You might also like
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Hyl 142Document11 pagesHyl 142Stefania CristinaNo ratings yet
- Dr. Nazim Mughal: Ms Ortho, DNB Ortho FNB Spine SurgeryDocument90 pagesDr. Nazim Mughal: Ms Ortho, DNB Ortho FNB Spine Surgerynazim mughalNo ratings yet
- BoneDocument68 pagesBonedr_asaleh100% (2)
- Bone TumorsDocument43 pagesBone TumorsIsaac MwangiNo ratings yet
- Bone and Soft Tissue TumoursDocument9 pagesBone and Soft Tissue TumoursSurgicalgownNo ratings yet
- Sarcoma de Ewing S NEJMDocument11 pagesSarcoma de Ewing S NEJMbanzethyskyNo ratings yet
- Cervical MyelopathyDocument7 pagesCervical Myelopathybmahmood1No ratings yet
- Bone Tumors2006Document89 pagesBone Tumors2006api-19916399No ratings yet
- Neoplasm of Musculo SkeletalDocument70 pagesNeoplasm of Musculo SkeletalRiyan ArdiansyahNo ratings yet
- Bone Tumor Osteochondroma GuideDocument16 pagesBone Tumor Osteochondroma GuideJohn KingoriNo ratings yet
- Diagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesDocument69 pagesDiagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesMochammad Fariz AmsalNo ratings yet
- Osteosarcoma Mini-SymposiumDocument11 pagesOsteosarcoma Mini-SymposiumJawad KhanNo ratings yet
- Mascard2015 ABCs Vs UBCsDocument9 pagesMascard2015 ABCs Vs UBCsWemdi Priya PrasetyaNo ratings yet
- 12 Bone and Soft Tissue Sarcomas 200609 v2Document58 pages12 Bone and Soft Tissue Sarcomas 200609 v2dr. Ahmad MuhsininNo ratings yet
- Bone Tumors: Prepared by DR Pgr.2 Ortho Unit 3 BMCHDocument47 pagesBone Tumors: Prepared by DR Pgr.2 Ortho Unit 3 BMCHMohamed Al-zichrawyNo ratings yet
- Ewing's SarcomaDocument10 pagesEwing's SarcomaVerli Fajriati NofliNo ratings yet
- Seminar W4 - Bone & Soft Tissue TumoursDocument123 pagesSeminar W4 - Bone & Soft Tissue TumoursUN EPNo ratings yet
- Osteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmuDocument36 pagesOsteochondroma: Dr. Mahesh Chaudhary Phase-A Resident Radiology & Imaging BsmmubucculuNo ratings yet
- Pediatric Sarcomas of Bone - Clinical GateDocument8 pagesPediatric Sarcomas of Bone - Clinical GateAkira MasumiNo ratings yet
- Dr. Ronald V. Munthe Spot SMF Bedah Rs UkiDocument50 pagesDr. Ronald V. Munthe Spot SMF Bedah Rs UkiOdilia Maria RahalusNo ratings yet
- MUSKULOSKELETALDocument79 pagesMUSKULOSKELETALkhalishaNo ratings yet
- Bone and Soft Tissue SarcomasDocument57 pagesBone and Soft Tissue SarcomasTerseah MuNo ratings yet
- Group 10 NCM 112 - (Osteonecrosis)Document8 pagesGroup 10 NCM 112 - (Osteonecrosis)Jezreel BonaNo ratings yet
- Osteosarcoma: Pathology, Staging and Management: Eview RticleDocument10 pagesOsteosarcoma: Pathology, Staging and Management: Eview RticleAditya Rahman RYNo ratings yet
- Primary Osseous Tumors of The Pediatric Spinal ColumnDocument14 pagesPrimary Osseous Tumors of The Pediatric Spinal ColumnthanhdhyscribdNo ratings yet
- Ccaass Cclliinniiq Quuee //ccaassee Rreeppo OrrttDocument4 pagesCcaass Cclliinniiq Quuee //ccaassee Rreeppo OrrttCamil ChouairyNo ratings yet
- Ewing SarcomaDocument15 pagesEwing Sarcomaamel015No ratings yet
- Osteochondroses: Franklin Danger, MD Christopher Wasyliw, MD Laura Varich, MDDocument7 pagesOsteochondroses: Franklin Danger, MD Christopher Wasyliw, MD Laura Varich, MDadrianNo ratings yet
- Musculoskeletal Neoplasms GuideDocument21 pagesMusculoskeletal Neoplasms Guidei dewa wisnu putraNo ratings yet
- Case Report - Non Ossifying Fibroma of TibiaDocument3 pagesCase Report - Non Ossifying Fibroma of TibiaChristabella Natalia WijayaNo ratings yet
