You might also like
- Instant Assessments for Data Tracking, Grade 4: MathFrom EverandInstant Assessments for Data Tracking, Grade 4: MathRating: 5 out of 5 stars5/5 (2)
- Never Can Say Goodbye Katherine JacksonDocument73 pagesNever Can Say Goodbye Katherine Jacksonalina28sept100% (5)
- EMAM Baldwin Manufacturers Cross-Reference Form560 PDFDocument908 pagesEMAM Baldwin Manufacturers Cross-Reference Form560 PDFDede KurniawanNo ratings yet
- Walk Hand in Hand 1 4 PDFDocument4 pagesWalk Hand in Hand 1 4 PDFLden BuenaventuraNo ratings yet
- Thera Bank - ProjectDocument34 pagesThera Bank - Projectbhumika singh100% (4)
- Service Manual Measuring CellsDocument545 pagesService Manual Measuring CellsDavid EguezNo ratings yet
- Laurel VS GarciaDocument2 pagesLaurel VS GarciaRon AceNo ratings yet
- Foreign Policy During Mahathir EraDocument7 pagesForeign Policy During Mahathir EraMuhamad Efendy Jamhar0% (1)
- Independent Nurse Practitioner 2Document8 pagesIndependent Nurse Practitioner 2Krishnaveni Murugesh100% (3)
- Case Presentation On AmputationDocument18 pagesCase Presentation On AmputationRumela Ganguly ChakrabortyNo ratings yet
- Top Down Proteomics Using Online Polymer Reversed Phase (PLRP) Nanocapillary-LC Coupled Fourier Transform Mass SpectrometryDocument1 pageTop Down Proteomics Using Online Polymer Reversed Phase (PLRP) Nanocapillary-LC Coupled Fourier Transform Mass Spectrometryapi-26001949No ratings yet
- H Typre Coupling Equivalent To N-EUPEX B Type Ender CouplingDocument1 pageH Typre Coupling Equivalent To N-EUPEX B Type Ender Couplingelect aksNo ratings yet
- Lab ProfileDocument2 pagesLab ProfileMarvin Jay Ignacio MamingNo ratings yet
- AsdfghjiklmnbvcxzDocument6 pagesAsdfghjiklmnbvcxzSampath KumarNo ratings yet
- Become A Scribd Member For Full Acces First 30 Days Are FreeDocument4 pagesBecome A Scribd Member For Full Acces First 30 Days Are FreeRaphael HarryNo ratings yet
- Seshadri 2 8 2021 ModelDocument1 pageSeshadri 2 8 2021 ModelnayaktudaNo ratings yet
- NCAT Report 15 - 02 Literature Review: The Impact of Pavement Roughness On Vehicle Operating CostsDocument22 pagesNCAT Report 15 - 02 Literature Review: The Impact of Pavement Roughness On Vehicle Operating CostsVishnu RNo ratings yet
- Outlook February 12 2018Document76 pagesOutlook February 12 2018SHAMPA SINHAROYNo ratings yet
- Rheumatoid ModelDocument1 pageRheumatoid ModelDrAmit VermaNo ratings yet
- Mianwali Job Application FormDocument1 pageMianwali Job Application FormHusnain KazmiNo ratings yet
- Modern Information Retrieval: ModelingDocument263 pagesModern Information Retrieval: ModelingahmadNo ratings yet
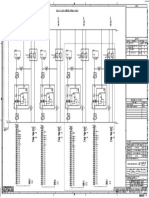
- 115Kv Busbar & BF Protection Panel-1 (D01/D02) : A P HA556 3-1313003.05 4400004657 EA-381637Document1 page115Kv Busbar & BF Protection Panel-1 (D01/D02) : A P HA556 3-1313003.05 4400004657 EA-381637Anonymous BZQOJwWIh6No ratings yet
- Scientists Under 40 Years of AgeDocument42 pagesScientists Under 40 Years of AgeKhurram IqbalNo ratings yet
- K SHD - 15423097962 1 PDFDocument34 pagesK SHD - 15423097962 1 PDFImtiaz AliNo ratings yet
- Political Science SemDocument16 pagesPolitical Science SemGrossAlasNo ratings yet
- Ecr 31032022Document1 pageEcr 31032022kvln murthyNo ratings yet
- Pre Reading Booklet For Chile PDFDocument49 pagesPre Reading Booklet For Chile PDFAndreaNo ratings yet
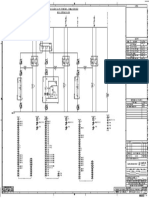
- 13.8Kv U/V Load Shedding Panel-2 +uvls.2: D HA555 P 3-1313003.03 EA-383186 4400004656Document1 page13.8Kv U/V Load Shedding Panel-2 +uvls.2: D HA555 P 3-1313003.03 EA-383186 4400004656Anonymous BZQOJwWIh6No ratings yet
- Characteristics of RightsDocument23 pagesCharacteristics of RightsArnav LekharaNo ratings yet
