You might also like
- Pericarditis Vs Mi: Internal Medicine: CvsDocument6 pagesPericarditis Vs Mi: Internal Medicine: CvsRojales FrancisNo ratings yet
- Ancient Norse RunesDocument19 pagesAncient Norse Runess_avgerNo ratings yet
- Pediatric Surgery Handbook For Residents and Medical Students (2017)Document428 pagesPediatric Surgery Handbook For Residents and Medical Students (2017)Oana Stefania Pintilii100% (1)
- Simple Note On Medical ApproachDocument7 pagesSimple Note On Medical ApproachSyaidatul NadwaNo ratings yet
- Family Safety HandbookDocument12 pagesFamily Safety HandbookAdib_dokterNo ratings yet
- Palmistry ExpertiseDocument65 pagesPalmistry ExpertisePawan AgrawalNo ratings yet
- Saint PatrickDocument1 pageSaint PatrickAnalía Cimolai0% (1)
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Eurocode 7 Section 7 Pile FoundationsDocument20 pagesEurocode 7 Section 7 Pile FoundationsHoNo ratings yet
- Pathophysiology of Acute Renal FailureDocument1 pagePathophysiology of Acute Renal FailureAina HaravataNo ratings yet
- List of Documents ISO 45001 Documentation Toolkit enDocument2 pagesList of Documents ISO 45001 Documentation Toolkit enCiciaSalatin100% (1)
- Mis C Clinical GuidelineDocument9 pagesMis C Clinical GuidelineasyqarNo ratings yet
- Drug StudyDocument30 pagesDrug StudyClaire MachicaNo ratings yet
- PATENT DUCTUS ARTERIOSUS Concept MapDocument2 pagesPATENT DUCTUS ARTERIOSUS Concept MapErika CadawanNo ratings yet
- Advanced Pathophysiology of Respiratory Failure and Other Underlying Resp Diseases With LegendDocument1 pageAdvanced Pathophysiology of Respiratory Failure and Other Underlying Resp Diseases With LegendTeanu Jose Gabrillo TamayoNo ratings yet
- Nursing Care Plan For HELLP SyndromeDocument17 pagesNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Simplified Modified Compression Field Theory For Calculating Shear Strength of Reinforced Concrete ElementsDocument11 pagesSimplified Modified Compression Field Theory For Calculating Shear Strength of Reinforced Concrete ElementsTooma David100% (1)
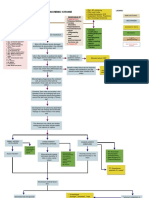
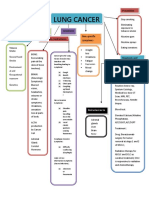
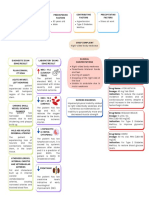
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- Colloquia Latina D Ooge PDFDocument104 pagesColloquia Latina D Ooge PDFHadaixx100% (1)
- Skill Checklist Applying An Extremity RestraintDocument2 pagesSkill Checklist Applying An Extremity RestraintAsep BageurNo ratings yet
- Metoprolol Drug StudyDocument4 pagesMetoprolol Drug StudyCrisha Ann Billones BacutaNo ratings yet
- 2nd - NCPDocument3 pages2nd - NCPjoidaNo ratings yet
- Acute Coronary Syndrome Workup Approach Considerations, Electrocardiography, Measurement of CK-MB LevelsDocument1 pageAcute Coronary Syndrome Workup Approach Considerations, Electrocardiography, Measurement of CK-MB LevelsfeaghNo ratings yet
- Name and Classification of DrugDocument3 pagesName and Classification of DrugAnicas, Ralph Joshua V.No ratings yet
- Feb DTRDocument3 pagesFeb DTRFeb NamiaNo ratings yet
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- Pediatric Shock StatesDocument32 pagesPediatric Shock StatessavasNo ratings yet
- Khorsand 2023 Not All Shock States Are Created EqualDocument25 pagesKhorsand 2023 Not All Shock States Are Created EqualLê Huy HoàngNo ratings yet
