You might also like
- 2019 LAMA For COPDDocument25 pages2019 LAMA For COPDdonnyNo ratings yet
- Dr. Sudarto Sppd's FileDocument22 pagesDr. Sudarto Sppd's FileVindy CesarianaNo ratings yet
- Current Pharmacological Treatment of Copd: Zen Ahmad Medical Faculty, Sriwijaya UniversityDocument32 pagesCurrent Pharmacological Treatment of Copd: Zen Ahmad Medical Faculty, Sriwijaya Universitylingga gumelarNo ratings yet
- GOLD 2017 Major Revision: Summary of Key Changes: Respiratory FranchiseDocument17 pagesGOLD 2017 Major Revision: Summary of Key Changes: Respiratory FranchiseudjkwNo ratings yet
- GOLD 2017 Major Revision: Summary of Key Changes: Amira Permatasari TariganDocument22 pagesGOLD 2017 Major Revision: Summary of Key Changes: Amira Permatasari Tariganpra375No ratings yet
- COPD Classification, Phenotypes and Risk Assesment J Thorac Dis 2019Document6 pagesCOPD Classification, Phenotypes and Risk Assesment J Thorac Dis 2019Claudio Rafael Salazar MNo ratings yet
- Gold Guidlines 2023 1Document24 pagesGold Guidlines 2023 1api-649066372No ratings yet
- ABC of COPDDocument51 pagesABC of COPDAmit HalderNo ratings yet
- Corona Virus - 19: A Case PresentationDocument25 pagesCorona Virus - 19: A Case PresentationYessamin Paith RoderosNo ratings yet
- Patofisiologi Luka BakarDocument34 pagesPatofisiologi Luka BakarRut HutagaolNo ratings yet
- Acep Evidencecare Covid19severitytoolDocument3 pagesAcep Evidencecare Covid19severitytoolShariq IqbalNo ratings yet
- Neumologia First AidDocument6 pagesNeumologia First AidMAINo ratings yet
- COPD NEW GuidelinesDocument45 pagesCOPD NEW GuidelinesMuhammad HaneefNo ratings yet
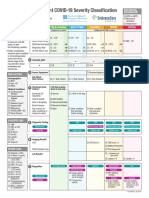
- Emergency Department COVID-19 Severity ClassificationDocument3 pagesEmergency Department COVID-19 Severity ClassificationAsti YumnaNo ratings yet
- REVISED COVID-19 TREATMENT PROTOCOL - Version 3Document17 pagesREVISED COVID-19 TREATMENT PROTOCOL - Version 3abhishekNo ratings yet
- Pneumonia Pathway Final 2010 Rev4Document7 pagesPneumonia Pathway Final 2010 Rev4lyuen600No ratings yet
- NPO Slides 110Document52 pagesNPO Slides 110Yaya ManNo ratings yet
- Hepatopulmonary Syndrome (HPS)Document2 pagesHepatopulmonary Syndrome (HPS)Cristian urrutia castilloNo ratings yet
- 04-Role of Echo in Pulm Hypertion N EmbolismDocument57 pages04-Role of Echo in Pulm Hypertion N EmbolismSiska Istanah Wong SintingNo ratings yet
- 2019 Copd OutpatientsDocument61 pages2019 Copd OutpatientsArshamNo ratings yet
- 1.2 Clinical SyndromesDocument14 pages1.2 Clinical SyndromesDan FabrosNo ratings yet
- Copd PathDocument2 pagesCopd Pathnursing concept maps100% (2)
- Morning Report: Physician in ChargeDocument29 pagesMorning Report: Physician in ChargeWilujeng AnggrainiNo ratings yet
- Inhalation Injury PresentationDocument51 pagesInhalation Injury PresentationFilologus Siwabessy100% (1)
- Pediatric Shock StatesDocument32 pagesPediatric Shock StatessavasNo ratings yet
- Case 1: Health Maintenance in GeneralDocument44 pagesCase 1: Health Maintenance in GeneralJoshuaNo ratings yet
- COPD - Chronic Objective Pulmonary DiseaseDocument22 pagesCOPD - Chronic Objective Pulmonary Diseasefayrouz fathiNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Muhammad IlyasDocument32 pagesChronic Obstructive Pulmonary Disease (COPD) : Muhammad IlyasSyarifah MariaNo ratings yet