- Good IrmodelingDocument263 pagesGood IrmodelingBhavy SinghNo ratings yet
- ReportDocument1 pageReportSupun Kanchana ChandrarathnaNo ratings yet
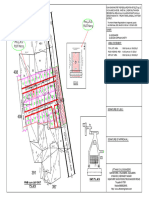
- Site Analysis CompressedDocument1 pageSite Analysis CompressedSupriya SamantaNo ratings yet
- Lab Requisition SampleDocument1 pageLab Requisition SampleUser SmuggNo ratings yet
- Moravian Cemetery MapDocument1 pageMoravian Cemetery MaphmiklitzNo ratings yet
- B - Braun: EffectiveDocument6 pagesB - Braun: EffectiveDaniela Patricia Gutiérrez MartínezNo ratings yet
- Anp & AhpDocument74 pagesAnp & AhpNihar Ranjan BarikNo ratings yet
- Mapa Solar Del Ecuador 2019: January 2020Document33 pagesMapa Solar Del Ecuador 2019: January 2020OSCAR VINICIO CHUQUITARCO LAGLANo ratings yet
- Duty Lab Cycle AnalysisDocument1 pageDuty Lab Cycle AnalysisGaurav ChauhanNo ratings yet
- May 5 Presentation: Comparing Public and Private Employee Compensaton and Retrement Benefits in CaliforniaDocument9 pagesMay 5 Presentation: Comparing Public and Private Employee Compensaton and Retrement Benefits in Californiasmf 4LAKidsNo ratings yet
- CAP 2022 Digital Order Renewal Form - CAP# 901958201, Expedient Healthcare Marketing PVT LTD DBA HealthiansDocument162 pagesCAP 2022 Digital Order Renewal Form - CAP# 901958201, Expedient Healthcare Marketing PVT LTD DBA HealthiansSharik MasoodNo ratings yet
- Akhwat Yar MirzaDocument1 pageAkhwat Yar MirzaAnonymous BZQOJwWIh6No ratings yet
- Farrokh K 2023 Military Reasons of HeracDocument38 pagesFarrokh K 2023 Military Reasons of HeracGligor BozinoskiNo ratings yet
- ScorereportDocument3 pagesScorereportapi-439003043No ratings yet
- Business Model Canvas Poster-DikonversiDocument1 pageBusiness Model Canvas Poster-DikonversiHana NatashamuraNo ratings yet
- Topographic Map of StarrvilleDocument1 pageTopographic Map of StarrvilleHistoricalMapsNo ratings yet
- Product Note - Ipo: Issue HighlightsDocument3 pagesProduct Note - Ipo: Issue Highlightsvidhyaeswaran2143No ratings yet
- Ac Generator Reference: Download NowDocument3 pagesAc Generator Reference: Download NowMANJUNATH manjunathNo ratings yet
- LB1 Format Revisi 2019 MaretDocument25 pagesLB1 Format Revisi 2019 MaretBintang Azzahra Al-adawiyahNo ratings yet
- Vawc Compliance Monitoring FormDocument1 pageVawc Compliance Monitoring FormOmar Dizon100% (4)
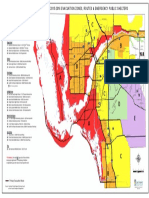
- Evac ZonesDocument1 pageEvac ZonesJessica McBrideNo ratings yet
- 2011 Publication of Guardian University Guide: Grid of Provisional Subject AppearancesDocument7 pages2011 Publication of Guardian University Guide: Grid of Provisional Subject AppearancesThe GuardianNo ratings yet
- Beneath New Culture Is Old Psychology Gossip and Social StratificationDocument6 pagesBeneath New Culture Is Old Psychology Gossip and Social StratificationCarlos PlazasNo ratings yet
- Nrad Full ReportDocument115 pagesNrad Full ReportSophia RoseNo ratings yet
- Accurate Determination of Catalyst Loading On Glassy Carbon Disk and Its Impact On Thin Film Rotating Disk Electrode For Oxygen Reduction Reaction.Document1 pageAccurate Determination of Catalyst Loading On Glassy Carbon Disk and Its Impact On Thin Film Rotating Disk Electrode For Oxygen Reduction Reaction.Muralidhar ChourashiyaNo ratings yet
- Neurologic Complications of Cancer Drug Therapies.11Document11 pagesNeurologic Complications of Cancer Drug Therapies.11Mayra AlejandraNo ratings yet
- Heat LoadDocument41 pagesHeat LoadpanyamnrNo ratings yet
- EconomicsDocument16 pagesEconomicsGrossAlasNo ratings yet
- Podar 2019 - 21 Kalyan Vagad Girgaon Andheri Borivali Dadar: #REF! #REF!Document1 pagePodar 2019 - 21 Kalyan Vagad Girgaon Andheri Borivali Dadar: #REF! #REF!bhavikNo ratings yet
