You might also like
- Reducing Airborne Exposure of COVID 19 Using Air Filtration Systems WhitePaperDocument9 pagesReducing Airborne Exposure of COVID 19 Using Air Filtration Systems WhitePaperColectibondiNo ratings yet
- E DAR Filter CatalogDocument38 pagesE DAR Filter CatalogJittiya WatcharotayangulNo ratings yet
- Airborne Covid-19-1Document2 pagesAirborne Covid-19-1riansyahNo ratings yet
- Microorganisms in Air SamplingDocument20 pagesMicroorganisms in Air SamplingerparixitpandeyNo ratings yet
- Respiratory Device Filters Catalogue INT Issue 2 WebDocument8 pagesRespiratory Device Filters Catalogue INT Issue 2 Webmanuales tecnicosNo ratings yet
- Review Article: Humidification During Mechanical Ventilation in The Adult PatientDocument13 pagesReview Article: Humidification During Mechanical Ventilation in The Adult Patientdan iacobNo ratings yet
- ASHRAE Modes of Transmission and Filtration GuidanceDocument15 pagesASHRAE Modes of Transmission and Filtration GuidanceNelson SouzaNo ratings yet
- Bland Aerosol TherapyDocument9 pagesBland Aerosol TherapyRyl WonNo ratings yet
- Importance of Health Air Humidity in HospitalsDocument24 pagesImportance of Health Air Humidity in HospitalsM.d Islem MezouarNo ratings yet
- Microbial Air PollutionDocument4 pagesMicrobial Air Pollutionyam pdNo ratings yet
- air-sanitation-2012Document6 pagesair-sanitation-2012aleenaNo ratings yet
- Nursing Care of At-Risk Mothers and ChildrenDocument6 pagesNursing Care of At-Risk Mothers and ChildrenMushy_ayaNo ratings yet
- Covid-19 Has Redefined Airborne TransmissionDocument2 pagesCovid-19 Has Redefined Airborne Transmissiondoris schopperNo ratings yet
- Pbox 9-5 Evidence Based Practice Guidelines For The Prevention of Ventilator Associated Pneumonia (Vap)Document2 pagesPbox 9-5 Evidence Based Practice Guidelines For The Prevention of Ventilator Associated Pneumonia (Vap)Theresia FlorensiayssNo ratings yet
- Inhalationtherapy 120807161343 Phpapp02Document38 pagesInhalationtherapy 120807161343 Phpapp02Anonymous X0Rm9zNo ratings yet
- Performing Tracheal Suction-1Document1 pagePerforming Tracheal Suction-1SITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- Lec 3 PTDocument12 pagesLec 3 PTBassam AlgalalyNo ratings yet
- HEPA Filter Inthe Covid 19 Era-Function and EficacyDocument3 pagesHEPA Filter Inthe Covid 19 Era-Function and EficacynoeNo ratings yet
- The Use of Bacterial/viral Filters During Artificial Airway and Invasive Mechanical VentilationDocument6 pagesThe Use of Bacterial/viral Filters During Artificial Airway and Invasive Mechanical VentilationMarcelo AlejandroNo ratings yet
- Pulmonary Drug Delivery Originated As A More Relevant Alternative For Delivering Drugs To The LungsDocument3 pagesPulmonary Drug Delivery Originated As A More Relevant Alternative For Delivering Drugs To The LungsRajesh AkkiNo ratings yet
- ICS Guidance For Nebulization During The COVID 19Document7 pagesICS Guidance For Nebulization During The COVID 19salman683 gNo ratings yet
- Balingbing Histo LungsDocument5 pagesBalingbing Histo LungsJonas Zacarias BalingbingNo ratings yet
- Air SanitationDocument8 pagesAir SanitationVignesh ReddyNo ratings yet
- pulsFOG Aerosoldisinfection in Public Health HygieneDocument16 pagespulsFOG Aerosoldisinfection in Public Health Hygienecoralmoise64No ratings yet
- Transmission Route RhinovirusDocument5 pagesTransmission Route RhinoviruspreproperusNo ratings yet
- Endoscope Reprocessing Risk and Current Risk PracticeDocument65 pagesEndoscope Reprocessing Risk and Current Risk PracticeHosam GomaaNo ratings yet
- Containment of Procedure-Associated Aerosols by An Extractor Tent: Effect On Nebulized Drug Particle DispersalDocument6 pagesContainment of Procedure-Associated Aerosols by An Extractor Tent: Effect On Nebulized Drug Particle DispersalRSH Galaxy rehab medikNo ratings yet
- Critical Care SuctioningDocument5 pagesCritical Care SuctioningChinta Nabila 조롱 수없는No ratings yet
- HepaDocument6 pagesHepaPatricia HeraNo ratings yet
