You might also like
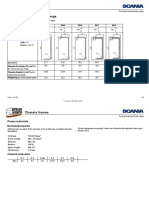
- Scania Chassis FramesDocument6 pagesScania Chassis Framesaamirmub100% (1)
- Design of A Lightweight Heavy Goods Vehicle TrailerDocument17 pagesDesign of A Lightweight Heavy Goods Vehicle TraileraamirmubNo ratings yet
- The Impression: A Blueprint To Restorative SuccessDocument5 pagesThe Impression: A Blueprint To Restorative SuccessgyulamaNo ratings yet
- 282MEDocument2 pages282MEdutt0784No ratings yet
- CERIA Interior CR 6100Document2 pagesCERIA Interior CR 6100HardiansyahNo ratings yet
- PavanarticleDocument12 pagesPavanarticleMrunali Porete CSE-11No ratings yet
- Packaging Textiles: The Use of Textile Materials in Consumer Packaging Is Exhibited in The Following ProductsDocument10 pagesPackaging Textiles: The Use of Textile Materials in Consumer Packaging Is Exhibited in The Following ProductsDewan Ajuad Hossain RifatNo ratings yet
- Dermatological ToxicityDocument95 pagesDermatological ToxicitySunilNo ratings yet
- PT. Indowijaya Sakti Teguh: Epoxy Primer Chemical ResistantDocument3 pagesPT. Indowijaya Sakti Teguh: Epoxy Primer Chemical Resistantyuli yonoNo ratings yet
- Patent LeatherDocument10 pagesPatent LeathervinothjohnnashNo ratings yet
- The Art of Chemical PeelingDocument5 pagesThe Art of Chemical PeelingBrian MacíaNo ratings yet
- Technical Bulletin Surface Treatment - EnCRES DUBUIT - 06Document2 pagesTechnical Bulletin Surface Treatment - EnCRES DUBUIT - 06marimadiNo ratings yet
- Chemtech GM Clear - English (Uk) - Issued.06.12.2007Document3 pagesChemtech GM Clear - English (Uk) - Issued.06.12.2007Mohamed Farag50% (2)
- Use of Enzymes in Cosmetics Proposed Enzymatic Peel ProcedureDocument7 pagesUse of Enzymes in Cosmetics Proposed Enzymatic Peel ProcedureAlejandra CortezNo ratings yet
- Transdermal Drug Delivery System - ManufDocument13 pagesTransdermal Drug Delivery System - ManufEsther Faith GabrielNo ratings yet
- Skin Glues For Wound Closure: Variable Results With Some WoundsDocument3 pagesSkin Glues For Wound Closure: Variable Results With Some WoundsjprakashjjNo ratings yet
- Basics of Skin ExposureDocument6 pagesBasics of Skin ExposureMustafa Cuneyt GezenNo ratings yet
- Transdermal Drug DeliveryDocument38 pagesTransdermal Drug DeliveryJhansi SattiNo ratings yet
- Transdermal Drug Delivery System: Shirode Rahul ADocument37 pagesTransdermal Drug Delivery System: Shirode Rahul AFrancisco MarcanoNo ratings yet
- A Review On Film Forming Gel FFGDocument10 pagesA Review On Film Forming Gel FFGEditor IJTSRDNo ratings yet
- TDDS #Document52 pagesTDDS #britoraj100% (2)
- Chemical Protective ClothingDocument47 pagesChemical Protective ClothingKeshav Dhawan50% (2)
- Surface Wetting Pre Treatment MethodsDocument2 pagesSurface Wetting Pre Treatment MethodsNattaya PunrattanasinNo ratings yet
- Research Journal of Pharmaceutical, Biological and Chemical SciencesDocument7 pagesResearch Journal of Pharmaceutical, Biological and Chemical ScienceszainabNo ratings yet
- T I: A B R S: HE Mpression Lueprint To Estorative UccessDocument7 pagesT I: A B R S: HE Mpression Lueprint To Estorative Uccessreal_septiady_madrid3532No ratings yet
- Adhesives Poly ChemDocument20 pagesAdhesives Poly ChemdivyaNo ratings yet
- Epoxy BasicsDocument6 pagesEpoxy BasicsMuthuKumarNo ratings yet
- Geeta AggarwalDocument9 pagesGeeta Aggarwalkhanaijaza129397No ratings yet
- Dokumentasjon DimethiconeDocument6 pagesDokumentasjon DimethiconeJacqueline SunaryoNo ratings yet
- Dermaroller: Dr. Stefani Marietta 1880721009 Dr. Felicia Hartono 1880 721033 Dr. Adellia Nike 1880721039Document26 pagesDermaroller: Dr. Stefani Marietta 1880721009 Dr. Felicia Hartono 1880 721033 Dr. Adellia Nike 1880721039Cindy Caroline Santoso SieNo ratings yet
