You might also like
- Sports: Strength and Conditioning Practices and Perspectives of Volleyball Coaches and PlayersDocument17 pagesSports: Strength and Conditioning Practices and Perspectives of Volleyball Coaches and PlayersΑΡΙΣΤΟΤΕΛΗΣ ΓΕΩΡΓΟΠΟΥΛΟΣNo ratings yet
- Ijerph 20 06130Document10 pagesIjerph 20 06130Priscila PintoNo ratings yet
- Junge - Soccer Injuries - A Review On Incidence and PreventionDocument10 pagesJunge - Soccer Injuries - A Review On Incidence and PreventionDaniel SantosNo ratings yet
- Research Article: Injury Risk Prediction of Aerobics Athletes Based On Big Data and Computer VisionDocument10 pagesResearch Article: Injury Risk Prediction of Aerobics Athletes Based On Big Data and Computer VisionYẾN TRẦN NGỌCNo ratings yet
- SM October 2021 AbdallahDocument8 pagesSM October 2021 AbdallahQuenton CompasNo ratings yet
- Predicting Injuries in FootballDocument15 pagesPredicting Injuries in FootballcarlosNo ratings yet
- Prediction of Injuries, Traumas and Musculoskeletal Pain in Elite Olympic and Paralympic Volleyball PlayersDocument9 pagesPrediction of Injuries, Traumas and Musculoskeletal Pain in Elite Olympic and Paralympic Volleyball Playersgonzalo osorioNo ratings yet
- Physiotherapeutic Performance in The Treatment of Anterior Cruciate Ligament Injuries in Soccer AthletesDocument7 pagesPhysiotherapeutic Performance in The Treatment of Anterior Cruciate Ligament Injuries in Soccer AthletesIJAERS JOURNALNo ratings yet
- Parpa & Michaelides 2022Document7 pagesParpa & Michaelides 2022Taha IliasNo ratings yet
- Popovicetal 2013bDocument8 pagesPopovicetal 2013bAlumnoNo ratings yet
- Sport Injuries Correct With Cover Page v2Document13 pagesSport Injuries Correct With Cover Page v2Băiceanu AlinNo ratings yet
- External Load in Male Professional Volleyball A Systematic ReviewDocument11 pagesExternal Load in Male Professional Volleyball A Systematic Reviewvictor.lefebvre8No ratings yet
- Essay 3 Final DraftDocument5 pagesEssay 3 Final Draftapi-706484561No ratings yet
- The Impact of Strength Training On The ImprovementDocument8 pagesThe Impact of Strength Training On The ImprovementPatríciaNo ratings yet
- 8BJHPA 14 2pisa1Document11 pages8BJHPA 14 2pisa1Bartłomiej SzczygiełNo ratings yet
- Game Performance Evaluation in Male Goalball PlayersDocument10 pagesGame Performance Evaluation in Male Goalball PlayersNeto JoaquimNo ratings yet
- Epidemiology of NCAA Bone Stress Injuries A Comparison of Athletes in Divisions I, II, and IIIDocument7 pagesEpidemiology of NCAA Bone Stress Injuries A Comparison of Athletes in Divisions I, II, and IIIMarliNo ratings yet
- Clay Et Al. 2013Document22 pagesClay Et Al. 2013isabela echeverriNo ratings yet
- Training Load Structure of Young Soccer Players in A Typical Training Microcycle During The Competitive and The Transition PeriodDocument9 pagesTraining Load Structure of Young Soccer Players in A Typical Training Microcycle During The Competitive and The Transition PeriodpredragbozicNo ratings yet
- Epidemiology of Injuries in Young Volleyball Athletes: A Systematic ReviewDocument9 pagesEpidemiology of Injuries in Young Volleyball Athletes: A Systematic Reviewgonzalo osorioNo ratings yet
- Contribution of Explosive Power Muscle Arms and Concentration of Floating Service in VolleyballDocument6 pagesContribution of Explosive Power Muscle Arms and Concentration of Floating Service in VolleyballRudi BoemelNo ratings yet
- Fphys 12 668145Document11 pagesFphys 12 668145Dery RimasaNo ratings yet
- Epidemiology of InjuriesDocument15 pagesEpidemiology of InjuriesAlexandru ChivaranNo ratings yet
