You might also like
- Hepatotoxicity Induced by High Dose of Methylprednisolone Therapy in A Patient With Multiple Sclerosis: A Case Report and Brief Review of LiteratureDocument5 pagesHepatotoxicity Induced by High Dose of Methylprednisolone Therapy in A Patient With Multiple Sclerosis: A Case Report and Brief Review of LiteratureBayu ParmikaNo ratings yet
- Acute Pancreatitis PathoDocument5 pagesAcute Pancreatitis PathoENo ratings yet
- Acute Kidney Injury Due To Pien Tze HuangDocument3 pagesAcute Kidney Injury Due To Pien Tze HuangDavid PalashNo ratings yet
- Acute He Pa To Toxicity After Ingestion of Morinda.22Document3 pagesAcute He Pa To Toxicity After Ingestion of Morinda.22Kay RuzNo ratings yet
- Acute Pancreatitis With Normal Serum Lipase: A Case SeriesDocument4 pagesAcute Pancreatitis With Normal Serum Lipase: A Case SeriesSilvina VernaNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Case Study For Colon CancerDocument2 pagesCase Study For Colon Cancerrhimineecat7150% (2)
- 6 Ashkin 062012Document79 pages6 Ashkin 062012Anonymous QPXAgjBwNo ratings yet
- Drug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in TreatmentDocument5 pagesDrug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in Treatmentmufqifitra160491No ratings yet
- Acetylcysteine For Acetaminophen Poisoning: Clinical TherapeuticsDocument8 pagesAcetylcysteine For Acetaminophen Poisoning: Clinical TherapeuticsShalini DosiNo ratings yet
- CetirizineDocument3 pagesCetirizinenephylymNo ratings yet
- Gastrointestinal Case StudiesDocument5 pagesGastrointestinal Case StudiesJude Micko Bunyi AlipitNo ratings yet
- Dialysis Free Protocol For Some End Stage Renal Disease PatientsDocument7 pagesDialysis Free Protocol For Some End Stage Renal Disease PatientsDannieCiambelliNo ratings yet
- Case ReportDocument5 pagesCase ReportAlfi YatunNo ratings yet
- BJSTR MS Id 001072Document4 pagesBJSTR MS Id 001072Jatin SinghNo ratings yet
- Preprint Not Peer ReviewedDocument21 pagesPreprint Not Peer ReviewedАмина ПлотноваNo ratings yet
- HyperthyroidDocument7 pagesHyperthyroidHaerun Nisa SiregarNo ratings yet
- Tuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghDocument3 pagesTuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghAnastasia Lilian SuryajayaNo ratings yet
- 12 CR Methotrexate Induced LiverDocument2 pages12 CR Methotrexate Induced LiverAnonymous bFByZ3FydNo ratings yet
- Two Cases of Recurrent ADIH in ChildrenDocument6 pagesTwo Cases of Recurrent ADIH in ChildrenTry Ahmad MirzaNo ratings yet
- X. Young 2011 HepDocument11 pagesX. Young 2011 HepJuan Carlos FloresNo ratings yet
- International Reports: Incidence of Hepatotoxicity Due To Antitubercular Medicines and Assessment of Risk FactorsDocument6 pagesInternational Reports: Incidence of Hepatotoxicity Due To Antitubercular Medicines and Assessment of Risk FactorsWelki VernandoNo ratings yet
- HerbalifeDocument7 pagesHerbalifeLuis Galeana MuñozNo ratings yet
- Eslam 2020 Mafld A Consensus Driven Proposed NDocument38 pagesEslam 2020 Mafld A Consensus Driven Proposed NRafael GermanoNo ratings yet
- Severe Cholestasis and Renal Failure Associated With The Use of The Designer Steroid Superdrol™ (Methasteron™) A Case Report and Literature ReviewDocument3 pagesSevere Cholestasis and Renal Failure Associated With The Use of The Designer Steroid Superdrol™ (Methasteron™) A Case Report and Literature ReviewPádraig Ó ĊonġaileNo ratings yet
- Nrgastro 2011Document2 pagesNrgastro 2011James LeungNo ratings yet
