You might also like
- White Book - 4 DelDocument12 pagesWhite Book - 4 DelJJovance80% (10)
- 4443-Multiple Choice Questions in Orthopaedics and TraumaDocument32 pages4443-Multiple Choice Questions in Orthopaedics and TraumaJunaidahMubarakAli81% (27)
- Toronto+Notes+2011+ +21.+orthopaedicsDocument46 pagesToronto+Notes+2011+ +21.+orthopaedicsChanique Cousins100% (1)
- Anatomy Concept Book AtfDocument246 pagesAnatomy Concept Book AtfRishi ShekharNo ratings yet
- 4443-Multiple Choice Questions in Orthopaedics and TraumaDocument32 pages4443-Multiple Choice Questions in Orthopaedics and TraumaAhmed ALi100% (1)
- Cast and BracesDocument58 pagesCast and BracesNikki M. Arapol100% (1)
- Orthopedics MCQs With AnswersDocument32 pagesOrthopedics MCQs With AnswerslanghalilafaNo ratings yet
- Polio - Ankle and FootDocument9 pagesPolio - Ankle and FootDoc DelowerNo ratings yet
- Cyriax ConceptDocument26 pagesCyriax ConceptMeenakshiputraeashwarprasad MacherlaNo ratings yet
- UKITE 07 AnswersDocument46 pagesUKITE 07 AnswersJipin Gopi100% (1)
- Chapter 25: Trauma: (Also See Chapter 19, Pediatrics)Document70 pagesChapter 25: Trauma: (Also See Chapter 19, Pediatrics)poddataNo ratings yet
- Gait CycleDocument74 pagesGait CycleOnwaree Ing100% (2)
- Booty by Bret Month 59Document16 pagesBooty by Bret Month 59moniquesmith90No ratings yet
- Triangular BandagingDocument25 pagesTriangular Bandagingcelinewinchester7No ratings yet
- Sleeve Fracture of The Adult PatellaDocument3 pagesSleeve Fracture of The Adult PatellaRadenMasKaerNo ratings yet
- Congenital Pseudoarthrosis of The Clavicle A Rare CaseDocument5 pagesCongenital Pseudoarthrosis of The Clavicle A Rare CaseInternational Medical PublisherNo ratings yet
- Thoracoscopic Excision of Symptomatic Esophageal Duplication Cyst in Adult Population-Experience From A Tertiary Care CenterDocument5 pagesThoracoscopic Excision of Symptomatic Esophageal Duplication Cyst in Adult Population-Experience From A Tertiary Care CenterIJAR JOURNALNo ratings yet
- International Journal of Surgery: A. Pal, J.M.F. Clarke, A.E.P. CameronDocument6 pagesInternational Journal of Surgery: A. Pal, J.M.F. Clarke, A.E.P. CameronSujasree NavaneethanNo ratings yet
- Soal TraumaDocument10 pagesSoal TraumaYoga PribadiNo ratings yet
- Fracture Des Plateaux Tibiaux Yao 2018Document41 pagesFracture Des Plateaux Tibiaux Yao 2018KhalilNo ratings yet
- Patellar Tendon Avulsion With Tibial Tuberosity SLDocument4 pagesPatellar Tendon Avulsion With Tibial Tuberosity SLKirana ArinNo ratings yet
- The Chertsey Classification of Tibial Plateau FracDocument2 pagesThe Chertsey Classification of Tibial Plateau FracWahyuu N PutraNo ratings yet
- Locking T-Plate Repair of Ilial Fractures in Cats and Small DogsDocument8 pagesLocking T-Plate Repair of Ilial Fractures in Cats and Small DogsNayra Cristina Herreira do ValleNo ratings yet
- MutiLoc Nail Versus Philos Plate inDocument9 pagesMutiLoc Nail Versus Philos Plate inResi de Trauma OrtopediaNo ratings yet
- Fractures of The Scapular Neck: Diagnosis, Classifications and TreatmentDocument11 pagesFractures of The Scapular Neck: Diagnosis, Classifications and Treatmentsoheil ostovanNo ratings yet
- Atton's Surgery 4th EdDocument126 pagesAtton's Surgery 4th EdАлександр АртамоновNo ratings yet
- Case Report Traumatic Fracture: Dislocation of Cervicothoracic Junction - Grand Round Presentation of C7-T1 Instabilities and Different Instrumentation TechniquesDocument6 pagesCase Report Traumatic Fracture: Dislocation of Cervicothoracic Junction - Grand Round Presentation of C7-T1 Instabilities and Different Instrumentation TechniquesMohammad Al-SofyaniNo ratings yet
- PCL Avulsion Fracture 2Document2 pagesPCL Avulsion Fracture 2harpreet singhNo ratings yet
- Spinal Cord Compression Due To Undiagnosed Thoracic Meningioma Following Lumbar Surgery in An Elderly Patient: A CaseDocument4 pagesSpinal Cord Compression Due To Undiagnosed Thoracic Meningioma Following Lumbar Surgery in An Elderly Patient: A CaseLuwiNo ratings yet
