You might also like
- Plabable-Gems-31. Respiratory Plabable GemsDocument68 pagesPlabable-Gems-31. Respiratory Plabable GemsHabo Habo100% (1)
- ICU One Pager Pulmonar Renal Syndrome-JbxqojDocument1 pageICU One Pager Pulmonar Renal Syndrome-JbxqojmujawayezuNo ratings yet
- ANCA Tests Guide: Understanding Interpretation and IndicationsDocument3 pagesANCA Tests Guide: Understanding Interpretation and IndicationsGREENCROSS PALDINo ratings yet
- ANCA Related Vasculitis PDFDocument51 pagesANCA Related Vasculitis PDF陳思任No ratings yet
- Lap Abdominal Surg-1Document4 pagesLap Abdominal Surg-1Rizwan AhmedNo ratings yet
- ICU One Pager Massive Hemoptysis v11Document1 pageICU One Pager Massive Hemoptysis v11Nicholas HelmstetterNo ratings yet
- Cardio Vascular PDFDocument148 pagesCardio Vascular PDFStefana RoxanaNo ratings yet
- Vasculitis: Allison Eunice B. ServandoDocument116 pagesVasculitis: Allison Eunice B. ServandoAllison Eunice ServandoNo ratings yet
- Clinical Approach To: Rapid Progressive GlomerulonephritisDocument38 pagesClinical Approach To: Rapid Progressive GlomerulonephritisMiri PravdaNo ratings yet
- Firman - CKD ST V + CKDMBDDocument28 pagesFirman - CKD ST V + CKDMBDAdinda DianNo ratings yet
- Pedia NephrologyDocument4 pagesPedia NephrologyJulie Anne AciertoNo ratings yet
- 8-Ecg in CovidsDocument35 pages8-Ecg in CovidsyandraNo ratings yet
- Congenital Heart Defects: Part Ii-Duct Dependent ChdsDocument28 pagesCongenital Heart Defects: Part Ii-Duct Dependent ChdslindaNo ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- Community-Acquired PneumoniaDocument22 pagesCommunity-Acquired PneumoniaIMAFDNo ratings yet
- Pulmonary-Renal SyndromesDocument9 pagesPulmonary-Renal SyndromesJanio Alberto OvalleNo ratings yet
- NCPDocument2 pagesNCPJulianne MagtunaoNo ratings yet
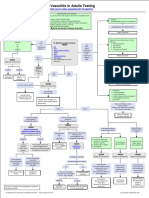
- I Am Sharing 'Vasculitis - in - Adults - Testing - Algorithm' With YouDocument1 pageI Am Sharing 'Vasculitis - in - Adults - Testing - Algorithm' With YouMahmoud AbouemiraNo ratings yet
- Pulmonary Hypertension and EchocardiographyDocument57 pagesPulmonary Hypertension and EchocardiographySiska Istanah Wong SintingNo ratings yet
- ICU One Pager - Pulmonary Embolism RX PDFDocument1 pageICU One Pager - Pulmonary Embolism RX PDFAbdul RaufNo ratings yet
- The Role of Blood Gas and D-Dimer Evaluation in The DiagnostDocument18 pagesThe Role of Blood Gas and D-Dimer Evaluation in The Diagnostifan zulfantriNo ratings yet
- Pulmonary ArtesiaDocument6 pagesPulmonary ArtesiaMaulani NurlatifahNo ratings yet
- Shaggy Aorta 6Document2 pagesShaggy Aorta 6Eghet SilviuNo ratings yet
- C19 SPACE ToolKit ChecklistsDocument8 pagesC19 SPACE ToolKit ChecklistsAdrian BălanNo ratings yet
- Diagnosis and Treatment of Radiation ProctitisDocument2 pagesDiagnosis and Treatment of Radiation ProctitispatNo ratings yet
- Pulmonary EmbolismDocument63 pagesPulmonary EmbolismeuniicehahaNo ratings yet
- Approach To Subarachnoid Hemorrhage - DR DikaDocument27 pagesApproach To Subarachnoid Hemorrhage - DR DikaOnyedika EgbujoNo ratings yet