- 11 - Management Post Operative Low Cardiac Output SyndromeDocument46 pages11 - Management Post Operative Low Cardiac Output SyndromeNat SNo ratings yet
- AGLIAM, Dwight Jeremy D. BSN Ii-Intl GRP B 10/15/2018Document3 pagesAGLIAM, Dwight Jeremy D. BSN Ii-Intl GRP B 10/15/2018Dwight Jeremy DeVera AgliamNo ratings yet
- Onco ImDocument2 pagesOnco ImAlexandra BascoNo ratings yet
- RUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONDocument4 pagesRUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONGiselle EstoquiaNo ratings yet
- Name of Drug Dosage, Route, and Frequency Drug Action Indication Contraindication Adverse Effects Nursing ConsiderationsDocument3 pagesName of Drug Dosage, Route, and Frequency Drug Action Indication Contraindication Adverse Effects Nursing ConsiderationsAngelou MortosNo ratings yet
- Septic Shock For SiteDocument3 pagesSeptic Shock For Siteمحمد زينNo ratings yet
- Why LAMA Is Fundamental Treatment For COPD: Rudi DermawanDocument29 pagesWhy LAMA Is Fundamental Treatment For COPD: Rudi DermawanwitwiiwNo ratings yet
- Diagnostic Test and Laboratory TestDocument7 pagesDiagnostic Test and Laboratory TestampalNo ratings yet
- 3Document1 page3Ayesha Mae Baniaga DoctoleroNo ratings yet
- Ineffective Cerebral Tissue PerfusionDocument4 pagesIneffective Cerebral Tissue PerfusionLeticia ElricNo ratings yet
- Categorize The Treatment Options For Patients With Existing Medical ConditionDocument3 pagesCategorize The Treatment Options For Patients With Existing Medical ConditionMicah LatosaNo ratings yet
- Second Degree Av Block Type 1 (Mobitz I or Wenckebach)Document1 pageSecond Degree Av Block Type 1 (Mobitz I or Wenckebach)christine louise bernardoNo ratings yet
- Pediatric Shock (PICUCOURSE)Document40 pagesPediatric Shock (PICUCOURSE)surasuarezlopezNo ratings yet
- Surgery FADocument170 pagesSurgery FArafeekwalid551No ratings yet
- Co AmoxyclavDocument2 pagesCo AmoxyclavHaneulNo ratings yet
- Pediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedDocument40 pagesPediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedLa Ode RinaldiNo ratings yet
- Labs:: Pulmonary Renal Syndromes (PRS) Diffuse Alveolar HemorrhageDocument1 pageLabs:: Pulmonary Renal Syndromes (PRS) Diffuse Alveolar HemorrhageRonald MoralesNo ratings yet
- CeftriaxoneDocument3 pagesCeftriaxonejiloNo ratings yet
- Shock States in ChildrenDocument37 pagesShock States in ChildrenjuanitaNo ratings yet
- 8-Ecg in CovidsDocument35 pages8-Ecg in CovidsyandraNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- PathophysiologyDocument1 pagePathophysiologyArt Lemuel LotereñaNo ratings yet
- Case Chest Pain and DyspneaDocument1 pageCase Chest Pain and DyspneaVineeNo ratings yet
- Celecoxib Drug Study WWW RNpedia ComDocument3 pagesCelecoxib Drug Study WWW RNpedia ComAngelou MortosNo ratings yet
- Dopamine HydrochlorideDocument1 pageDopamine HydrochlorideJoannes SanchezNo ratings yet
- Estados de ChoqueDocument25 pagesEstados de ChoqueKarina Moreno PalacioNo ratings yet
- Bagian Ilmu Kesehatan Anak FK UNSRAT/ RSU. Prof. Dr. R.D. Kandou-ManadoDocument29 pagesBagian Ilmu Kesehatan Anak FK UNSRAT/ RSU. Prof. Dr. R.D. Kandou-ManadoAmarantoNo ratings yet
- Drug Study (Print3copiesDocument8 pagesDrug Study (Print3copiesPhylum ChordataNo ratings yet