- Sports Outcomes Review BMBGougouliasDocument35 pagesSports Outcomes Review BMBGougouliasJoselyn M Sandoval ANo ratings yet
- Prevalence of Sports Injuries in Adolescent AthletDocument6 pagesPrevalence of Sports Injuries in Adolescent AthletAstrieLarashatiNo ratings yet
- Sports Injury PreventionDocument2 pagesSports Injury PreventionRadu Cristian StuparNo ratings yet
- Background of The Studa1Document8 pagesBackground of The Studa1Henrietta ArturiaNo ratings yet
- The UEFA Injury Study: 11-Year Data Concerning 346 MCL Injuries and Time To Return To PlayDocument6 pagesThe UEFA Injury Study: 11-Year Data Concerning 346 MCL Injuries and Time To Return To PlayIlham Amal MNo ratings yet
- UEFA Expert Group Statement On Nutrition in EliteDocument27 pagesUEFA Expert Group Statement On Nutrition in EliteRosaNo ratings yet
- Uefa Expert NutritionDocument27 pagesUefa Expert NutritionMarc FloNo ratings yet
- Hockey JournalDocument9 pagesHockey JournalNabilatul AmirohNo ratings yet
- Rehab Di Pemain BolaDocument7 pagesRehab Di Pemain Bolaalit yastikaNo ratings yet
- UEFA Expert Group Statement On Nutritiona in Elite FootballDocument27 pagesUEFA Expert Group Statement On Nutritiona in Elite FootballVerenna MeloNo ratings yet
- Chapter 1 Regional Sports Training CenterDocument20 pagesChapter 1 Regional Sports Training CenterScott AlilayNo ratings yet
- Relationship Between Soccer-Specific Skills and Skill-Related Fitness in Adolescent Soccer PlayersDocument8 pagesRelationship Between Soccer-Specific Skills and Skill-Related Fitness in Adolescent Soccer PlayersQuenton CompasNo ratings yet
- HHS Public Access: Musculoskeletal Pain in Lacrosse Officials Impacts Function On The FieldDocument16 pagesHHS Public Access: Musculoskeletal Pain in Lacrosse Officials Impacts Function On The FieldfpNo ratings yet
- 2022 Soccer Coaches vs. Sport Science and Medicine Staff Who Can More Accurately Predict The Skeletal Age of High Level Youth Soccer PlayersDocument21 pages2022 Soccer Coaches vs. Sport Science and Medicine Staff Who Can More Accurately Predict The Skeletal Age of High Level Youth Soccer PlayersAziz NdamNo ratings yet
- A Rare Soccer Related Injury Traumatic PosteriorDocument6 pagesA Rare Soccer Related Injury Traumatic PosteriorDr. Andre Lopes PhD.No ratings yet
- 2021 Ball Impact Position in Recreational Male Padel PlayersDocument10 pages2021 Ball Impact Position in Recreational Male Padel PlayersFede PannutoNo ratings yet
- E000468 FullDocument9 pagesE000468 FullNAFTALIA NURAYALZANo ratings yet
- Biomechanics of Kicks in Football Are ViewDocument14 pagesBiomechanics of Kicks in Football Are ViewAkshat SinghNo ratings yet
- The Effect of Weekly Training Load Across A Competitive Microcycle On Contextual Variables in Professional SoccerDocument10 pagesThe Effect of Weekly Training Load Across A Competitive Microcycle On Contextual Variables in Professional SoccerAmin CherbitiNo ratings yet
- Evaluation of Basketball Specific Agility .96300Document31 pagesEvaluation of Basketball Specific Agility .96300Coach-NeilKhayechNo ratings yet
- Lower Back Injuries in National Collegiate Athletic Association Football PlayersDocument7 pagesLower Back Injuries in National Collegiate Athletic Association Football PlayersirmarizkyyNo ratings yet
- Association Between Concentric and Eccentric IsokiDocument11 pagesAssociation Between Concentric and Eccentric Isokiashlyn granthamNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- 1078 2020 Lip 0016Document11 pages1078 2020 Lip 0016novasesarina00No ratings yet