- A Review On Film Forming Gel Novel Drug Delivery SystemDocument10 pagesA Review On Film Forming Gel Novel Drug Delivery SystemEditor IJTSRDNo ratings yet
- HDBeauty PMU Manual2Document36 pagesHDBeauty PMU Manual2Taita Vlakoff NunesNo ratings yet
- Pharmaeutical Technology Ii Topical and Transdermal Drug Delivery: Skin Structure and FunctionDocument7 pagesPharmaeutical Technology Ii Topical and Transdermal Drug Delivery: Skin Structure and FunctionJoelle SleibeNo ratings yet
- Transdermal OpoidsDocument6 pagesTransdermal OpoidsSau Yee ChowNo ratings yet
- Deproteinized Natural Rubber Latex-Hydroxypropylmethyl CelluloseDocument11 pagesDeproteinized Natural Rubber Latex-Hydroxypropylmethyl CelluloseLucas CarvalhoNo ratings yet
- Novel Colloidal Delivery Systems For Dermal Application: M.A. Schubert, C.C. Müller-GoymannDocument12 pagesNovel Colloidal Delivery Systems For Dermal Application: M.A. Schubert, C.C. Müller-GoymannAhmad AinurofiqNo ratings yet
- Material Science Miscellaneous Engg. Materials Layout: Chapter Iv - Adhesives, Bonding Plastics and PaintsDocument21 pagesMaterial Science Miscellaneous Engg. Materials Layout: Chapter Iv - Adhesives, Bonding Plastics and PaintsPrakash KatdareNo ratings yet
- Natural SilkDocument3 pagesNatural Silkapi-302611547No ratings yet
- 1 s2.0 S1818087617301538 MainDocument11 pages1 s2.0 S1818087617301538 MainismayaniNo ratings yet
- PT. Indowijaya Sakti Teguh: Puffin Epoxy Chemical Resistant TOP 70%Document3 pagesPT. Indowijaya Sakti Teguh: Puffin Epoxy Chemical Resistant TOP 70%yuli yonoNo ratings yet
- Polymer, 10Document9 pagesPolymer, 10Mohammed MNo ratings yet
- Nicotine Transdermal Patches Using Polymeric Natural Rubber As The Matrix Controlling System Effect of Polymer and Plasticizer BlendsDocument10 pagesNicotine Transdermal Patches Using Polymeric Natural Rubber As The Matrix Controlling System Effect of Polymer and Plasticizer BlendsLucas CarvalhoNo ratings yet
- FlexicreteDocument3 pagesFlexicreteapi-302611547No ratings yet
- Megayacht Imperial Antifouling DataDocument3 pagesMegayacht Imperial Antifouling DatakormatekNo ratings yet
- Transdermal Drug Delivery System: Shirode Rahul ADocument37 pagesTransdermal Drug Delivery System: Shirode Rahul Aنور الهدىNo ratings yet
- Preparation of Histological SpecimensDocument4 pagesPreparation of Histological SpecimensAqilah HazwaniNo ratings yet
- Surface Energy: Corona Treatment Is One of The Methods To Increases The Surface Energy of Plastic Films, FoilsDocument5 pagesSurface Energy: Corona Treatment Is One of The Methods To Increases The Surface Energy of Plastic Films, FoilsHeart Touching VideosNo ratings yet
- HDBeauty MicrobladingDocument32 pagesHDBeauty Microbladingmungaimoses394No ratings yet
- Skin Surface Model Material As A Substrate For Adhesion To Skin TestingDocument17 pagesSkin Surface Model Material As A Substrate For Adhesion To Skin TestingAnakyn JaegerNo ratings yet
- Introduction MethodsDocument70 pagesIntroduction MethodsHohai ConcepcionNo ratings yet
- Pharmaceutical Applications of Plasticized Polymers PDFDocument23 pagesPharmaceutical Applications of Plasticized Polymers PDFSatish VaidyaNo ratings yet
- Handbook of Adhesives and SealantsDocument4 pagesHandbook of Adhesives and SealantsHarymsl MslNo ratings yet
- Assignment On Technical Textile... Sec..aDocument23 pagesAssignment On Technical Textile... Sec..aShamima akterNo ratings yet
- Introduction To Cosmetic DermatologyDocument41 pagesIntroduction To Cosmetic DermatologyElizabeth TovittoNo ratings yet