- Liver Toxicity of Sitaxentan in Pulmonary Arterial HypertensionDocument2 pagesLiver Toxicity of Sitaxentan in Pulmonary Arterial Hypertensionefra maneNo ratings yet
- A Case Report On Benign Prostatic Hyperplasia With Homeopathic RemediesDocument6 pagesA Case Report On Benign Prostatic Hyperplasia With Homeopathic RemediesBaru Chandrasekhar RaoNo ratings yet
- Drug-Induced Liver Injury Associated With Complementary and Alternative MedicinesDocument8 pagesDrug-Induced Liver Injury Associated With Complementary and Alternative MedicinesTimotius Kevin NatanaelNo ratings yet
- Problems in Diagnosis Approach For Carcinoma of Pancreatic HeadDocument6 pagesProblems in Diagnosis Approach For Carcinoma of Pancreatic HeadfikriafisNo ratings yet
- A Case Study On Urinalysis and Body FluidsDocument17 pagesA Case Study On Urinalysis and Body Fluidsrakish16No ratings yet
- The Oncologist 1998 Goumas 50 3Document4 pagesThe Oncologist 1998 Goumas 50 3Kammi HumedNo ratings yet
- A Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver DiseaseDocument6 pagesA Placebo-Controlled Trial of Silymarin in Patients With Nonalcoholic Fatty Liver Diseasesnn123456No ratings yet
- Case Report: Acute Liver Injury With Severe Coagulopathy in Marasmus Caused by A Somatic Delusional DisorderDocument3 pagesCase Report: Acute Liver Injury With Severe Coagulopathy in Marasmus Caused by A Somatic Delusional DisorderNur Ismi Mustika FebrianiNo ratings yet
- Komplit Kasus Ingris ES Edit 22 Agusts 2013Document48 pagesKomplit Kasus Ingris ES Edit 22 Agusts 2013YhooogaNo ratings yet
- RajaniDocument8 pagesRajaniArnette Castro de GuzmanNo ratings yet
- Graves' Disease Case Report Links Severe Hypoalbuminemia to ThyrotoxicosisDocument2 pagesGraves' Disease Case Report Links Severe Hypoalbuminemia to ThyrotoxicosisAbdur Rachman Ba'abdullahNo ratings yet
- Resmetirom Phase 2 Clinical Trial ResultsDocument13 pagesResmetirom Phase 2 Clinical Trial ResultsRayNo ratings yet
- Falciparum Malaria Complicated by Acute PancreatitisDocument3 pagesFalciparum Malaria Complicated by Acute PancreatitisMuhammad Taufik AdhyatmaNo ratings yet
- Palliative Stenting With or Without Radiotherapy For Inoperable Esophageal CarcinomaDocument7 pagesPalliative Stenting With or Without Radiotherapy For Inoperable Esophageal CarcinomaBella StevannyNo ratings yet
- PRISMA-P 2015 ChecklistDocument16 pagesPRISMA-P 2015 ChecklistPUTRI LITAPRIANINo ratings yet
- Garlic (Allium Sativum) and Ginger (Zingiber Officinale) Attenuate Structural Nephropathy Progression in Streptozotocin-Induced Diabetic RatsDocument10 pagesGarlic (Allium Sativum) and Ginger (Zingiber Officinale) Attenuate Structural Nephropathy Progression in Streptozotocin-Induced Diabetic RatsAna HerawatiNo ratings yet
- GR 080013Document3 pagesGR 080013malik003No ratings yet
- Do Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Document29 pagesDo Proton Pump Inhibitors Increase Mortality in Cirrhotic Patients With Spontaneous Bacterial Peritonitis?Muhammad Rehan AnisNo ratings yet
- Shared RX Modules For FinalsDocument11 pagesShared RX Modules For FinalsOdyNo ratings yet
- Ceju 66 00246Document4 pagesCeju 66 00246Àlex MataNo ratings yet
- Interpretation of Liver Function Test in Ayurveda-2Document4 pagesInterpretation of Liver Function Test in Ayurveda-2tasmitadas9101No ratings yet
- JournalDocument8 pagesJournalFentiNo ratings yet
- Pi Is 0016508519325685Document14 pagesPi Is 0016508519325685Sefrilia Miftahul JannahNo ratings yet