- ACBT and Autogenic Drainage PDFDocument14 pagesACBT and Autogenic Drainage PDFSwati GuptaNo ratings yet
- 01 Aerosol Delivery Devices in The Treatment of AsthmaDocument27 pages01 Aerosol Delivery Devices in The Treatment of Asthmatsegaab yosephNo ratings yet
- International Journal of Research in Pharmaceutical SciencesDocument16 pagesInternational Journal of Research in Pharmaceutical SciencesSatyam SachanNo ratings yet
- Visualizing The Effectiveness of Face Masks in Obstructing Respiratory JetsDocument8 pagesVisualizing The Effectiveness of Face Masks in Obstructing Respiratory JetsJakob RodriguezNo ratings yet
- Aerosol and Humidity Therapy 2Document27 pagesAerosol and Humidity Therapy 2Fadz HadjiriNo ratings yet
- Surgical Airway Procedures and ComplicationsDocument4 pagesSurgical Airway Procedures and ComplicationsGus LionsNo ratings yet
- The HVAC Systems Role in Environmental Infection Control 1585330997Document7 pagesThe HVAC Systems Role in Environmental Infection Control 1585330997Abdülhamit KayyaliNo ratings yet
- Updated Isolation StretcherDocument2 pagesUpdated Isolation StretcherCORRTECH ENGINEERINGNo ratings yet
- Aero BiologyDocument8 pagesAero BiologyFlavio ChipanaNo ratings yet
- Endoscope Reprocessing - How To Perform An Adequate Air DryDocument3 pagesEndoscope Reprocessing - How To Perform An Adequate Air DryBelén Mora BalboaNo ratings yet
- DR Dina - SARS-CoV-2 TransmissionDocument11 pagesDR Dina - SARS-CoV-2 TransmissionDina FaizahNo ratings yet
- Mechanical and Electrical EquipmentsDocument45 pagesMechanical and Electrical EquipmentsJohanson GoNo ratings yet
- Air Sanitation SystemsDocument29 pagesAir Sanitation SystemsmanmithNo ratings yet
- Activating To Success - A Comprehensive Review of Irrigant Agitation Devices in endodontics-PARIPEXDocument3 pagesActivating To Success - A Comprehensive Review of Irrigant Agitation Devices in endodontics-PARIPEXSnigdho DasNo ratings yet
- ARTICLE David N Schurk The HVAC Systems Roll in Environmental Infection Control For Hospitals REV 4 4 20 PDFDocument7 pagesARTICLE David N Schurk The HVAC Systems Roll in Environmental Infection Control For Hospitals REV 4 4 20 PDFSundar RamasamyNo ratings yet
- Research in High FlowaDocument6 pagesResearch in High FlowaVNo ratings yet
- Oxygen Delivery SystemsDocument9 pagesOxygen Delivery Systemsanon_784834955No ratings yet
- SuctioningDocument15 pagesSuctioningAngie MandeoyaNo ratings yet
- Filtration and Disinfection Faq ASHRAEDocument5 pagesFiltration and Disinfection Faq ASHRAEFamilia Toledo AlvesNo ratings yet
- RESUMEN MODULO III IRA - CompressedDocument97 pagesRESUMEN MODULO III IRA - CompressedGUSTAVONo ratings yet
- Humidification and Nebulization TechniquesDocument16 pagesHumidification and Nebulization TechniquesjanviNo ratings yet
- oxygen_therapyDocument40 pagesoxygen_therapySerah Ann ShajiNo ratings yet
- Challenges in Simulating and Modeling The Airborne Virus Transmission: A State-Of-The-Art ReviewDocument23 pagesChallenges in Simulating and Modeling The Airborne Virus Transmission: A State-Of-The-Art ReviewSustechlabNo ratings yet
- Oral Suctioning With RationaleDocument3 pagesOral Suctioning With RationaleKaguraNo ratings yet
- Kostroglou 2020Document4 pagesKostroglou 2020josiejonesNo ratings yet
- Sterile Filtration of Gases by Membrane Filters: Timothy J. Leahy and Raymond GablerDocument8 pagesSterile Filtration of Gases by Membrane Filters: Timothy J. Leahy and Raymond GablerMaheshNo ratings yet
- Supplying Oxygen InhalationDocument4 pagesSupplying Oxygen Inhalationjanna mae patriarcaNo ratings yet
- Airborne Infection ControlDocument43 pagesAirborne Infection Controlbphc meppadyNo ratings yet
- Research: P. M. de Oliveira, L. C. C. Mesquita, S. Gkantonas, A. Giusti and E. MastorakosDocument23 pagesResearch: P. M. de Oliveira, L. C. C. Mesquita, S. Gkantonas, A. Giusti and E. MastorakosKaroline MarxNo ratings yet
- Equipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterDocument2 pagesEquipment: Administering Oxygen by Way of Endotracheal and Tracheostomy Tubes With A T-Piece (Briggs) AdapterIan TuNo ratings yet