- Pulmonary Edema: Mycobacterium Tuberculosis Patient BackgroundDocument1 pagePulmonary Edema: Mycobacterium Tuberculosis Patient BackgroundAubrey RecierdoNo ratings yet
- Drug Study Emergency DrugsDocument6 pagesDrug Study Emergency DrugsJhessa Curie PitaganNo ratings yet
- MIB 3 AnnotatedDocument78 pagesMIB 3 AnnotatedShekhar NandalNo ratings yet
- Fluid and Electrolyte ImbalanceDocument18 pagesFluid and Electrolyte ImbalanceKaren PiliNo ratings yet
- Shock in Covid PatientDocument21 pagesShock in Covid PatientGHALEB A. AlmekhlafiNo ratings yet
- 2019 LAMA For COPDDocument25 pages2019 LAMA For COPDdonnyNo ratings yet
- Updates On Pulmonary HypertensionDocument39 pagesUpdates On Pulmonary HypertensionZurlin DwirostantinNo ratings yet
- Jantung - Acute Heart FailureDocument32 pagesJantung - Acute Heart FailurefaradibaNo ratings yet
- Dilantin (Phenytoin) : Drug Classification Actions Side Effects ConsiderationsDocument4 pagesDilantin (Phenytoin) : Drug Classification Actions Side Effects ConsiderationsbreehaireNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Insulin Degludec PDFDocument19 pagesInsulin Degludec PDFLilisNo ratings yet
- Steiner2010 PDFDocument14 pagesSteiner2010 PDFLilisNo ratings yet
- Gestational AgeDocument7 pagesGestational AgeLilisNo ratings yet
- Denver II, Dev DelDocument11 pagesDenver II, Dev DelLilisNo ratings yet
- ZILLENIALSDocument1 pageZILLENIALSakhilNo ratings yet
- Everyday2 M8 S2 Student GrammarDocument2 pagesEveryday2 M8 S2 Student GrammarIvan MQNo ratings yet
- Test 1Document15 pagesTest 1Ngọc ÁnhNo ratings yet
- M M M MMMMMMMMMMMMMMMMM MMMMMM MMMM MMMMMMMMM MMMMMMMMMMMMMMMMMM M M ! MM MMM"MM M MMM#MMMM M MMDocument8 pagesM M M MMMMMMMMMMMMMMMMM MMMMMM MMMM MMMMMMMMM MMMMMMMMMMMMMMMMMM M M ! MM MMM"MM M MMM#MMMM M MMcool_vjk4b9No ratings yet
- Cambodia V ThailandDocument22 pagesCambodia V ThailandMaria QadirNo ratings yet
- Favour Emmanuel - Resume - Data AnalystDocument3 pagesFavour Emmanuel - Resume - Data AnalystEmmanuel FavourNo ratings yet
- Guidelines On Cadastral (2017 Edition Final)Document29 pagesGuidelines On Cadastral (2017 Edition Final)Olaitan RasheedNo ratings yet
- Leadership and FollowershipDocument10 pagesLeadership and FollowershipLawrence ConananNo ratings yet
- Coop Conference Proceeding (21-22aug 2022)Document585 pagesCoop Conference Proceeding (21-22aug 2022)oliviahuda75No ratings yet
- VLD 6000 AIS Airborne Transponder PDFDocument2 pagesVLD 6000 AIS Airborne Transponder PDFShin Ami IgamiNo ratings yet
- Alargamiento Del Complejo Gastronemio SoleoDocument8 pagesAlargamiento Del Complejo Gastronemio SoleoC Martin TraumatoNo ratings yet
- EC6802 Wireless Networks Important PART-A &B Questions With AnswersDocument21 pagesEC6802 Wireless Networks Important PART-A &B Questions With AnswersohmshankarNo ratings yet
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- Punk Science - Inside The Mind of GodDocument3 pagesPunk Science - Inside The Mind of GodRobert Garcia0% (2)
- Sampel Cylinder 1 (MS-01-177) R0Document6 pagesSampel Cylinder 1 (MS-01-177) R0herysyam1980No ratings yet
- Impact TestDocument11 pagesImpact TestMohsin AbbasNo ratings yet
- Compresor Atlas Copco GA30Document16 pagesCompresor Atlas Copco GA30Florin Maria Chirila100% (1)
- Parts of Speech (Updated) - 1Document33 pagesParts of Speech (Updated) - 1Ramzan MemonNo ratings yet
- uC-GUI UserDocument920 pagesuC-GUI Userpmih1No ratings yet