- Hepatitis Alcohólica Novedades EASL 2018-1Document10 pagesHepatitis Alcohólica Novedades EASL 2018-1Ingrid González EfronNo ratings yet
- Bacopa HepatotoxicityDocument9 pagesBacopa Hepatotoxicityadrip234No ratings yet
- EMQs for Medical Students Volume 2 GastroenterologyDocument30 pagesEMQs for Medical Students Volume 2 Gastroenterologynob2011nob100% (1)
- Acetaminophen-Induced Hepatotoxicity PDFDocument12 pagesAcetaminophen-Induced Hepatotoxicity PDFFranklin AvilaNo ratings yet
- Tyrosinemia Type 1 Case Report in Saudi ChildDocument4 pagesTyrosinemia Type 1 Case Report in Saudi ChildMelanie Pad-ayNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing DiagnosisLeonardo S. Posadas Sr.No ratings yet
- Tamara Case StudyDocument6 pagesTamara Case Studymike0% (1)
- Jaundice Fulminant Hepatic Failure HE Symposium Dr. Vinod KVDocument2 pagesJaundice Fulminant Hepatic Failure HE Symposium Dr. Vinod KVPinimNo ratings yet
- Nishinaga CGA and Team InterventionDocument6 pagesNishinaga CGA and Team InterventioninunNo ratings yet
- Preview ML Concept of NormalDocument5 pagesPreview ML Concept of NormalinunNo ratings yet
- Preview ML Concept of NormalDocument5 pagesPreview ML Concept of NormalinunNo ratings yet
- Qat Chewing and Autoimmune Hepatitis - True Association or CoincidenceDocument7 pagesQat Chewing and Autoimmune Hepatitis - True Association or CoincidenceinunNo ratings yet
- Kurtz 1996Document7 pagesKurtz 1996inunNo ratings yet
- Lent Soma Scale For Cervix Carcinoma RadiotherapyDocument7 pagesLent Soma Scale For Cervix Carcinoma RadiotherapyinunNo ratings yet
- g2124 PDFDocument4 pagesg2124 PDFFawzahNo ratings yet
- Cuidados Del Adulto MayorDocument9 pagesCuidados Del Adulto MayorBeatrizNo ratings yet
- Nishinaga CGA and Team InterventionDocument6 pagesNishinaga CGA and Team InterventioninunNo ratings yet
- Lent Soma Scale For Cervix Carcinoma RadiotherapyDocument7 pagesLent Soma Scale For Cervix Carcinoma RadiotherapyinunNo ratings yet
- Family Medicine in Arab CountriesDocument7 pagesFamily Medicine in Arab CountriesinunNo ratings yet
- Kurtz 1996Document7 pagesKurtz 1996inunNo ratings yet
- Dengue Virus: Iqbal Ainnun Azis Tutor 23Document10 pagesDengue Virus: Iqbal Ainnun Azis Tutor 23inunNo ratings yet
- Development of Family Medicine in The Middle EastDocument7 pagesDevelopment of Family Medicine in The Middle EastinunNo ratings yet
- Dietary Assessment-23Document22 pagesDietary Assessment-23inun100% (1)
- Cervical Cancer: An OverviewDocument12 pagesCervical Cancer: An OverviewinunNo ratings yet
- 10 11648 J CNN 20200402 12Document4 pages10 11648 J CNN 20200402 12inunNo ratings yet
- Shingles Rash and Pain DefinitionDocument21 pagesShingles Rash and Pain DefinitioninunNo ratings yet
- Corynebacterium diphtheriae: Pathogenesis and IdentificationDocument10 pagesCorynebacterium diphtheriae: Pathogenesis and IdentificationinunNo ratings yet
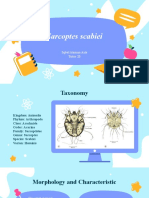
- Biology of Sarcoptes ScabieiDocument8 pagesBiology of Sarcoptes ScabieiinunNo ratings yet
- Health Maintainance in PregnancyDocument10 pagesHealth Maintainance in PregnancyinunNo ratings yet
- Formatif 1Document6 pagesFormatif 1inunNo ratings yet
- Antibiotic Therapy For Shigella DysenteryDocument107 pagesAntibiotic Therapy For Shigella DysenteryinunNo ratings yet
- 10 11648 J CNN 20200402 12Document4 pages10 11648 J CNN 20200402 12inunNo ratings yet