- Orchestrating A Winning Strategy: End-To-End Supply Chain SynchronizationDocument52 pagesOrchestrating A Winning Strategy: End-To-End Supply Chain SynchronizationANGELICANo ratings yet
- Atlas Solar Del EcuadorDocument33 pagesAtlas Solar Del EcuadorChristianEstrellaNietoNo ratings yet
- Bell S Palsy 10Document20 pagesBell S Palsy 10Ananya DebNo ratings yet
- Research Title SheetDocument1 pageResearch Title SheetGlee Gray FrauletheaNo ratings yet
- Kresse Vasp PhononDocument54 pagesKresse Vasp PhononNamrata JaykhedkarNo ratings yet
- AYUSHI THAKKAR - SEC-C - FAR - Individual Assignment IDocument7 pagesAYUSHI THAKKAR - SEC-C - FAR - Individual Assignment IAyushi ThakkarNo ratings yet
- 303 Excavator Electrical System: Harness and Wire Electrical Schematic SymbolsDocument2 pages303 Excavator Electrical System: Harness and Wire Electrical Schematic Symbolsramon hidalgoNo ratings yet
- Literacy Rate PercentageDocument1 pageLiteracy Rate Percentageteja 1570No ratings yet
- Basic NRP Algorithm EnglishDocument1 pageBasic NRP Algorithm EnglishRumela Ganguly ChakrabortyNo ratings yet
- Curriculum Vitae: NAME: Rumela Chakraborty MOBILE NO: 8617254440 E-Mail IdDocument6 pagesCurriculum Vitae: NAME: Rumela Chakraborty MOBILE NO: 8617254440 E-Mail IdRumela Ganguly ChakrabortyNo ratings yet
- Extended Mop Up Notice 1Document1 pageExtended Mop Up Notice 1Rumela Ganguly ChakrabortyNo ratings yet
- You Are Here: Skip To Main ContentDocument5 pagesYou Are Here: Skip To Main ContentRumela Ganguly ChakrabortyNo ratings yet
- Health PDFDocument94 pagesHealth PDFMayom MabuongNo ratings yet
- 7 Essential Nursing Care of The Critically Ill PatientDocument24 pages7 Essential Nursing Care of The Critically Ill PatientAyah TiarAzkaNo ratings yet
- Cardiac Surgery in Octogenarians: Peri-Operative Outcome and Long-Term ResultsDocument9 pagesCardiac Surgery in Octogenarians: Peri-Operative Outcome and Long-Term ResultsRumela Ganguly ChakrabortyNo ratings yet
- 3 11 38 983Document5 pages3 11 38 983Rumela Ganguly ChakrabortyNo ratings yet
- 5 TarangDocument8 pages5 TarangRumela Ganguly ChakrabortyNo ratings yet
- Quality of Life After Open-Heart Surgery in Patients Over 75 Years OldDocument4 pagesQuality of Life After Open-Heart Surgery in Patients Over 75 Years OldRumela Ganguly ChakrabortyNo ratings yet
- WHO Report - April 23Document12 pagesWHO Report - April 23CityNewsTorontoNo ratings yet
- Article 6Document4 pagesArticle 6Rumela Ganguly ChakrabortyNo ratings yet
- 100 PijlsDocument118 pages100 PijlsSinisa RisticNo ratings yet
- Acute Myocardial Infarction Survivors Experiences: A Qualitative Literature ReviewDocument10 pagesAcute Myocardial Infarction Survivors Experiences: A Qualitative Literature ReviewRumela Ganguly ChakrabortyNo ratings yet
- Quality of Life After Cardiac Surgery: Underresearched ResearchDocument5 pagesQuality of Life After Cardiac Surgery: Underresearched ResearchRumela Ganguly ChakrabortyNo ratings yet
- Bitton2013 PDFDocument21 pagesBitton2013 PDFVirgo WNo ratings yet
- 2006 Inaccurate Risk PerceptionDocument5 pages2006 Inaccurate Risk PerceptionRumela Ganguly ChakrabortyNo ratings yet
- MSC NursingDocument8 pagesMSC NursingRumela Ganguly ChakrabortyNo ratings yet
- Annotated Bibliograhy: Submitted ToDocument4 pagesAnnotated Bibliograhy: Submitted ToRumela Ganguly ChakrabortyNo ratings yet
- Deciding Which Short Form Survey To UseDocument8 pagesDeciding Which Short Form Survey To UseRumela Ganguly ChakrabortyNo ratings yet
- Nurses NoteDocument1 pageNurses NoteRumela Ganguly ChakrabortyNo ratings yet
- 2008 CCModule 3Document13 pages2008 CCModule 3Jaymee GasparNo ratings yet