- Imaging of Thoracic Aspergillosis: Prof. G Ferretti Chu GrenobleDocument50 pagesImaging of Thoracic Aspergillosis: Prof. G Ferretti Chu GrenobleIqbal AbdillahNo ratings yet
- Recruitment Checklist: Security Forces Hospital ProgramDocument4 pagesRecruitment Checklist: Security Forces Hospital ProgramDerick RanaNo ratings yet
- IM Part 1Document48 pagesIM Part 1sasghfdgNo ratings yet
- IM Part 1 and 2 CombinedDocument100 pagesIM Part 1 and 2 CombinedsasghfdgNo ratings yet
- Dignostic Investigation in Respiratory SystemDocument99 pagesDignostic Investigation in Respiratory SystemGopi JaladiNo ratings yet
- Uac VS UvcDocument1 pageUac VS UvcJunaidahMubarakAliNo ratings yet
- Drug StudyDocument30 pagesDrug StudyClaire MachicaNo ratings yet
- Thrombosis ManagementDocument14 pagesThrombosis ManagementJessa MaeNo ratings yet
- Acute Chest SyndromeDocument28 pagesAcute Chest SyndromeJohn OkidiNo ratings yet
- Algoritmo-COVID19 PDF pdf81552961419587596081570311557Document1 pageAlgoritmo-COVID19 PDF pdf81552961419587596081570311557Keti JanevskaNo ratings yet
- BRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISDocument3 pagesBRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISmarielleaudreeyNo ratings yet
- Acute GlomerulonephritisDocument27 pagesAcute GlomerulonephritisKumara GuruNo ratings yet
- Acute Glomerulonephritis PDFDocument27 pagesAcute Glomerulonephritis PDFRaj RNo ratings yet
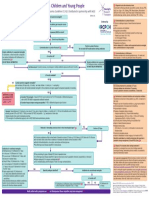
- Incorporates NICE Bacterial Meningitis and Meningococcal Septicaemia Guideline CG102. Distributed in Partnership With NICEDocument1 pageIncorporates NICE Bacterial Meningitis and Meningococcal Septicaemia Guideline CG102. Distributed in Partnership With NICELilisNo ratings yet
- Major Causes of ARF and Clinical FeaturesDocument3 pagesMajor Causes of ARF and Clinical FeaturespurwandinyNo ratings yet
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocument21 pagesMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariNo ratings yet
- ElectrodiagnosticsDocument4 pagesElectrodiagnosticsAndy Delos ReyesNo ratings yet
- PLABABLE Gems Respiratory MedicineDocument68 pagesPLABABLE Gems Respiratory Mediciney æskNo ratings yet
- TID Part 2 Dr. Lu 2014 SalveDocument3 pagesTID Part 2 Dr. Lu 2014 SalveMACATANGAY, GAELLE LISETTENo ratings yet
- Glomerulonephritis MindmapDocument1 pageGlomerulonephritis MindmapAlia AnasNo ratings yet
- Top Ten Family Practice DiagosesDocument6 pagesTop Ten Family Practice DiagosesKatrina HumphreyNo ratings yet
- Road To MEmMedDocument12 pagesRoad To MEmMedWinnie WongNo ratings yet
- Shock in Covid PatientDocument21 pagesShock in Covid PatientGHALEB A. AlmekhlafiNo ratings yet
- Blunt Abdominal Trauma Case ReviewDocument3 pagesBlunt Abdominal Trauma Case ReviewGio Tamaño BalisiNo ratings yet
- Table of Content: Post-Streptococcal Glomerulonephritis 3Document5 pagesTable of Content: Post-Streptococcal Glomerulonephritis 3rup100% (1)
- Ampullary Carcinoma - Dr. Limchiaco, J.Document11 pagesAmpullary Carcinoma - Dr. Limchiaco, J.Neil Victor Ongco PajugotNo ratings yet