- 9 Suppl - 1 S58Document7 pages9 Suppl - 1 S58ChristopherLawrenceNo ratings yet
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Initial Angular Deformity and Its Recovery of The Proximal Tibial Metaphyseal Fracture According To The Cause: Trampoline-Related Injury Versus Other InjuriesDocument8 pagesInitial Angular Deformity and Its Recovery of The Proximal Tibial Metaphyseal Fracture According To The Cause: Trampoline-Related Injury Versus Other InjuriesYuji AibNo ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Complications of Pediatric Femur Fractures Treated With Titanium Elastic NailsDocument4 pagesComplications of Pediatric Femur Fractures Treated With Titanium Elastic Nailsrhamadani.farahNo ratings yet
- Solomon 2010Document10 pagesSolomon 2010Roger WatersNo ratings yet
- Le Fort Fractures With Maxillary ImmobilityDocument6 pagesLe Fort Fractures With Maxillary ImmobilityNguyễn Minh NgọcNo ratings yet
- Arthroscopic Fixation of Intercondylar Eminence Fractures Using A 4-Portal TechniqueDocument11 pagesArthroscopic Fixation of Intercondylar Eminence Fractures Using A 4-Portal Techniquesyairozi_hidayatNo ratings yet
- 4 in 1 Quadricepsplasty For Fixed and Habitual DisDocument8 pages4 in 1 Quadricepsplasty For Fixed and Habitual DisMinh ChíNo ratings yet
- Bab 1Document12 pagesBab 1ibnu syahNo ratings yet
- Adolescent-Type Ankle:: Tillaux Fracture of The Two Case ReportsDocument4 pagesAdolescent-Type Ankle:: Tillaux Fracture of The Two Case ReportsMohammed TayyemNo ratings yet
- Article in Press: Brachial Plexus Birth Palsy: Management During The First Year of LifeDocument8 pagesArticle in Press: Brachial Plexus Birth Palsy: Management During The First Year of LifeDyah SafitriNo ratings yet
- Comminuted Patella Fracture in Elderly Patients - A Systematic Review and Case ReportDocument10 pagesComminuted Patella Fracture in Elderly Patients - A Systematic Review and Case ReportAldrovando JrNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- Clinical Analysis of Classification For Tibial PlaDocument17 pagesClinical Analysis of Classification For Tibial PlaRizky Andrey RarungNo ratings yet
- Musculo Exam 2004Document7 pagesMusculo Exam 2004AngeredYetiNo ratings yet
- Treating Patella Fractures With A Fixed-Angle Patella PlateDocument7 pagesTreating Patella Fractures With A Fixed-Angle Patella PlateAldrovando JrNo ratings yet
- Quinto SADocument5 pagesQuinto SAFreddy Churata SuriNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Plantillo Anteromedial + LCP + ApeDocument7 pagesPlantillo Anteromedial + LCP + ApeThiagoNo ratings yet
- Tibial Derotational Osteotomies in Two Neuromuscular PopulationsDocument6 pagesTibial Derotational Osteotomies in Two Neuromuscular PopulationsJuan Agustin Valcarce LeonNo ratings yet
- Anatomy and Classification of The Posterior Tibial Fragment in Ankle FracturesDocument13 pagesAnatomy and Classification of The Posterior Tibial Fragment in Ankle FracturesCruz RamonNo ratings yet
- Treatment of Aring of The Costal Arch After The Minimally Invasive Pectus Excavatum Repair (Nuss Procedure) in ChildrenDocument4 pagesTreatment of Aring of The Costal Arch After The Minimally Invasive Pectus Excavatum Repair (Nuss Procedure) in ChildrenFelix RushNo ratings yet
- Percutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDocument7 pagesPercutaneous Femoral Derotational Osteotomy For Excessive Femoral TorsionDouglas PrinaNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- The Management of Bilateral Posterior Fracture Dislocations of The Shoulder: A Case Series Illustrating Management OptionsDocument7 pagesThe Management of Bilateral Posterior Fracture Dislocations of The Shoulder: A Case Series Illustrating Management OptionsGustavo BECERRA PERDOMONo ratings yet
- 5.776 2014 Article 653Document11 pages5.776 2014 Article 653AndaPintilieNo ratings yet
- Boxer Fracture: An Unusual Presentation: KeywordsDocument3 pagesBoxer Fracture: An Unusual Presentation: KeywordsRadita Dwihaning PutriNo ratings yet