- Tnicu Case PresentationDocument45 pagesTnicu Case Presentationapi-690342013No ratings yet
- Acute Respiratory Failure Type Ii, Cap HR: de La Salle Health Sciences Institute College of Nursing Nursing Case PlanDocument9 pagesAcute Respiratory Failure Type Ii, Cap HR: de La Salle Health Sciences Institute College of Nursing Nursing Case PlanLuigi ArenasNo ratings yet
- Cute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraDocument40 pagesCute Respiratory Distress Syndrome Ards: Guide - DR - Shiv.S.Sharma - Dr.Y. JamraandenaNo ratings yet
- Oxygen - Therapy 2)Document33 pagesOxygen - Therapy 2)Bryson MwengeNo ratings yet
- Jantung - Acute Heart FailureDocument32 pagesJantung - Acute Heart FailurefaradibaNo ratings yet
- Septic Shock For SiteDocument3 pagesSeptic Shock For Siteمحمد زينNo ratings yet
- Respiratory Physiology & Respiratory Function During AnesthesiaDocument105 pagesRespiratory Physiology & Respiratory Function During Anesthesiahouman726254085100% (2)
- Copd FK Unhas 2015Document28 pagesCopd FK Unhas 2015Muhammad Nur DelaphanEnamNo ratings yet
- Persiapan Triage Primary Survey Resusitasi Adjunct Primary: By: RiswanDocument7 pagesPersiapan Triage Primary Survey Resusitasi Adjunct Primary: By: Riswanrudi mirinoNo ratings yet
- MedCon Template - Melena+DOC+Septic ConditionDocument26 pagesMedCon Template - Melena+DOC+Septic ConditionPramudia DeniNo ratings yet
- 006 COPD - Lecture StudentsDocument52 pages006 COPD - Lecture Studentszyz6639No ratings yet
- ARDS Patopi FinaleDocument1 pageARDS Patopi FinaleCuttie Anne GalangNo ratings yet
- Sos Pomr SatitiDocument30 pagesSos Pomr SatitiIka AyuNo ratings yet
- A Case Study On AsthmaDocument38 pagesA Case Study On AsthmaMark Tristan AsuncionNo ratings yet
- DR Susanthy SP.P (K)Document52 pagesDR Susanthy SP.P (K)dadankNo ratings yet
- MR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHDocument24 pagesMR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHIka AyuNo ratings yet
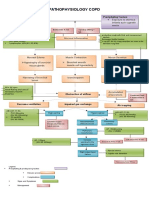
- COPD PATHOPHYSIOLOGY DiagramDocument2 pagesCOPD PATHOPHYSIOLOGY Diagramcris_198893% (15)
- ARDSDocument82 pagesARDSfeniNo ratings yet
- RetrieveDocument18 pagesRetrieveAleCosentinoNo ratings yet
- City Hospitals Sunderland A&E Department: Information Card PackDocument47 pagesCity Hospitals Sunderland A&E Department: Information Card PackMulki HakamNo ratings yet
- E Poster On CopdDocument1 pageE Poster On CopdSarithaRajeshNo ratings yet
- Complete Blood CountDocument5 pagesComplete Blood CountYessaminNo ratings yet
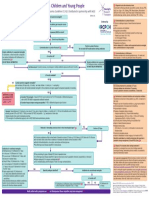
- Incorporates NICE Bacterial Meningitis and Meningococcal Septicaemia Guideline CG102. Distributed in Partnership With NICEDocument1 pageIncorporates NICE Bacterial Meningitis and Meningococcal Septicaemia Guideline CG102. Distributed in Partnership With NICELilisNo ratings yet
- Respirology Division, Department of Child Health, Udayana University Medical School/Sanglah Hospital, DenpasarDocument59 pagesRespirology Division, Department of Child Health, Udayana University Medical School/Sanglah Hospital, DenpasarWita FitriyaniNo ratings yet
- Pediatric Shock (PICUCOURSE)Document40 pagesPediatric Shock (PICUCOURSE)surasuarezlopezNo ratings yet
- Pediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedDocument40 pagesPediatric Shock: Dr. Lilia Dewiyanti, Spa, MsimedLa Ode RinaldiNo ratings yet
- Ppok 2023 PDFDocument33 pagesPpok 2023 PDFBagas Trikuncoro BawonoNo ratings yet
- Morning Report: Date: 6 April 2021Document17 pagesMorning Report: Date: 6 April 2021Adinda DianNo ratings yet
- Clinical Criteria For Early Diagnosis of Ventilator Associated Pneumonia in Pediatric Intensive Care Unit (Picu) DR Soetomo General HospitalDocument11 pagesClinical Criteria For Early Diagnosis of Ventilator Associated Pneumonia in Pediatric Intensive Care Unit (Picu) DR Soetomo General HospitalTor JaNo ratings yet
- Materi DrbambangDocument33 pagesMateri DrbambangWiedya kristiantiNo ratings yet
- MR 20 May Sob Copd FixDocument30 pagesMR 20 May Sob Copd FixWenNy RupiNaNo ratings yet
- Update On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007Document38 pagesUpdate On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007witwiiwNo ratings yet
- J. Antimicrob. Chemother.-2011-Rørtveit-1360-4 PDFDocument5 pagesJ. Antimicrob. Chemother.-2011-Rørtveit-1360-4 PDFwitwiiwNo ratings yet
- 1Document1 page1witwiiwNo ratings yet
- Appi Ajp 2014 13111517Document11 pagesAppi Ajp 2014 13111517witwiiwNo ratings yet
- Hamilton D ScoringDocument1 pageHamilton D ScoringJoezerk Jhon BielNo ratings yet
- Update On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007Document38 pagesUpdate On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007witwiiwNo ratings yet
- Jurnal TB Kutis 1Document14 pagesJurnal TB Kutis 1witwiiwNo ratings yet
- Appi Ajp 2014 13111517Document11 pagesAppi Ajp 2014 13111517witwiiwNo ratings yet
- A Users Guide To The 2016 Surviving Sepsis.1Document5 pagesA Users Guide To The 2016 Surviving Sepsis.1zico yusuf alfariziNo ratings yet
- Jadwal Periode Maret 2017Document28 pagesJadwal Periode Maret 2017Muhammad BasriNo ratings yet
- Jadwal Ikut Visit Rumah Sakit KlenderDocument1 pageJadwal Ikut Visit Rumah Sakit KlenderwitwiiwNo ratings yet
- JurnalDocument10 pagesJurnalwitwiiwNo ratings yet
- Comparison Dopamin Dan NorepinefrinDocument11 pagesComparison Dopamin Dan NorepinefrinnadyajondriNo ratings yet
- Microbiologic Methods in The DiagnosticsDocument7 pagesMicrobiologic Methods in The DiagnosticswitwiiwNo ratings yet
- JurnalDocument16 pagesJurnalwitwiiwNo ratings yet
- JurnalDocument10 pagesJurnalwitwiiwNo ratings yet
- Patient and Parent-Reported Signs and Symptoms For Group A Streptococcal PharyngitisDocument9 pagesPatient and Parent-Reported Signs and Symptoms For Group A Streptococcal PharyngitiswitwiiwNo ratings yet
- E20154608 FullDocument10 pagesE20154608 FullwitwiiwNo ratings yet
- E20154547 FullDocument11 pagesE20154547 FullwitwiiwNo ratings yet
- Iron-Refractory Iron Deficiency Anemia May Not Lead To Neurocognitive Dysfunction: A Case ReportDocument6 pagesIron-Refractory Iron Deficiency Anemia May Not Lead To Neurocognitive Dysfunction: A Case ReportwitwiiwNo ratings yet
- Interpretacion Curso Cat CoolantDocument39 pagesInterpretacion Curso Cat Coolanthouston machacaNo ratings yet
- E 23 Fuel System Schaffer 4350ZDocument3 pagesE 23 Fuel System Schaffer 4350ZSergeyNo ratings yet
- Cord Care Evaluation ToolDocument1 pageCord Care Evaluation ToolCherry AnnNo ratings yet
- Substation Off Line and Hot Line CommissioningDocument3 pagesSubstation Off Line and Hot Line CommissioningMohammad JawadNo ratings yet