- Downloadfile 5Document51 pagesDownloadfile 5Faheem Ul HasanNo ratings yet
- Pulmonary Embolism Diagnosis and InterpretationDocument60 pagesPulmonary Embolism Diagnosis and InterpretationGordana PuzovicNo ratings yet
- Arteriovenous Malformation 1001Document19 pagesArteriovenous Malformation 1001housic1No ratings yet
- Physiomonitoring TransDocument4 pagesPhysiomonitoring TransAimie DagaleaNo ratings yet
- SPIDER WEB ACUTE RENAL FAILURE (ARF/AKIDocument3 pagesSPIDER WEB ACUTE RENAL FAILURE (ARF/AKITien KartiniNo ratings yet
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument2 pagesNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar IzzoNo ratings yet
- ICU One Pager Flow Volume LoopsDocument1 pageICU One Pager Flow Volume LoopsRonald MoralesNo ratings yet
- Cremer 2016Document9 pagesCremer 2016Ronald MoralesNo ratings yet
- Hernia Diafragmatica 2019Document7 pagesHernia Diafragmatica 2019Ronald MoralesNo ratings yet
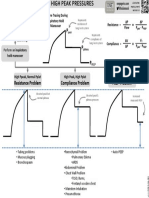
- VENT TROUBLESHOOTING: HIGH PEAK PRESSURESDocument1 pageVENT TROUBLESHOOTING: HIGH PEAK PRESSURESRonald MoralesNo ratings yet
- Nmda - RDocument8 pagesNmda - RRonald MoralesNo ratings yet
- Pain Anxiety Delirium: Rass CAM ICUDocument1 pagePain Anxiety Delirium: Rass CAM ICUNicholas HelmstetterNo ratings yet
- Estandarización Entrevista Apego en Chile para AdultosDocument9 pagesEstandarización Entrevista Apego en Chile para AdultosDaniel GSNo ratings yet
- Neonatal Hypoglycemia: A Review: Mahdi Alsaleem, MD, Lina Saadeh, MD, and Deepak Kamat, MD, PHD, FaapDocument6 pagesNeonatal Hypoglycemia: A Review: Mahdi Alsaleem, MD, Lina Saadeh, MD, and Deepak Kamat, MD, PHD, FaapRonald MoralesNo ratings yet
- Prediciendo SDR Usando Espectroscopía Del Residuo Gástrico - ClínicaDocument6 pagesPrediciendo SDR Usando Espectroscopía Del Residuo Gástrico - ClínicaRonald MoralesNo ratings yet
- Nejm - Eritropoyetina para Neuroprotección en PrematurosDocument11 pagesNejm - Eritropoyetina para Neuroprotección en PrematurosRonald MoralesNo ratings yet
- Efecto Del Surfatante Menos Invasivo Sobre La Oxigenación CerebralDocument9 pagesEfecto Del Surfatante Menos Invasivo Sobre La Oxigenación CerebralRonald MoralesNo ratings yet
- Acog PromDocument14 pagesAcog PromjjlazarteNo ratings yet
- Calidad de Los Probiítcos para PrematurosDocument4 pagesCalidad de Los Probiítcos para PrematurosRonald MoralesNo ratings yet
- QuantifiersDocument19 pagesQuantifiersThelma EstudilloNo ratings yet
- QuantifiersDocument19 pagesQuantifiersThelma EstudilloNo ratings yet
- Gui Ewb Unit01 Print and WorkDocument3 pagesGui Ewb Unit01 Print and WorkRonald MoralesNo ratings yet
- DC 40 S1 FinalDocument4 pagesDC 40 S1 FinalRonald MoralesNo ratings yet
- BW Mc2 XWHM y Na ManualDocument23 pagesBW Mc2 XWHM y Na ManualSatyasrinivas PulavarthiNo ratings yet
- SITE. Defining Project Goals & ObjectivesDocument1 pageSITE. Defining Project Goals & Objectivescoach balaNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- Celecoxib Identification MethodsDocument5 pagesCelecoxib Identification Methodsabc1679No ratings yet