- Codo FlotanteDocument16 pagesCodo FlotanteOlinda Maria GamarraNo ratings yet
- Protrusio Acetabuli Diagnosis and TreatmentDocument10 pagesProtrusio Acetabuli Diagnosis and TreatmentFerney Leon BalceroNo ratings yet
- Postamputation Orthopedic Surgery in Canine Amputees: Owner Satisfaction and OutcomeDocument8 pagesPostamputation Orthopedic Surgery in Canine Amputees: Owner Satisfaction and OutcomeBrenda Yohana Benitez CristianoNo ratings yet
- Late Fracture of The Hip After Reamed Intramedullary Nailing of The FemurDocument5 pagesLate Fracture of The Hip After Reamed Intramedullary Nailing of The FemurGordana PuzovicNo ratings yet
- Transposition of EIP Pro EPL ACTA BIOMED 2019 Sperati - CeriDocument4 pagesTransposition of EIP Pro EPL ACTA BIOMED 2019 Sperati - CerivasasdfwqeNo ratings yet
- Elif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesDocument7 pagesElif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesHariom ShuklaNo ratings yet
- Zygomatic Fractures: Classification and Complications: TveterasDocument7 pagesZygomatic Fractures: Classification and Complications: TveterasBriando Stevano LinelejanNo ratings yet
- Essential Orthopedic Review: Questions and Answers for Senior Medical StudentsFrom EverandEssential Orthopedic Review: Questions and Answers for Senior Medical StudentsAdam E.M. EltoraiNo ratings yet
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- Cubital Tunnel Syndrome: Diagnosis, Management and RehabilitationFrom EverandCubital Tunnel Syndrome: Diagnosis, Management and RehabilitationJohn R. FowlerNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Treatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiDocument4 pagesTreatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiNuno Craveiro LopesNo ratings yet
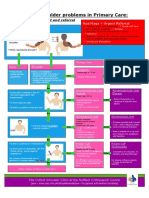
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- FTU CountDocument1 pageFTU CountOliver QNo ratings yet
- Pelvic TraumaDocument47 pagesPelvic TraumaMuhammad DaniyalNo ratings yet
- ACL Peroneus GraftDocument16 pagesACL Peroneus Graftanon_550027423No ratings yet
- Chapter 8 PDFDocument39 pagesChapter 8 PDFDr Tahira NihalNo ratings yet
- Body Adjustment To Elevate The Spirit KriyaDocument5 pagesBody Adjustment To Elevate The Spirit KriyaHans Werner DaakeNo ratings yet
- Bilateral Variation in The Branching Pattern of The Axillary Artery - A Case ReportDocument5 pagesBilateral Variation in The Branching Pattern of The Axillary Artery - A Case ReportIJAR JOURNALNo ratings yet
- Fluoric Acid - Allen HandbookDocument12 pagesFluoric Acid - Allen HandbookaldodiasNo ratings yet
- QAWELLNESS MASSAGE Q3 Module 3Document28 pagesQAWELLNESS MASSAGE Q3 Module 3meachie100% (1)
- El Nuevo Orden Del Astrosol PDFDocument12 pagesEl Nuevo Orden Del Astrosol PDFJulián AndrésNo ratings yet
- Anatomy Mnemonics: Diaphragm Apertures: Spinal LevelsDocument22 pagesAnatomy Mnemonics: Diaphragm Apertures: Spinal Levelsagar agarNo ratings yet
- Final Back&NeckPainManagement StudyMaterialDocument9 pagesFinal Back&NeckPainManagement StudyMaterialchinnu1235395No ratings yet
- Orca Share Media1571800842460Document27 pagesOrca Share Media1571800842460Reniel De MesaNo ratings yet
- An Electromyographic Analysis of Sumo And.19Document7 pagesAn Electromyographic Analysis of Sumo And.19JulianoEscudeiroNo ratings yet
- Dumbbell Workout Routine FinalDocument18 pagesDumbbell Workout Routine FinalSachith SeneviratnaNo ratings yet
- JRF - Allograft Catalog 2019 - M600.002Document20 pagesJRF - Allograft Catalog 2019 - M600.002Gopi RamuNo ratings yet
- Origen HipotoniaDocument7 pagesOrigen HipotoniaPablo Hernández MaripillánNo ratings yet
- HSB Skeletal NotesDocument2 pagesHSB Skeletal NotesArvin SinghNo ratings yet
- Excercise 2 Activity 7 DoniDocument6 pagesExcercise 2 Activity 7 DoniDoni SaragihNo ratings yet
- Gluteal Region, Back of The Thigh and Popliteal Fossa: Kimaiga H.O 1 Year MBCHB (Uon)Document342 pagesGluteal Region, Back of The Thigh and Popliteal Fossa: Kimaiga H.O 1 Year MBCHB (Uon)Patrick NyakwambaNo ratings yet