You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- You Are Here: Skip To Main ContentDocument5 pagesYou Are Here: Skip To Main ContentRumela Ganguly ChakrabortyNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
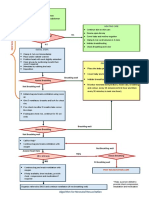
- Basic NRP Algorithm EnglishDocument1 pageBasic NRP Algorithm EnglishRumela Ganguly ChakrabortyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Extended Mop Up Notice 1Document1 pageExtended Mop Up Notice 1Rumela Ganguly ChakrabortyNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Curriculum Vitae: NAME: Rumela Chakraborty MOBILE NO: 8617254440 E-Mail IdDocument6 pagesCurriculum Vitae: NAME: Rumela Chakraborty MOBILE NO: 8617254440 E-Mail IdRumela Ganguly ChakrabortyNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Health PDFDocument94 pagesHealth PDFMayom MabuongNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Independent Nurse Practitioner 2Document8 pagesIndependent Nurse Practitioner 2Krishnaveni Murugesh100% (3)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 7 Essential Nursing Care of The Critically Ill PatientDocument24 pages7 Essential Nursing Care of The Critically Ill PatientAyah TiarAzkaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 100 PijlsDocument118 pages100 PijlsSinisa RisticNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Nurses NoteDocument1 pageNurses NoteRumela Ganguly ChakrabortyNo ratings yet
- 3 11 38 983Document5 pages3 11 38 983Rumela Ganguly ChakrabortyNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Quality of Life After Open-Heart Surgery in Patients Over 75 Years OldDocument4 pagesQuality of Life After Open-Heart Surgery in Patients Over 75 Years OldRumela Ganguly ChakrabortyNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cardiac Surgery in Octogenarians: Peri-Operative Outcome and Long-Term ResultsDocument9 pagesCardiac Surgery in Octogenarians: Peri-Operative Outcome and Long-Term ResultsRumela Ganguly ChakrabortyNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Article 6Document4 pagesArticle 6Rumela Ganguly ChakrabortyNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 5 TarangDocument8 pages5 TarangRumela Ganguly ChakrabortyNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- WHO Report - April 23Document12 pagesWHO Report - April 23CityNewsTorontoNo ratings yet
- MSC NursingDocument8 pagesMSC NursingRumela Ganguly ChakrabortyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Acute Myocardial Infarction Survivors Experiences: A Qualitative Literature ReviewDocument10 pagesAcute Myocardial Infarction Survivors Experiences: A Qualitative Literature ReviewRumela Ganguly ChakrabortyNo ratings yet
- Annotated Bibliograhy: Submitted ToDocument4 pagesAnnotated Bibliograhy: Submitted ToRumela Ganguly ChakrabortyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Home About Us Editorial Board Search Ahead of Print Current Issue Archives Submit ArticleDocument11 pagesHome About Us Editorial Board Search Ahead of Print Current Issue Archives Submit ArticleRumela Ganguly ChakrabortyNo ratings yet
- 1427 - Rana Kachouh Nursing Process HammoudDocument54 pages1427 - Rana Kachouh Nursing Process HammoudRumela Ganguly ChakrabortyNo ratings yet
- 2006 Inaccurate Risk PerceptionDocument5 pages2006 Inaccurate Risk PerceptionRumela Ganguly ChakrabortyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bitton2013 PDFDocument21 pagesBitton2013 PDFVirgo WNo ratings yet
- Quality of Life After Cardiac Surgery: Underresearched ResearchDocument5 pagesQuality of Life After Cardiac Surgery: Underresearched ResearchRumela Ganguly ChakrabortyNo ratings yet
- 05 N501 28766Document23 pages05 N501 28766Rumela Ganguly ChakrabortyNo ratings yet
- Article 6Document4 pagesArticle 6Rumela Ganguly ChakrabortyNo ratings yet
- Emerging Role of District Level Nursing PersonnelDocument9 pagesEmerging Role of District Level Nursing PersonnelRumela Ganguly ChakrabortyNo ratings yet