- PCOS Diet Cookbook For Newly Diagnosed IndividualsDocument67 pagesPCOS Diet Cookbook For Newly Diagnosed Individualsmavendave4lifeNo ratings yet
- Rational Choice TheoryDocument6 pagesRational Choice TheoryMaria Theresa HerbolingoNo ratings yet
- Starbucks BSC Project Analyzes Store PerformanceDocument8 pagesStarbucks BSC Project Analyzes Store Performanceandrea100% (1)
- Old Fashioned Southern Tea CakesDocument2 pagesOld Fashioned Southern Tea CakesDB ScottNo ratings yet
- STC Bec Wir Plu D 0209 01 PDFDocument10 pagesSTC Bec Wir Plu D 0209 01 PDFAdel MorsyNo ratings yet
- REMOTE Calculator Tool May 21 2013Document77 pagesREMOTE Calculator Tool May 21 2013Leyner Garcia MezquitaNo ratings yet
- Mill Housings Mangal SinghDocument5 pagesMill Housings Mangal SinghGun SmithNo ratings yet
- Fuente As-IDocument4 pagesFuente As-IadalaviNo ratings yet
- Fosfomycin: Review and Use Criteria BackgroundDocument12 pagesFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Gaggia Cadorna Milk Full Instruction ManualDocument76 pagesGaggia Cadorna Milk Full Instruction ManualKanen Coffee, LLC.No ratings yet
- Plane Bearings: Material Indicator Shape or SeriesDocument4 pagesPlane Bearings: Material Indicator Shape or SeriesJuan LoaizaNo ratings yet
- RV Failure: Pathophysiology, Diagnosis and TreatmentDocument16 pagesRV Failure: Pathophysiology, Diagnosis and TreatmentRizky Regia TriseynesyaNo ratings yet
- SEN Code of Practice 2001Document148 pagesSEN Code of Practice 2001Matt GrantNo ratings yet
- CHAPTER 3: Toxic Effects of Drugs: Pharmacology Page 1Document1 pageCHAPTER 3: Toxic Effects of Drugs: Pharmacology Page 1Gabriel GonzagaNo ratings yet
- Data Sheet Dump ValveDocument2 pagesData Sheet Dump ValveVlade NaumovskiNo ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Torsion of Circular Shaft: Torque or Turning Moment or Twisting MomentDocument13 pagesTorsion of Circular Shaft: Torque or Turning Moment or Twisting Momentmahmudul adilNo ratings yet
- Trisyl Silica Gel: For Oils/Fats and Biofuel RefiningDocument4 pagesTrisyl Silica Gel: For Oils/Fats and Biofuel RefiningJosé Mauricio Bonilla TobónNo ratings yet
- BiostastisticDocument2 pagesBiostastisticاحمد ماجد زبنNo ratings yet
- Hydrostatic Testing ProcedureDocument21 pagesHydrostatic Testing ProcedureFerdie OSNo ratings yet
- Indian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaDocument13 pagesIndian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaPranjal MaluNo ratings yet
- Qualifications of Public Health NurseDocument2 pagesQualifications of Public Health Nursekaitlein_mdNo ratings yet
- Test A: Reading - Passage 1Document29 pagesTest A: Reading - Passage 1barishyayNo ratings yet
- Revised Provisional Selection List 30122022 1Document150 pagesRevised Provisional Selection List 30122022 1onlinetrash45No ratings yet
- Child Rearing Practices Articles India & ChinaDocument14 pagesChild Rearing Practices Articles India & ChinaGeorgiana GattinaNo ratings yet
- Smoke Stratification - Understanding the DynamicsDocument3 pagesSmoke Stratification - Understanding the DynamicsGagan UpadhyayNo ratings yet