- 4 5997052321324860969 PDFDocument384 pages4 5997052321324860969 PDFMedicine Agency100% (1)
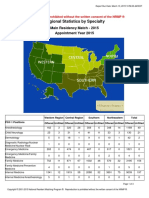
- NRMP Eras Match 3-16-15 Regional - Statistics - 2015Document3 pagesNRMP Eras Match 3-16-15 Regional - Statistics - 2015Niyi ArunaNo ratings yet
- Update 24,2 Basic Sciences 2008Document200 pagesUpdate 24,2 Basic Sciences 2008Ibrahim Fadl Mahmoud0% (1)
- Anae 12034Document8 pagesAnae 12034Gian Paolo SisonaNo ratings yet
- Anaesthesia: Update inDocument4 pagesAnaesthesia: Update inRaditya DidotNo ratings yet
- UnderstandingAnesthesia1 1 2Document144 pagesUnderstandingAnesthesia1 1 2marina_shawkyNo ratings yet
- Course Outline TP WindowsDocument6 pagesCourse Outline TP WindowsAnonymous PcPkRpAKD5No ratings yet
- dgx670 Es Om b0Document116 pagesdgx670 Es Om b0rafael enrique cely rodriguezNo ratings yet
- RJR Nabisco LBODocument14 pagesRJR Nabisco LBONazir Ahmad BahariNo ratings yet
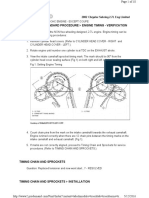
- 02+sebring+2.7+timing+chainDocument10 pages02+sebring+2.7+timing+chainMaushil Salman MarkNo ratings yet
- b1 Preliminary For Schools Classroom Posters and Activities PDFDocument13 pagesb1 Preliminary For Schools Classroom Posters and Activities PDFNat ShattNo ratings yet
- Lesson 2: Weaving A Mannahatta Muir WebDocument2 pagesLesson 2: Weaving A Mannahatta Muir WebTamas SzamosfalvyNo ratings yet
- Large Generators WEBDocument16 pagesLarge Generators WEBMaycon MaranNo ratings yet
- Jun 2005 - AnsDocument13 pagesJun 2005 - AnsHubbak Khan100% (1)
- DEME Offshore Brochure_2022Document16 pagesDEME Offshore Brochure_2022amin32No ratings yet
- CN Assignment 1 COE-540Document5 pagesCN Assignment 1 COE-540Ghazanfar LatifNo ratings yet
- Diagnosing and Managing Acute and Chronic SinusitisDocument14 pagesDiagnosing and Managing Acute and Chronic SinusitisAnonymous y3TIOwX8100% (1)
- Leadership's Ramdom MCQsDocument48 pagesLeadership's Ramdom MCQsAhmed NoumanNo ratings yet
- Sample Resume For HRDocument2 pagesSample Resume For HRnapinnvoNo ratings yet
- React Rich Text EditorDocument3 pagesReact Rich Text Editordhirendrapratapsingh398No ratings yet
- Remove Fuel Sub TankDocument9 pagesRemove Fuel Sub Tankthierry.fifieldoutlook.comNo ratings yet
- MF ISIN CodeDocument49 pagesMF ISIN CodeshriramNo ratings yet
- Sunday School Lesson Activity 219 Moses Builds A Tablernacle in The Wilderness - Printable 3D Model KitDocument17 pagesSunday School Lesson Activity 219 Moses Builds A Tablernacle in The Wilderness - Printable 3D Model Kitmcontrerasseitz3193No ratings yet
- Cracking The SQL InterviewDocument52 pagesCracking The SQL InterviewRedouan AFLISSNo ratings yet
- SRV210 - 250TC Spare PartsDocument2 pagesSRV210 - 250TC Spare PartsEnzo SovittiNo ratings yet
- RD218 Gardan 3110 Ob2226657 NDocument1 pageRD218 Gardan 3110 Ob2226657 Nopen hartigNo ratings yet
- v16 n3Document219 pagesv16 n3Mark ReinhardtNo ratings yet
- CEO Corner New Products Powerful Pocket SimulatorDocument23 pagesCEO Corner New Products Powerful Pocket SimulatorMOHAMMA MUSANo ratings yet
- Analisis Hasil Led Pada Jam Pertama Dan Jam KeduaDocument11 pagesAnalisis Hasil Led Pada Jam Pertama Dan Jam KeduavirafutmainnarNo ratings yet
- Perlis V. Composer's Voices From Ives To Ellington PDFDocument506 pagesPerlis V. Composer's Voices From Ives To Ellington PDFOleksii Ternovii100% (1)
- 2020会社案内(英語版)Document18 pages2020会社案内(英語版)DAC ORGANIZERNo ratings yet
- Arts and Crafts of Basey SamarDocument28 pagesArts and Crafts of Basey SamarTrisha MenesesNo ratings yet
- Eddy Current Testing Exam Questions Assignment2Document1 pageEddy Current Testing Exam Questions Assignment2Narotam Kumar GupteshwarNo ratings yet
- Delays in Endoscope Reprocessing and The Biofilms WithinDocument12 pagesDelays in Endoscope Reprocessing and The Biofilms WithinHAITHM MURSHEDNo ratings yet
- XFARDocument14 pagesXFARRIZA SAMPAGANo ratings yet
- Rate of ChangeDocument22 pagesRate of ChangeTrisha MariehNo ratings yet