- Penetration of Drugs Through Skin, A Complex Rate-Controlling MembraneDocument10 pagesPenetration of Drugs Through Skin, A Complex Rate-Controlling MembraneFawwaziNo ratings yet
- Transunilac Finish 331Document4 pagesTransunilac Finish 331bhukyanaik02No ratings yet
- 283MEDocument2 pages283MEdutt0784No ratings yet
- Fevicol PurDocument3 pagesFevicol PurVenkata ChadaNo ratings yet
- Nature Medicine. Conducted by Researchers From Emory University and The Georgia Institute ofDocument5 pagesNature Medicine. Conducted by Researchers From Emory University and The Georgia Institute ofKashmiri HinduismNo ratings yet
- Tablet Coating 2-2Document30 pagesTablet Coating 2-2Abdur RaquibNo ratings yet
- TD Eco Ee 4010Document2 pagesTD Eco Ee 4010HardiansyahNo ratings yet
- 2004 FE Simulations of Impact On Metal & CompoDocument114 pages2004 FE Simulations of Impact On Metal & CompoaamirmubNo ratings yet
- IJMS 50 2008 - ZhixueDocument8 pagesIJMS 50 2008 - ZhixueaamirmubNo ratings yet
- Öz and Öztürk - 2022 - Effect of Carbon Filler-Modified Epoxy Adhesive OnDocument14 pagesÖz and Öztürk - 2022 - Effect of Carbon Filler-Modified Epoxy Adhesive OnaamirmubNo ratings yet
- Materials 16 02870Document26 pagesMaterials 16 02870aamirmubNo ratings yet
- Effect of GNP and MWCNT Addition On Lap ShearDocument6 pagesEffect of GNP and MWCNT Addition On Lap ShearaamirmubNo ratings yet
- Cross Cogging Torque AnalysisDocument4 pagesCross Cogging Torque AnalysisaamirmubNo ratings yet
- Ballistic Resistance of Novel Amorphous-Alloy-Reinforced Perforated ArmorDocument15 pagesBallistic Resistance of Novel Amorphous-Alloy-Reinforced Perforated ArmoraamirmubNo ratings yet
- 2014 SCIEI May Sydney Conf Proceedings IACSITDocument5 pages2014 SCIEI May Sydney Conf Proceedings IACSITaamirmubNo ratings yet
- Progressive Failure Analysis of FRC Containing HoleDocument16 pagesProgressive Failure Analysis of FRC Containing HoleaamirmubNo ratings yet
- A Numerical Investigation and Experimental Validation On Chip Morphology of Aluminum Alloy 6061 During Orthogonal MachiningDocument6 pagesA Numerical Investigation and Experimental Validation On Chip Morphology of Aluminum Alloy 6061 During Orthogonal MachiningaamirmubNo ratings yet
- Multiscale Modeling of Human Bone: Y. W. Kwon B. R. ClumpnerDocument11 pagesMultiscale Modeling of Human Bone: Y. W. Kwon B. R. ClumpneraamirmubNo ratings yet
- Multiobjective Optimization of Mechanical Properties Based On The Composition of AdhesivesDocument24 pagesMultiobjective Optimization of Mechanical Properties Based On The Composition of AdhesivesaamirmubNo ratings yet
- Patient-Specific Bone Multiscale Modelling FracturDocument67 pagesPatient-Specific Bone Multiscale Modelling FracturaamirmubNo ratings yet
- Experimental Investigation On The Ballistic Resistance of Monolithic and Multi-Layred Plates Against Ogival-Nose Rigid Projectiles (2012)Document12 pagesExperimental Investigation On The Ballistic Resistance of Monolithic and Multi-Layred Plates Against Ogival-Nose Rigid Projectiles (2012)aamirmubNo ratings yet
- Design and Characteristics of Hybrid Composite Armor Subjected To Projectile Impact (2013)Document6 pagesDesign and Characteristics of Hybrid Composite Armor Subjected To Projectile Impact (2013)aamirmubNo ratings yet
- Lightweight Ceramic Composite Armour SystemDocument5 pagesLightweight Ceramic Composite Armour SystemaamirmubNo ratings yet
- Mil STD 709dDocument30 pagesMil STD 709daamirmubNo ratings yet
- Computer Methods in Biomechanics and Biomedical EngineeringDocument10 pagesComputer Methods in Biomechanics and Biomedical EngineeringaamirmubNo ratings yet