- Case Presentation On AmputationDocument18 pagesCase Presentation On AmputationRumela Ganguly ChakrabortyNo ratings yet
- 2008 CCModule 3Document13 pages2008 CCModule 3Jaymee GasparNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Knowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionDocument49 pagesKnowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionRumela Ganguly ChakrabortyNo ratings yet
- Eisen 1998Document7 pagesEisen 1998Angela EnacheNo ratings yet
- 8604 Assignment 1Document20 pages8604 Assignment 1Ruhaan TanvirNo ratings yet
- Satisfaction With Life Scale: ReferenceDocument8 pagesSatisfaction With Life Scale: ReferencetotalnocoolNo ratings yet
- Customer Satisfaction BarometerDocument17 pagesCustomer Satisfaction Barometershahmed999No ratings yet
- Avey Et Al. (2009 Psychological Ownership Scale)Document19 pagesAvey Et Al. (2009 Psychological Ownership Scale)Abdullah Sultan100% (1)
- Session 9 Human Resource ManagementDocument42 pagesSession 9 Human Resource ManagementUmair ShahNo ratings yet
- Simulation of A Model Tank Gunnery Test PDFDocument84 pagesSimulation of A Model Tank Gunnery Test PDFAlexanderPetrovNo ratings yet
- Authentic Assessmen T in The ClassroomDocument56 pagesAuthentic Assessmen T in The ClassroomJenjen GammadNo ratings yet
- Sodhi's Attitude Scales (SAS)Document23 pagesSodhi's Attitude Scales (SAS)Ananya Sharma50% (2)
- Lesson 5.1 - ValidityDocument14 pagesLesson 5.1 - Validitygwen awasNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Self-Perception Profile For Adolescents PDFDocument50 pagesSelf-Perception Profile For Adolescents PDFIonela MilitaruNo ratings yet
- تست بانك منهجيه مهم جدا PDFDocument59 pagesتست بانك منهجيه مهم جدا PDFDema Farrayh100% (1)
- 4 Reliability ValidityDocument47 pages4 Reliability ValidityMin MinNo ratings yet
- Appeals in AdvertisementDocument12 pagesAppeals in AdvertisementYash Gupta100% (1)
- Indices To Assess Malocclusions in Patients With Cleft Lip and Palate PDFDocument11 pagesIndices To Assess Malocclusions in Patients With Cleft Lip and Palate PDFIsharajini Prasadika Subhashni GamageNo ratings yet
- Language TestingDocument132 pagesLanguage TestingKKO TGINo ratings yet
- Quality-Of-Life Measurement in Chronic Heart Failure: Do We Take Account of The Patient Perspective?Document11 pagesQuality-Of-Life Measurement in Chronic Heart Failure: Do We Take Account of The Patient Perspective?Gaoudam NatarajanNo ratings yet
- 4708 17202 1 PBDocument16 pages4708 17202 1 PBThảo QuyênNo ratings yet
- StockWatson 3e EmpiricalExerciseSolutionsDocument65 pagesStockWatson 3e EmpiricalExerciseSolutionsmarkus67% (6)
- Motional Intelligence in Teams: Development and Initial Validation of The Short Version of The Workgroup Emotional Intelligence Profile (WEIP-S)Document19 pagesMotional Intelligence in Teams: Development and Initial Validation of The Short Version of The Workgroup Emotional Intelligence Profile (WEIP-S)Small Leaf NguyễnNo ratings yet
- Educ 6BDocument15 pagesEduc 6BDex LicongNo ratings yet
- Elbow MethodDocument18 pagesElbow MethodOsmar SalvadorNo ratings yet
- Amultiple itemscaleformeasurigSCBDocument27 pagesAmultiple itemscaleformeasurigSCBDoni StiadiNo ratings yet
- PDF Melese Alemayehu Research ProposalDocument28 pagesPDF Melese Alemayehu Research Proposalmelu alexsNo ratings yet
- Doc-20240128-Wa0002 240128 203620Document94 pagesDoc-20240128-Wa0002 240128 203620Malak BenkaddourNo ratings yet
- Examining The Effects of Servant Leadership On Life SatisfactionDocument17 pagesExamining The Effects of Servant Leadership On Life SatisfactionPhuoc NguyenNo ratings yet
- Chapter3 Research MethodologyDocument30 pagesChapter3 Research MethodologyJoey DeonNo ratings yet
- Accepted ManuscriptDocument38 pagesAccepted ManuscriptrobertNo ratings yet
- AsiaTEFL2023Proceedings 20240115 1Document1,418 pagesAsiaTEFL2023Proceedings 20240115 1bonik.kerrinNo ratings yet
- Sewhareg GetenetDocument121 pagesSewhareg GetenetIsaan Naafta'eNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (393)