- Spinal Imaging DX Direct Compress (209 282)Document74 pagesSpinal Imaging DX Direct Compress (209 282)francktopr55No ratings yet
- fINAL of Octeochondroma in C - SpineDocument1 pagefINAL of Octeochondroma in C - SpineadilNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Bone Tumours - I & Ii - 2015Document113 pagesBone Tumours - I & Ii - 2015Nur Atiqah Mohd AzliNo ratings yet
- Osteosarcoma Bone Cancer in TeensDocument3 pagesOsteosarcoma Bone Cancer in TeensKristine CastilloNo ratings yet
- Solitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - InterdisciDocument5 pagesSolitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - Interdiscib00403007No ratings yet
- Fibrous DysplasiaDocument29 pagesFibrous Dysplasiadr_adjie100% (2)
- Radiological characteristics of periosteal reactionsDocument9 pagesRadiological characteristics of periosteal reactionsVesna PavlovicNo ratings yet
- Pediatric Malignant Bone TumoursDocument28 pagesPediatric Malignant Bone TumourscorneliusNo ratings yet
- 08 Bone TumorsDocument94 pages08 Bone TumorsSara FoudaNo ratings yet
- Benign Non Odontogenic Lesions - 6Document97 pagesBenign Non Odontogenic Lesions - 6Thaer ZabenNo ratings yet
- Imaging of Musculoskeletal SystemDocument53 pagesImaging of Musculoskeletal SystemSara ManzoorNo ratings yet
- ID NoneDocument9 pagesID NoneNur AnisaNo ratings yet
- Bone Tumor Types, Symptoms & TreatmentDocument2 pagesBone Tumor Types, Symptoms & TreatmentJinsen Paul MartinNo ratings yet
- Radiology NotesDocument24 pagesRadiology NotesAaron Raestas0% (1)
- Aneurysmal Bone Cyst: Review ArticleDocument9 pagesAneurysmal Bone Cyst: Review ArticleJeyachandran MariappanNo ratings yet
- One Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaDocument40 pagesOne Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaNaysahNo ratings yet
- Chondroma: X-Ray ShowsDocument2 pagesChondroma: X-Ray ShowsMd Ahsanuzzaman PinkuNo ratings yet
- Low-Grade Central Osteosarcoma Versus Fibrous Dysplasia: Carrie Y. Inwards, MDDocument6 pagesLow-Grade Central Osteosarcoma Versus Fibrous Dysplasia: Carrie Y. Inwards, MDManuelGonzalezGaitanoNo ratings yet
- Benign Bone Tumours Lecture - PpsDocument11 pagesBenign Bone Tumours Lecture - Ppsnickmirad2No ratings yet
- Benign Bone TumoursDocument13 pagesBenign Bone TumoursAnisah MahmudahNo ratings yet
- Foot and Ankle Tumor Radiographic FeaturesDocument9 pagesFoot and Ankle Tumor Radiographic FeaturesShazeb RizviNo ratings yet
- Fibrous Dysplasia - Radiology Reference Article - RadiopaediaDocument18 pagesFibrous Dysplasia - Radiology Reference Article - RadiopaediaManuelGonzalezGaitanoNo ratings yet
- Diagnostic Imaging - 6 - Osteolytic Lesions, Sclerosis, Neoplasia, Atrophy, Infection - Prof - Dr.İsmet TAMERDocument26 pagesDiagnostic Imaging - 6 - Osteolytic Lesions, Sclerosis, Neoplasia, Atrophy, Infection - Prof - Dr.İsmet TAMERAly MssreNo ratings yet
- Chapter 13Document27 pagesChapter 13Zaky DavidiaNo ratings yet
- PathologyDocument12 pagesPathologyKetmia ZamoraNo ratings yet
- DsdfdfsDocument33 pagesDsdfdfsmayliaNo ratings yet
- Ew WikiDocument8 pagesEw WikidesyonkNo ratings yet
- Hip ExaminationDocument7 pagesHip ExaminationWaqas Haleem100% (1)
- Shoulder ReductionDocument4 pagesShoulder ReductionWaqas HaleemNo ratings yet
- Invx and Radiological Features of Promary Bone TumorsDocument14 pagesInvx and Radiological Features of Promary Bone TumorsWaqas HaleemNo ratings yet
- Rehman Medical Institute: MethodDocument1 pageRehman Medical Institute: MethodWaqas HaleemNo ratings yet