- Coronavirus Reported SpeechDocument1 pageCoronavirus Reported SpeechGabiZ - Kalifato SurNo ratings yet
- Request For New Tax DeclarationDocument2 pagesRequest For New Tax DeclarationAsterio MagootNo ratings yet
- Aerobic ActivitiesExercises PDFDocument14 pagesAerobic ActivitiesExercises PDFPalma, Arrabela M.No ratings yet
- Octavia Tour BrochureDocument9 pagesOctavia Tour BrochureOvidiuIONo ratings yet
- Oedipus SummaryDocument1 pageOedipus SummaryReynold FrancoNo ratings yet
- (Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Document589 pages(Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Andi sutandi100% (1)
- 1.ar-315 BC&BL Lighting & IlluminationDocument28 pages1.ar-315 BC&BL Lighting & IlluminationUsha Sri GNo ratings yet
- Case Study 2Document3 pagesCase Study 2Mrinal BhandariNo ratings yet
- Microcosmic Orbit Breath Awareness and Meditation Process: For Enhanced Reproductive Health, An Ancient Taoist MeditationDocument1 pageMicrocosmic Orbit Breath Awareness and Meditation Process: For Enhanced Reproductive Health, An Ancient Taoist MeditationSaimon S.M.No ratings yet
- Effects of Career Plateau On Job Satisfaction and MotivationDocument105 pagesEffects of Career Plateau On Job Satisfaction and Motivationalanwil100% (1)
- Know Your Customer BrochureDocument4 pagesKnow Your Customer BrochureTEL COMENo ratings yet
- PERDEV FIRST Periodical Test (2022)Document5 pagesPERDEV FIRST Periodical Test (2022)jeadryl LinatocNo ratings yet
- Chapter 10 Fitness Training PrinciplesDocument80 pagesChapter 10 Fitness Training Principlesapi-115744109No ratings yet
- 3RD Summative Exam in Science 6Document6 pages3RD Summative Exam in Science 6Maricris Palermo SancioNo ratings yet
- Substation Basic PDFDocument6 pagesSubstation Basic PDFSaraswatapalitNo ratings yet
- Static Var CompensatorDocument12 pagesStatic Var CompensatorBengal Gaming100% (1)
- BSNL KERALA Executives and Non Executives Health Insurance Policy 2021-22Document3 pagesBSNL KERALA Executives and Non Executives Health Insurance Policy 2021-22Vikramjeet MannNo ratings yet
- Calinescu2017 PDFDocument38 pagesCalinescu2017 PDFElizabeth UrrutiaNo ratings yet
- CHEM 333: Lab Experiment 5: Introduction To Chromatography : Thin Layer and High Performance Liquid ChromatographyDocument5 pagesCHEM 333: Lab Experiment 5: Introduction To Chromatography : Thin Layer and High Performance Liquid ChromatographymanurihimalshaNo ratings yet
- Korean Wellhead KWM-2014-Revision0Document20 pagesKorean Wellhead KWM-2014-Revision0DrakkarNo ratings yet
- Tutorial SessionDocument5 pagesTutorial SessionKhánh LinhNo ratings yet
- One Village One Product Movement in Laos: AbstractDocument5 pagesOne Village One Product Movement in Laos: Abstractoeleong19699685No ratings yet
- Method For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (Document8 pagesMethod For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (DiptiNo ratings yet
- Problems Associated With The Use of Compaction Grout For SinkholeDocument4 pagesProblems Associated With The Use of Compaction Grout For SinkholeVetriselvan ArumugamNo ratings yet
- Key MechanicalDocument72 pagesKey MechanicalDasuki FahmiNo ratings yet
- 12 29 11editionDocument27 pages12 29 11editionSan Mateo Daily JournalNo ratings yet