority List 8 of SDEs(T) issued by BSNLSDE TRANS BSNLNo ratings yet
- T-.$ 7 T'T Ir I ('-D "T 'l1l':": /,&I S?EF?N STAR DP - NC (:F?SDocument4 pagesT-.$ 7 T'T Ir I ('-D "T 'l1l':": /,&I S?EF?N STAR DP - NC (:F?SDaryl DanielsNo ratings yet
- Purchase: Requisition ! EDocument2 pagesPurchase: Requisition ! ETan JokoNo ratings yet
- Chapter 2 - Shear Design SP 17-09-07Document37 pagesChapter 2 - Shear Design SP 17-09-07Alex FerrariNo ratings yet
- Fir Format For KapsitDocument15 pagesFir Format For Kapsitanirbanpwd76No ratings yet
- Chemical Hazards at Construction SitesDocument1 pageChemical Hazards at Construction Sitesanirbanpwd76No ratings yet
- DN 600m Amirabad 3Document5 pagesDN 600m Amirabad 3anirbanpwd76No ratings yet
- Design of Shear Reinforcement in RCC Structures: Intended Learning Outcomes (ILO)Document16 pagesDesign of Shear Reinforcement in RCC Structures: Intended Learning Outcomes (ILO)anirbanpwd76No ratings yet
- 1118mm - Thickness Calculator For MS or DI PipesDocument8 pages1118mm - Thickness Calculator For MS or DI Pipesanirbanpwd76No ratings yet
- Seismic Analysis 2Document6 pagesSeismic Analysis 2anirbanpwd76No ratings yet
- Seismic Analysis 2Document6 pagesSeismic Analysis 2anirbanpwd76No ratings yet
- Design of Reinforced Concrete FoundationsDocument16 pagesDesign of Reinforced Concrete Foundationsanirbanpwd76No ratings yet
- 1118mm - Thickness Calculator For MS or DI PipesDocument8 pages1118mm - Thickness Calculator For MS or DI Pipesanirbanpwd76No ratings yet
- Seismic Analysis 200 CumDocument6 pagesSeismic Analysis 200 Cumanirbanpwd76No ratings yet
- 1118mm - Thickness Calculator For MS or DI PipesDocument8 pages1118mm - Thickness Calculator For MS or DI Pipesanirbanpwd76No ratings yet
- Seismic AnalysisDocument6 pagesSeismic Analysisanirbanpwd76No ratings yet
- Seismic Analysis 2Document6 pagesSeismic Analysis 2anirbanpwd76No ratings yet
- r1 CPP Estimate July 2019Document4 pagesr1 CPP Estimate July 2019anirbanpwd76No ratings yet
- Designof DomesDocument33 pagesDesignof DomesMukesh KumarNo ratings yet
- Design Requirements - IIDocument1 pageDesign Requirements - IIanirbanpwd76No ratings yet
- Seismic Analysis 200 CumDocument6 pagesSeismic Analysis 200 Cumanirbanpwd76No ratings yet
- Unified Schedule of Rates Iw DeptDocument96 pagesUnified Schedule of Rates Iw Deptanirbanpwd76No ratings yet
- Submission of Asset Statement to West Bengal GovernmentDocument1 pageSubmission of Asset Statement to West Bengal Governmentanirbanpwd76No ratings yet
- Erroneous ATM withdrawal - Rs. 300 missing from Rs. 1500 transactionDocument1 pageErroneous ATM withdrawal - Rs. 300 missing from Rs. 1500 transactionanirbanpwd76No ratings yet
- Design Requirements - IIDocument1 pageDesign Requirements - IIanirbanpwd76No ratings yet
- Tectonics 2Document1 pageTectonics 2anirbanpwd76No ratings yet
- TectonicsDocument1 pageTectonicsanirbanpwd76No ratings yet
- Flow Area CalcDocument4 pagesFlow Area Calcanirbanpwd76No ratings yet
- Dimensional AnalysisDocument1 pageDimensional Analysisanirbanpwd76No ratings yet
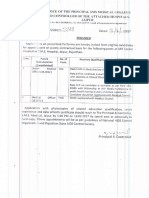
- Technical Data Pertaining To Source For Clearance by State Level Scheme Sanctioning CommitteeDocument3 pagesTechnical Data Pertaining To Source For Clearance by State Level Scheme Sanctioning Committeeanirbanpwd76No ratings yet
- MedicalDocument1 pageMedicalanirbanpwd76No ratings yet
- WTP DetailsDocument2 pagesWTP Detailsanirbanpwd76No ratings yet