- Modelling and Simulation of Brittle ArmourDocument166 pagesModelling and Simulation of Brittle ArmouraamirmubNo ratings yet
- Neo Fiberglass Mesh 160 GSM TDSDocument1 pageNeo Fiberglass Mesh 160 GSM TDSAkosh AchuNo ratings yet
- Tut-371 No.2Document8 pagesTut-371 No.2fletusdiabloiNo ratings yet
- Application of Plain Carbon SteelDocument39 pagesApplication of Plain Carbon SteelDivyesh Kumar0% (1)
- Manual Plancha OSTER GCSTSP6104Document42 pagesManual Plancha OSTER GCSTSP6104Jorge Leon75% (4)
- D. Lesson PlanDocument5 pagesD. Lesson PlanLowell Lastima Ramboyong PasturanNo ratings yet
- Yuan - 2021 - Preparation of Complex Shaped Aluminum Foam by A Novel Casting-Foaming MethodDocument4 pagesYuan - 2021 - Preparation of Complex Shaped Aluminum Foam by A Novel Casting-Foaming MethodmishtisonuNo ratings yet
- Rajeshs Home PDFDocument30 pagesRajeshs Home PDFCh. NarendraNo ratings yet
- FiberDocument5 pagesFiberEka Nanda PutrianiNo ratings yet
- CoreBOO Brochure April 2023Document7 pagesCoreBOO Brochure April 2023Lavkesh KumarNo ratings yet
- Confinement of Columns and Wall Boundary Elements Using Headed BarsDocument9 pagesConfinement of Columns and Wall Boundary Elements Using Headed BarsJuaNNo ratings yet
- 2-Design For Action Effects - M & N (2014)Document15 pages2-Design For Action Effects - M & N (2014)george santiagoNo ratings yet
- Manning's Equation & Table of N ValuesDocument1 pageManning's Equation & Table of N ValuesSupawat RangsiwongNo ratings yet
- HASLE Brochure Cement Ind Us Tri en (EUversion 3-Fl.)Document6 pagesHASLE Brochure Cement Ind Us Tri en (EUversion 3-Fl.)mohamadi42No ratings yet
- ReynoArch ACP LouversDocument4 pagesReynoArch ACP LouversReynobond indiaNo ratings yet
- Ub 214Document3 pagesUb 214DANIEL SALAZARNo ratings yet
- 8.50 Lacks Pipeline CorrectedDocument68 pages8.50 Lacks Pipeline CorrectedChimakurthy NagarapanchayatNo ratings yet
- PolymersDocument43 pagesPolymersKaizNo ratings yet
- Basic Concepts in Engineering Metallurgy - Gate Mechanical Concepts - Mechanical Engineering World - Project Ideas - Seminar Topics - E-Books (PDF) - New TrendsDocument4 pagesBasic Concepts in Engineering Metallurgy - Gate Mechanical Concepts - Mechanical Engineering World - Project Ideas - Seminar Topics - E-Books (PDF) - New TrendsSandeep PrajapatiNo ratings yet
- Phet Online Lab Conductors and Insulators1Document2 pagesPhet Online Lab Conductors and Insulators1Michelle CenNo ratings yet
- Vol Keramik HTDocument408 pagesVol Keramik HTrajef FathNo ratings yet
- 2020 Enerack Ground Solar MountDocument14 pages2020 Enerack Ground Solar MountEcosenseTechnologies GreenenergyNo ratings yet
- F-DMD Technical DataDocument1 pageF-DMD Technical DataĐức LêNo ratings yet
- Pedo GIC ShamikaDocument75 pagesPedo GIC ShamikaSrishti SrivastavaNo ratings yet
- Mixing Maching For Refractory ConcreteDocument9 pagesMixing Maching For Refractory Concreteorangel anayaNo ratings yet
- One Partner. Many Experts.: Product Reference GuideDocument11 pagesOne Partner. Many Experts.: Product Reference GuideTélémaqueNo ratings yet
- Sanitary and Industrial RTDsDocument4 pagesSanitary and Industrial RTDsPrihartono Danan WingusNo ratings yet
- Sikacryl®-150: Product Data SheetDocument3 pagesSikacryl®-150: Product Data SheetMoatz HamedNo ratings yet
- Jet Lube Grease CatalogDocument24 pagesJet Lube Grease CatalogKapil TiwariNo ratings yet
- Shield Bright 309L-1Document1 pageShield Bright 309L-1adanmeneses1No ratings yet
- 4 Tanur Tinggi (Blast Furnace)Document67 pages4 Tanur Tinggi (Blast Furnace)Samsul BahriNo ratings yet