- Training MonitoringDocument9 pagesTraining MonitoringMateus Rotermund BarattoNo ratings yet
- Static Stretching of The Hamstring Muscle For Injury Prevention in Football Codes: A Systematic ReviewDocument10 pagesStatic Stretching of The Hamstring Muscle For Injury Prevention in Football Codes: A Systematic ReviewVeronika AtaNo ratings yet
- The Influence of Low Intensity-High Intensity PlyoDocument9 pagesThe Influence of Low Intensity-High Intensity PlyoCoach-NeilKhayechNo ratings yet
- Consensus Statement On Injury Definitions and Data Collection Procedures in Studies of Football (Soccer) InjuriesDocument9 pagesConsensus Statement On Injury Definitions and Data Collection Procedures in Studies of Football (Soccer) InjuriesLuis RamosNo ratings yet
- Quadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateDocument21 pagesQuadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateAthenaeum Scientific PublishersNo ratings yet
- English Professional Football Players Concussio - 2016 - Journal of Sport and HeDocument8 pagesEnglish Professional Football Players Concussio - 2016 - Journal of Sport and HeBUBUSNo ratings yet
- The Influence of Somatic Maturity To Anthropometrics and Body Composition in Youth Football PlayersDocument13 pagesThe Influence of Somatic Maturity To Anthropometrics and Body Composition in Youth Football PlayersJaron KungNo ratings yet
- Groin PainDocument9 pagesGroin Painjk20466402No ratings yet
- Journal Pone 0263354Document19 pagesJournal Pone 0263354marcus souzaNo ratings yet
- Osgood-Schlatter Disease in Young Athletes Katarzyna CiechanowskaDocument7 pagesOsgood-Schlatter Disease in Young Athletes Katarzyna CiechanowskaBreechesNo ratings yet
- Osgood-Schlatter Disease in Young Athletes Katarzyna CiechanowskaDocument7 pagesOsgood-Schlatter Disease in Young Athletes Katarzyna CiechanowskaBreechesNo ratings yet
- Coping Strategies of Elite Hungarian Junior Handball Players INFODocument12 pagesCoping Strategies of Elite Hungarian Junior Handball Players INFOErzsébet Bodorné NagyNo ratings yet
- Anterior Cruciate Ligament Reconstruction: A Practical Surgical GuideFrom EverandAnterior Cruciate Ligament Reconstruction: A Practical Surgical GuideNo ratings yet
- Informe Resumen. Europe. UEFA Womens Euro 2022Document25 pagesInforme Resumen. Europe. UEFA Womens Euro 2022Danilo Andres Silva EsparzaNo ratings yet
- Physical Characteristics, Physiological Attributes, and On-Field Performances of Soccer GoalkeepersDocument16 pagesPhysical Characteristics, Physiological Attributes, and On-Field Performances of Soccer GoalkeepersDanilo Andres Silva EsparzaNo ratings yet
- Physical Characteristics, Physiological Attributes, and On-Field Performances of Soccer GoalkeepersDocument16 pagesPhysical Characteristics, Physiological Attributes, and On-Field Performances of Soccer GoalkeepersDanilo Andres Silva EsparzaNo ratings yet
- Activity Monitoring in Professional Soccer Goalkeepers During Training and Match PlayDocument13 pagesActivity Monitoring in Professional Soccer Goalkeepers During Training and Match PlayDanilo Andres Silva EsparzaNo ratings yet
- The Physical Demands of Professional Soccer Goalkeepers Throughout A Week-Long Competitive Microcycle and Transiently Throughout Match-PlayDocument8 pagesThe Physical Demands of Professional Soccer Goalkeepers Throughout A Week-Long Competitive Microcycle and Transiently Throughout Match-PlayDanilo Andres Silva Esparza100% (1)
- ACSM-Resistance Training For Kids. Right From The Start 2016Document7 pagesACSM-Resistance Training For Kids. Right From The Start 2016JesusLinkinNo ratings yet