- Partial Full Volume of TankDocument8 pagesPartial Full Volume of TankBabita GuptaNo ratings yet
- Vodacom Fibre - Application Form CPD - 23 August 2018Document8 pagesVodacom Fibre - Application Form CPD - 23 August 2018Mla Emmanuel ZondoNo ratings yet
- Manual Flowpet 5GDocument56 pagesManual Flowpet 5GRahkmat DanizarNo ratings yet
- Jasmine Nagata Smart GoalsDocument5 pagesJasmine Nagata Smart Goalsapi-319625868No ratings yet
- GPU, A Gnutella Processing UnitDocument27 pagesGPU, A Gnutella Processing UnitMengotti Tiziano FlavioNo ratings yet
- California Evaluation Procedures For New Aftermarket Catalytic ConvertersDocument27 pagesCalifornia Evaluation Procedures For New Aftermarket Catalytic Convertersferio252No ratings yet
- Much NeedeDocument11 pagesMuch NeedeRijul KarkiNo ratings yet
- Impact On Cocoon Quality Improvement.1Document10 pagesImpact On Cocoon Quality Improvement.1Naveen NtrNo ratings yet
- Lesson2.1-Chapter 8-Fundamentals of Capital BudgetingDocument6 pagesLesson2.1-Chapter 8-Fundamentals of Capital BudgetingMeriam HaouesNo ratings yet
- Consultants DirectoryDocument36 pagesConsultants DirectoryAnonymous yjLUF9gDTSNo ratings yet
- ABB Surge Arrester POLIM-H SD - Data Sheet 1HC0075860 E02 ABDocument4 pagesABB Surge Arrester POLIM-H SD - Data Sheet 1HC0075860 E02 ABHan HuangNo ratings yet
- Presentation On Tutorial Question On Promissory EstoppelDocument13 pagesPresentation On Tutorial Question On Promissory EstoppelNaqeeb NexerNo ratings yet
- Shangri La Hotels and Resorts SWOTDocument2 pagesShangri La Hotels and Resorts SWOTHadi Agustana100% (1)
- ChecklistDocument2 pagesChecklistKyra AlesonNo ratings yet
- Ultra Life ER14250 DatasheetDocument2 pagesUltra Life ER14250 DatasheetArslan AwanNo ratings yet
- Lecture 08Document27 pagesLecture 08simraNo ratings yet
- Inductive sensor technical specifications in 40 charactersDocument3 pagesInductive sensor technical specifications in 40 charactersBasarNo ratings yet
- Battery Calculations For Fire Alarm and Signaling SystemsDocument7 pagesBattery Calculations For Fire Alarm and Signaling Systemsleland macasinag100% (1)
- Log-PASSAT IMMO-WVWZZZ3CZ7E064873-266870km-165825miDocument13 pagesLog-PASSAT IMMO-WVWZZZ3CZ7E064873-266870km-165825miMihalciuc AlexandruNo ratings yet
- HSD (1) .Product - Spec.sheet BootstrapReserviorDocument2 pagesHSD (1) .Product - Spec.sheet BootstrapReserviorJay R SVNo ratings yet
- Sap AbapDocument7 pagesSap Abapidrees aliNo ratings yet
- New Product Development ProcessDocument29 pagesNew Product Development ProcessGAURAV SHARMA100% (1)
- Brazilian Labour Ministry Updates Machinery Safety RulesDocument89 pagesBrazilian Labour Ministry Updates Machinery Safety Rulestomy_ueziNo ratings yet
- Space Management Guidelines: Brief SummaryDocument17 pagesSpace Management Guidelines: Brief SummaryMOHD JIDINo ratings yet
- Rapidcure: Corrosion Management Products Rapidcure UwDocument1 pageRapidcure: Corrosion Management Products Rapidcure UwHeramb TrifaleyNo ratings yet
- IBM OpenPages Admin Guide 7.0 PDFDocument822 pagesIBM OpenPages Admin Guide 7.0 PDFMba NaniNo ratings yet
- 125 128Document4 pages125 128Majdi JerbiNo ratings yet
- OptiLobe Rotary Lobe PumpDocument4 pagesOptiLobe Rotary Lobe PumpRemus-Mihai GheorghitaNo ratings yet
- Digital Undated Portrait Cosy MondayDocument133 pagesDigital Undated Portrait Cosy MondayholajackNo ratings yet
- PSE Archery2015 RecurveDocument10 pagesPSE Archery2015 RecurvecarlheindlNo ratings yet