- Kolej Matrikulasi Pulau Pinang Kementerian Pelajaran Malaysia 13200 Kepala BatasDocument9 pagesKolej Matrikulasi Pulau Pinang Kementerian Pelajaran Malaysia 13200 Kepala Bataskelisa157100% (2)
- 1 An Overview of Physical and Phase ChangeDocument5 pages1 An Overview of Physical and Phase ChangeGede KrishnaNo ratings yet
- Gpfs Overview v33Document54 pagesGpfs Overview v33Farha AzadNo ratings yet
- Warsaw Pact Order of Battle - 1989Document61 pagesWarsaw Pact Order of Battle - 1989Zero Knight100% (1)
- Shaw's play about a sculptor and his creationDocument8 pagesShaw's play about a sculptor and his creationEmanuel BurculetNo ratings yet
- Drill Pipe Performance DataDocument35 pagesDrill Pipe Performance DatasnatajNo ratings yet
- Full Download Test Bank For Positive Psychology 4th Edition Lopez PDF Full ChapterDocument36 pagesFull Download Test Bank For Positive Psychology 4th Edition Lopez PDF Full Chaptershaps.tortillayf3th100% (21)
- Future Developments in Management AccountingDocument4 pagesFuture Developments in Management AccountingAmar narayanNo ratings yet
- Unit 4 FSQCDocument28 pagesUnit 4 FSQCvaralakshmi KNo ratings yet
- Lab Manual Ds&BdalDocument100 pagesLab Manual Ds&BdalSEA110 Kshitij BhosaleNo ratings yet
- Unit DNI Candidate Guidance v51612018191423Document14 pagesUnit DNI Candidate Guidance v51612018191423Carla Baraybar100% (1)
- Project's Estimated Residual Income and Required InvestmentDocument7 pagesProject's Estimated Residual Income and Required InvestmentblueberryNo ratings yet
- Bahan Belajar Ujian Akhir SekolahDocument13 pagesBahan Belajar Ujian Akhir SekolahArga AnggaraNo ratings yet
- Pakistan'S Economy & The Role of Imf & World Bank On ITDocument15 pagesPakistan'S Economy & The Role of Imf & World Bank On ITAsaad Imtiaz100% (1)
- Project Management Remote ExamDocument4 pagesProject Management Remote ExamAnis MehrabNo ratings yet
- Jurnal SinusitisDocument49 pagesJurnal SinusitisAramanda Dian100% (1)
- Case 26 Star River Electronics - Group Thạch Trung Chương HiểnDocument12 pagesCase 26 Star River Electronics - Group Thạch Trung Chương HiểnTrương ThạchNo ratings yet
- Mhdp-08-Rsdll Report Issue 6.0Document159 pagesMhdp-08-Rsdll Report Issue 6.0billNo ratings yet
- Compact NSX - Micrologic 5-6-7 - User Guide 11Document1 pageCompact NSX - Micrologic 5-6-7 - User Guide 11amnd amorNo ratings yet
- MCMC Methods For Multi-Response Generalized LinearDocument22 pagesMCMC Methods For Multi-Response Generalized LinearkyotopinheiroNo ratings yet
- Giáo trình TACN Đồ họa 1 - 2021 - chính thứcDocument57 pagesGiáo trình TACN Đồ họa 1 - 2021 - chính thứcHeo BiểnNo ratings yet
- Lubricated Coupling TrainingDocument47 pagesLubricated Coupling TrainingTheerayootNo ratings yet
- Soft Course Material Iran 2007 PDFDocument646 pagesSoft Course Material Iran 2007 PDFLa Picarona del Peru100% (1)
- ENGG378 - 948 HydroPower-Lecture - 1 - 2019 PDFDocument34 pagesENGG378 - 948 HydroPower-Lecture - 1 - 2019 PDFJ CNo ratings yet
- THE END - MagDocument164 pagesTHE END - MagRozze AngelNo ratings yet
- Chap3-2e SO2 Absorption ExampleDocument8 pagesChap3-2e SO2 Absorption Exampledarkelf_riderNo ratings yet
- PP 1Document33 pagesPP 1Vishnu IngleNo ratings yet
- VKS INFRA DPR Submission for NHAI Bihar ProjectDocument1 pageVKS INFRA DPR Submission for NHAI Bihar ProjectamirNo ratings yet
- Troubleshooting Guide: Multifunctional Digital SystemsDocument132 pagesTroubleshooting Guide: Multifunctional Digital SystemsnguyenhieuproNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)