- 36 Semanas de Treinamento FutebolDocument729 pages36 Semanas de Treinamento FutebolDanilo Andres Silva EsparzaNo ratings yet
- 28.Garca-Pinillos 2019Document9 pages28.Garca-Pinillos 2019Danilo Andres Silva EsparzaNo ratings yet
- The Physical Demands of Professional Soccer Goalkeepers Throughout A Week-Long Competitive Microcycle and Transiently Throughout Match-PlayDocument8 pagesThe Physical Demands of Professional Soccer Goalkeepers Throughout A Week-Long Competitive Microcycle and Transiently Throughout Match-PlayDanilo Andres Silva Esparza100% (1)
- Academia Del Arsenal Ejercicios TécnicosDocument22 pagesAcademia Del Arsenal Ejercicios TécnicosDanilo Andres Silva Esparza100% (1)
- Activity Monitoring in Professional Soccer Goalkeepers During Training and Match PlayDocument13 pagesActivity Monitoring in Professional Soccer Goalkeepers During Training and Match PlayDanilo Andres Silva EsparzaNo ratings yet
- High Speed Running and Sprinting Profiles of Elite Soccer PlayersDocument8 pagesHigh Speed Running and Sprinting Profiles of Elite Soccer PlayersDanilo Andres Silva EsparzaNo ratings yet
- A Comparison of Maximal Aerobic Speed and Maximal Sprint Speed in Elite Youth Soccer Players 636982647024658367Document6 pagesA Comparison of Maximal Aerobic Speed and Maximal Sprint Speed in Elite Youth Soccer Players 636982647024658367Danilo Andres Silva EsparzaNo ratings yet
- Academia Del Arsenal Ejercicios TécnicosDocument22 pagesAcademia Del Arsenal Ejercicios TécnicosDanilo Andres Silva Esparza100% (1)
- A Comparison of Maximal Aerobic Speed and Maximal Sprint Speed in Elite Youth Soccer Players 636982647024658367Document6 pagesA Comparison of Maximal Aerobic Speed and Maximal Sprint Speed in Elite Youth Soccer Players 636982647024658367Danilo Andres Silva EsparzaNo ratings yet
- Reporte Fisico AS - Roma-Porto - Fitness DatDocument11 pagesReporte Fisico AS - Roma-Porto - Fitness DatDanilo Andres Silva EsparzaNo ratings yet
- Rondo Your Brains Out PDFDocument47 pagesRondo Your Brains Out PDFDanilo Andres Silva EsparzaNo ratings yet
- A 10-Week Randomized Trial Comparing Eccentric vs. Concentric Hmastring Strength Training in Well Trained Soccer PlayersDocument7 pagesA 10-Week Randomized Trial Comparing Eccentric vs. Concentric Hmastring Strength Training in Well Trained Soccer PlayersCristian YanezNo ratings yet
- Gabbe TT 2018Document9 pagesGabbe TT 2018Danilo Andres Silva EsparzaNo ratings yet
- SSG Vs Match BucheitDocument24 pagesSSG Vs Match BucheitDanilo Andres Silva EsparzaNo ratings yet
- Effectsof Sit Factorson PAin SL2018Document12 pagesEffectsof Sit Factorson PAin SL2018Danilo Andres Silva EsparzaNo ratings yet
- Elite Football of 2030 Will Not Be The Same As That of 2020Document3 pagesElite Football of 2030 Will Not Be The Same As That of 2020Danilo Andres Silva EsparzaNo ratings yet
- Programa de Futbol Base 10 y 11 Años PDFDocument276 pagesPrograma de Futbol Base 10 y 11 Años PDFAnonymous fuiFHBDQ100% (1)
- Block Periodization Versus Traditional Training Theory: A ReviewDocument12 pagesBlock Periodization Versus Traditional Training Theory: A ReviewbomgorilaoNo ratings yet
- Castagna JSCR 2006 Yoyo Tests CorrelationsDocument6 pagesCastagna JSCR 2006 Yoyo Tests CorrelationsDanilo Andres Silva EsparzaNo ratings yet
- An Evidence Based Approach ForDocument15 pagesAn Evidence Based Approach ForDanilo Andres Silva EsparzaNo ratings yet
- The Validity of The Push Band 20 During Vertical JDocument13 pagesThe Validity of The Push Band 20 During Vertical JDanilo Andres Silva EsparzaNo ratings yet
