You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Working and Non-Working University Students Anxiety, Depression, and Grade Point AverageDocument12 pagesWorking and Non-Working University Students Anxiety, Depression, and Grade Point Averagejanettst2No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Treating University Students With Social Phobia and Public Speaking FearsDocument12 pagesTreating University Students With Social Phobia and Public Speaking Fearsjanettst2No ratings yet
- Rural-Urban Background, Depression and Suicidal Ideation in Chinese College StudentsDocument7 pagesRural-Urban Background, Depression and Suicidal Ideation in Chinese College Studentsjanettst2No ratings yet
- Parental Attachment, Cognitive Working Models, and Depression Among African-American Collede StudentsDocument14 pagesParental Attachment, Cognitive Working Models, and Depression Among African-American Collede Studentsjanettst2No ratings yet
- The Role of Mental Health in Primary Prevention of Sexual and Gender Based ViolenceDocument6 pagesThe Role of Mental Health in Primary Prevention of Sexual and Gender Based Violencejanettst2No ratings yet
- The Thinner The Better. Competitiveness Depression and BodyDocument10 pagesThe Thinner The Better. Competitiveness Depression and Bodyjanettst2No ratings yet
- Depression-Focused Interpersonal CounsellingDocument10 pagesDepression-Focused Interpersonal Counsellingjanettst2No ratings yet
- Gender Differences in The Relationship Between Emotional Regulation and Depressive SymptomsDocument17 pagesGender Differences in The Relationship Between Emotional Regulation and Depressive Symptomsjanettst2No ratings yet
- Cognitive Techniques As A Means For Facilitating Supervisee DevelopmentDocument15 pagesCognitive Techniques As A Means For Facilitating Supervisee Developmentjanettst2No ratings yet
- How To Find FramesDocument22 pagesHow To Find Framesjanettst2No ratings yet
- Self-Regulation and Mechanisms of Action in Psychotherapy. A Theory-Based Translational Perspective PDFDocument12 pagesSelf-Regulation and Mechanisms of Action in Psychotherapy. A Theory-Based Translational Perspective PDFjanettst2No ratings yet
- Beliefs of Professional CounselorsDocument10 pagesBeliefs of Professional Counselorsjanettst2No ratings yet
- Tryptophan and Serotonin in Blood and Platelets of Depressed Patients. Effect of An Antidepressant TreatmenDocument8 pagesTryptophan and Serotonin in Blood and Platelets of Depressed Patients. Effect of An Antidepressant Treatmenjanettst2No ratings yet
- Impact of Childhood Trauma On The Outcomes of A Perinatal Depression TrialDocument12 pagesImpact of Childhood Trauma On The Outcomes of A Perinatal Depression TrialValeriaNo ratings yet
- Effect of Acupuncture Treatment On Depression. Correlation Between Psychological Outcomes and Salivary Cortisol LevelsDocument6 pagesEffect of Acupuncture Treatment On Depression. Correlation Between Psychological Outcomes and Salivary Cortisol Levelsjanettst2No ratings yet
- Beyond Depression. Toward A Process-Based Approach To Research, Diagnosis, and Treatment.Document26 pagesBeyond Depression. Toward A Process-Based Approach To Research, Diagnosis, and Treatment.janettst2No ratings yet
- Cognitive Behavioral Psychotherapy For DepressionDocument5 pagesCognitive Behavioral Psychotherapy For Depressionjanettst2No ratings yet
- Cognitive-Personality Subtypes of Depression - Theories in Search of Disorder PDFDocument20 pagesCognitive-Personality Subtypes of Depression - Theories in Search of Disorder PDFjanettst2No ratings yet
- Behavioural Factors Asociated With Symptom Outcome in A Primary CareDocument10 pagesBehavioural Factors Asociated With Symptom Outcome in A Primary Carejanettst2No ratings yet
- The Importance of Asking Patients-The Potential Value of Patient Report of Brief Interventions AddDocument4 pagesThe Importance of Asking Patients-The Potential Value of Patient Report of Brief Interventions Addjanettst2No ratings yet
- Using Attachment Theory To Understand The Treatment of Adult Depression PDFDocument13 pagesUsing Attachment Theory To Understand The Treatment of Adult Depression PDFjanettst2No ratings yet
- Beyond Depression. Toward A Process-Based Approach To Research, Diagnosis, and Treatment.Document26 pagesBeyond Depression. Toward A Process-Based Approach To Research, Diagnosis, and Treatment.janettst2No ratings yet
- Narrative and Narrative Enquiry in Health and Social SciencesDocument13 pagesNarrative and Narrative Enquiry in Health and Social Sciencesjanettst2No ratings yet