- 1427 - Rana Kachouh Nursing Process HammoudDocument54 pages1427 - Rana Kachouh Nursing Process HammoudRumela Ganguly ChakrabortyNo ratings yet
- Emerging Role of District Level Nursing PersonnelDocument9 pagesEmerging Role of District Level Nursing PersonnelRumela Ganguly ChakrabortyNo ratings yet
- Knowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionDocument49 pagesKnowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionRumela Ganguly ChakrabortyNo ratings yet
- 05 N501 28766Document23 pages05 N501 28766Rumela Ganguly ChakrabortyNo ratings yet
- Article 6Document4 pagesArticle 6Rumela Ganguly ChakrabortyNo ratings yet
- 11v.jigisha Chaptear2Document53 pages11v.jigisha Chaptear2Anirban PalNo ratings yet
- Flexural Design of Fiber-Reinforced Concrete Soranakom Mobasher 106-m52Document10 pagesFlexural Design of Fiber-Reinforced Concrete Soranakom Mobasher 106-m52Premalatha JeyaramNo ratings yet
- Brand Zara GAP Forever 21 Mango H&M: Brand Study of Zara Nancys Sharma FD Bdes Batch 2 Sem 8 Brand-ZaraDocument2 pagesBrand Zara GAP Forever 21 Mango H&M: Brand Study of Zara Nancys Sharma FD Bdes Batch 2 Sem 8 Brand-ZaraNancy SharmaNo ratings yet
- Ra 9048 Implementing RulesDocument9 pagesRa 9048 Implementing RulesToffeeNo ratings yet
- Brent Berlin-Covert Categories and Folk TaxonomyDocument10 pagesBrent Berlin-Covert Categories and Folk TaxonomyKawita ChuachengNo ratings yet
- The Concepts and Principles of Equity and HealthDocument18 pagesThe Concepts and Principles of Equity and HealthPaulo César López BarrientosNo ratings yet
- Unit 6 Listening Practice OUT AND ABOUT 1Document1 pageUnit 6 Listening Practice OUT AND ABOUT 1Marta Sampedro GonzalezNo ratings yet
- CaseDocument2 pagesCaseKimi Walia0% (2)
- Task 1 Methods in Teaching LiteratureDocument2 pagesTask 1 Methods in Teaching LiteratureJaepiNo ratings yet
- Analysis of Effectiveness of Heat Exchanger Shell and Tube Type One Shell Two Tube Pass As Cooling OilDocument6 pagesAnalysis of Effectiveness of Heat Exchanger Shell and Tube Type One Shell Two Tube Pass As Cooling OilHendrik V SihombingNo ratings yet
- Organisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)Document28 pagesOrganisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)mahtaabkNo ratings yet
- Mag Issue137 PDFDocument141 pagesMag Issue137 PDFShafiq Nezat100% (1)
- List of Naruto Char.Document40 pagesList of Naruto Char.Keziah MecarteNo ratings yet
- 280-Article Text-1201-1-10-20220426Document8 pages280-Article Text-1201-1-10-20220426Ayu Ratri PNo ratings yet
- Chryso CI 550Document2 pagesChryso CI 550Flavio Jose MuhaleNo ratings yet
- English VowelDocument6 pagesEnglish Vowelqais yasinNo ratings yet
- Communist Party of India - WikipediaDocument104 pagesCommunist Party of India - WikipediaRameshwar ChandravanshiNo ratings yet
- Vassula Ryden TestimoniesDocument7 pagesVassula Ryden TestimoniesFrancis LoboNo ratings yet
- Shipping Operation Diagram: 120' (EVERY 30')Document10 pagesShipping Operation Diagram: 120' (EVERY 30')Hafid AriNo ratings yet
- AL Applied Mathematics 1989 Paper1+2 (E)Document7 pagesAL Applied Mathematics 1989 Paper1+2 (E)eltytanNo ratings yet
- The Novel TodayDocument3 pagesThe Novel Todaylennon tanNo ratings yet
- Press ReleaseDocument1 pagePress Releaseapi-303080489No ratings yet
- Universal Prayers IIDocument3 pagesUniversal Prayers IIJericho AguiatanNo ratings yet
- 4 Problem GamblingDocument14 pages4 Problem GamblingLee Jia HuiNo ratings yet
- The Impact of Climatic and Cultural Factors On Openings in Traditional Houses in MaharashtraDocument14 pagesThe Impact of Climatic and Cultural Factors On Openings in Traditional Houses in Maharashtracoldflame81No ratings yet
- Case Study 3Document6 pagesCase Study 3monika_pratiwi_2No ratings yet