- Analisis LesionesDocument7 pagesAnalisis LesionesDanilo Andres Silva EsparzaNo ratings yet
- Castagna JSCR 2006 Yoyo Tests CorrelationsDocument6 pagesCastagna JSCR 2006 Yoyo Tests CorrelationsDanilo Andres Silva EsparzaNo ratings yet
- HOPEDocument3 pagesHOPEAndrea Venesse NaldaNo ratings yet
- Npte Sample QuestionsDocument61 pagesNpte Sample QuestionsMaybelyn Jorado100% (1)
- Exercises For Scapulothoracic and Postural Muscle StrengthDocument2 pagesExercises For Scapulothoracic and Postural Muscle StrengthSantosh PatiNo ratings yet
- Butchering The Human Carcass For Human ConsumptionDocument5 pagesButchering The Human Carcass For Human Consumptionpablo_muradNo ratings yet
- DHZ Alien U2000C (1) (2) - 230427 - 121227Document19 pagesDHZ Alien U2000C (1) (2) - 230427 - 121227Sérgio ÍtaloNo ratings yet
- Sun SalutationDocument2 pagesSun SalutationAshish MaheshwariNo ratings yet
- Npte Sample Questions 2Document61 pagesNpte Sample Questions 2Maybelyn Jorado50% (2)
- Swimmer StretchingDocument6 pagesSwimmer Stretchinggeorge104100% (1)
- Arthroscopic Revision Rotator CuffDocument10 pagesArthroscopic Revision Rotator CuffPujia Cahya AmaliaNo ratings yet
- Sandhigata Vikar Visheshank December 2007Document12 pagesSandhigata Vikar Visheshank December 2007dr amitNo ratings yet
- Material Mini NetterDocument17 pagesMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNo ratings yet
- Physio4all... : Orthopaedics Assessment Sagar NaikDocument9 pagesPhysio4all... : Orthopaedics Assessment Sagar NaikRajeev Tiwari100% (2)
- Delta XtendDocument60 pagesDelta XtendMarcelo KrauseNo ratings yet
- CH 5 Joints PDFDocument4 pagesCH 5 Joints PDFIbra TutorNo ratings yet
- Upper Limb OrthosisDocument84 pagesUpper Limb OrthosisShriyaNo ratings yet
- Viloma PranayamaDocument17 pagesViloma PranayamaRajesh KumarNo ratings yet
- Sports Injuries: How Are Classified and Managed?Document14 pagesSports Injuries: How Are Classified and Managed?Rachmat BayuNo ratings yet
- Manual in Radiographic Positioning.Document116 pagesManual in Radiographic Positioning.Jestia Lyn EngracialNo ratings yet
- A Paediatric Musculoskeletal Competence FrameworkDocument18 pagesA Paediatric Musculoskeletal Competence FrameworkPT Depart AMCHNo ratings yet
- Physics 135 Fall 2018 Exam 1 Form 1Document21 pagesPhysics 135 Fall 2018 Exam 1 Form 1Rubab ImtiazNo ratings yet
- Birth Brachial Plexus Palsy UpdateDocument8 pagesBirth Brachial Plexus Palsy UpdateDyah SafitriNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic Injuriesamber tariqNo ratings yet
- Hygienic Physiology: With Special Reference To The Use of Alcoholic Drinks and Narcotics by Steele, Joel DormanDocument235 pagesHygienic Physiology: With Special Reference To The Use of Alcoholic Drinks and Narcotics by Steele, Joel DormanGutenberg.orgNo ratings yet
- The Lung Meridian Acu-PointsDocument1 pageThe Lung Meridian Acu-PointsVicaas VSNo ratings yet
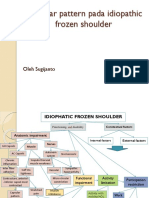
- Capsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoDocument11 pagesCapsular Pattern Pada Idiopathic Frozen Shoulder: Oleh SugijantoRhany JulyatiNo ratings yet
- Uppercross SyndromeDocument5 pagesUppercross SyndromeNazmul IslamNo ratings yet
- Yoga For Anatomy CompleteDocument71 pagesYoga For Anatomy CompleteVasily ZabelinNo ratings yet
- Anatomy Samplex 2Document30 pagesAnatomy Samplex 2Jo Anne80% (10)
- Approach To Patients EULARDocument35 pagesApproach To Patients EULARstuckinbedNo ratings yet
- Traumatology Orthopaedic EXAMDocument219 pagesTraumatology Orthopaedic EXAMElo GonçalvesNo ratings yet