- Evaluating The Effectiveness of A Scholl-Based CounsellingDocument14 pagesEvaluating The Effectiveness of A Scholl-Based Counsellingjanettst2100% (1)
- Tryptophan and Serotonin in Blood and Platelets of Depressed Patients. Effect of An Antidepressant TreatmenDocument8 pagesTryptophan and Serotonin in Blood and Platelets of Depressed Patients. Effect of An Antidepressant Treatmenjanettst2No ratings yet
- Various Forms of DepressionDocument11 pagesVarious Forms of Depressionjanettst2No ratings yet
- An Introduction To The Biographical Narrative Interpretive MethodDocument6 pagesAn Introduction To The Biographical Narrative Interpretive Methodjanettst2No ratings yet
- Impact of Childhood Trauma On The Outcomes of A Perinatal Depression TrialDocument12 pagesImpact of Childhood Trauma On The Outcomes of A Perinatal Depression TrialValeriaNo ratings yet
- The Phenomenology of Intersubjectivity in Bipolar Disorder and SquizophreniaDocument9 pagesThe Phenomenology of Intersubjectivity in Bipolar Disorder and Squizophreniajanettst2No ratings yet
- Banner Page: IHCP Updates Reimbursement Rate For HCPCS Code C9803, Mass Adjusts Claims That Paid IncorrectlyDocument8 pagesBanner Page: IHCP Updates Reimbursement Rate For HCPCS Code C9803, Mass Adjusts Claims That Paid IncorrectlyIndiana Family to FamilyNo ratings yet
- Middy CCTV Case StudyDocument2 pagesMiddy CCTV Case StudyLucas StacheckiNo ratings yet
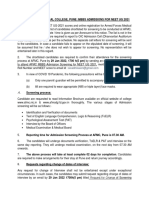
- AFMC MBBS Admissions Screening Dates for NEET UG 2021Document33 pagesAFMC MBBS Admissions Screening Dates for NEET UG 2021robert hookeNo ratings yet
- Continual Improvement ProcedureDocument6 pagesContinual Improvement ProcedureRonald Sarillana100% (1)
- HISTORIA DE LA ORTODONCIADocument9 pagesHISTORIA DE LA ORTODONCIAcarmonao.carina94No ratings yet
- Telli Health 1 of 2Document15 pagesTelli Health 1 of 2Ayush KumarNo ratings yet
- Figure of Speech QuizDocument1 pageFigure of Speech QuizManal SalamehNo ratings yet
- RhetoricDocument32 pagesRhetoricDian ValerieNo ratings yet
- CR10958 AttachmentDocument25 pagesCR10958 AttachmentPaulo MoraisNo ratings yet
- Mba HRM 3 AprDocument13 pagesMba HRM 3 AprFarhaNo ratings yet
- Handling Compressed Gas CylindersDocument103 pagesHandling Compressed Gas CylinderstorolsoNo ratings yet
- Adime 2Document13 pagesAdime 2api-496164982No ratings yet
- Ashgate - Landscape Professional Practice PDFDocument281 pagesAshgate - Landscape Professional Practice PDFyondaimethunderNo ratings yet
- NSTP Program GuideDocument19 pagesNSTP Program GuideLester ElipseNo ratings yet
- Online Visa Application for Business & TourismDocument5 pagesOnline Visa Application for Business & TourismdoomsayeropethNo ratings yet
- Basketball Court Construction SampleDocument17 pagesBasketball Court Construction Sampleashenafi girmaNo ratings yet
- Analisis Sifat Mirip Obat Prediksi ADMET Dan PenamDocument14 pagesAnalisis Sifat Mirip Obat Prediksi ADMET Dan PenamFrisma DheanovaNo ratings yet
- MDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Document13 pagesMDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Clarabelle Mae Dela RosaNo ratings yet
- Bihar Jharkhand Lab ScrapDocument27 pagesBihar Jharkhand Lab ScrapOFC accountNo ratings yet
- HMEF5063 Guidance and Counseling - Caug16 (Bookmark) PDFDocument188 pagesHMEF5063 Guidance and Counseling - Caug16 (Bookmark) PDFMarilyn Richard100% (1)
- Anatomy / Physio of The EarDocument58 pagesAnatomy / Physio of The EarRA100% (1)
- Alu DrossDocument10 pagesAlu DrossfahmiNo ratings yet
- Annamalai University Faculty of Engineering and TechnologyDocument46 pagesAnnamalai University Faculty of Engineering and TechnologyPrasad PNo ratings yet
- Emergency Management of Severe Burns (EMSB) : Dr. Amrin Amir LubisDocument17 pagesEmergency Management of Severe Burns (EMSB) : Dr. Amrin Amir Lubisamrin amir lubisNo ratings yet
- Module 1Document26 pagesModule 1priya malikNo ratings yet
- Intrusion Detection System Method StatementDocument30 pagesIntrusion Detection System Method StatementNideesh RobertNo ratings yet
- LOTODocument31 pagesLOTORanganayaki Tirumale Srinivasa RangacharNo ratings yet
- Csec Physics Sbaform ModerationDocument1 pageCsec Physics Sbaform Moderationapi-248240402No ratings yet
- Profiles in Diversity Journal - Sep/Oct 2007Document201 pagesProfiles in Diversity Journal - Sep/Oct 2007Profiles in Diversity JournalNo ratings yet
- A. Gudang Farmasi 2023 (Feni Dwi) UpdateDocument882 pagesA. Gudang Farmasi 2023 (Feni Dwi) UpdatehefikurniasariNo ratings yet