- Salma BibiDocument1 pageSalma BibiWaqas HaleemNo ratings yet
- Outcomes of Arthroscopic ACLDocument5 pagesOutcomes of Arthroscopic ACLWaqas HaleemNo ratings yet
- INx of Musculoskeletal MalignancyDocument9 pagesINx of Musculoskeletal MalignancyWaqas HaleemNo ratings yet
- Epidem of Bone and Soft Tissue TumorsDocument8 pagesEpidem of Bone and Soft Tissue TumorsWaqas HaleemNo ratings yet
- Candidate Guide To MRCS Examination July2018 PDFDocument51 pagesCandidate Guide To MRCS Examination July2018 PDFBakri MustafaNo ratings yet
- Vdocuments - MX - Mrcs Preparation Emrcs Questions Surgery PDFDocument1,085 pagesVdocuments - MX - Mrcs Preparation Emrcs Questions Surgery PDFWaqas HaleemNo ratings yet
- Plaster of Paris Backslab' Casts Application in The Emergency Department GuidelineDocument10 pagesPlaster of Paris Backslab' Casts Application in The Emergency Department GuidelineWaqas HaleemNo ratings yet
- Review of Orthopaedic Trauma 2e 2013 PDF Unitedvrg PDFDocument568 pagesReview of Orthopaedic Trauma 2e 2013 PDF Unitedvrg PDFWahyu Alamsyah DasopangNo ratings yet
- Chon Dro SarcomaDocument10 pagesChon Dro SarcomaWaqas HaleemNo ratings yet
- MX of Soft Tissue SarcomasDocument8 pagesMX of Soft Tissue SarcomasWaqas HaleemNo ratings yet
- KMU MBBS Result 2014-15Document5 pagesKMU MBBS Result 2014-15Waqas HaleemNo ratings yet
- Nasa Khan MRCS A Notes 2018 PDFDocument834 pagesNasa Khan MRCS A Notes 2018 PDFWaqas Haleem100% (5)
- KMU MBBS Result 2014-15Document5 pagesKMU MBBS Result 2014-15Waqas HaleemNo ratings yet
- Office Order Fcps2 July2019Document8 pagesOffice Order Fcps2 July2019Waqas HaleemNo ratings yet
- Subspecialty Induction July2019Document3 pagesSubspecialty Induction July2019Waqas HaleemNo ratings yet
- Instrumen Snars NestwsiDocument4 pagesInstrumen Snars NestwsiSyahrul Mubarak Danar SumantriNo ratings yet
- Fixed Provisional Merit List July 2019Document18 pagesFixed Provisional Merit List July 2019Waqas HaleemNo ratings yet
- Paton1981 Article HaemostaticChangesInDiabeticCoDocument6 pagesPaton1981 Article HaemostaticChangesInDiabeticCoWaqas HaleemNo ratings yet
- Surgical Patient Review PDFDocument2 pagesSurgical Patient Review PDFWaqas HaleemNo ratings yet
- Result of Mbbs Fa - 16Document23 pagesResult of Mbbs Fa - 16Waqas HaleemNo ratings yet
- How To Be An Excellent m3 Surgery Medical StudentDocument24 pagesHow To Be An Excellent m3 Surgery Medical StudentWaqas HaleemNo ratings yet
- ZZZZXDocument1 pageZZZZXJoko SantosoNo ratings yet
- Common Surgical Abbreviations: Continuous Bladder Irrigation (Urological Procedure)Document2 pagesCommon Surgical Abbreviations: Continuous Bladder Irrigation (Urological Procedure)llianNo ratings yet
- Mistakes in Fa 2017Document8 pagesMistakes in Fa 2017Nixon GoyalNo ratings yet
- How To Be An Excellent m3 Surgery Medical StudentDocument24 pagesHow To Be An Excellent m3 Surgery Medical StudentWaqas HaleemNo ratings yet
- In vitro effect of anti-coccidial drugs on Kudoa septempunctata myxosporesDocument5 pagesIn vitro effect of anti-coccidial drugs on Kudoa septempunctata myxosporesDeLiza SuhaaNo ratings yet
- Biology of Orthodontic Tooth MovementDocument16 pagesBiology of Orthodontic Tooth MovementGowri ShankarNo ratings yet
- Infowar and Spiritual Apocalypse The Destiny of Mankind: DR Bill Deagle MDDocument37 pagesInfowar and Spiritual Apocalypse The Destiny of Mankind: DR Bill Deagle MDprateekthaparian100% (1)
- Gizzard Proventriculus Health Marker Avinews Int Sept 22Document11 pagesGizzard Proventriculus Health Marker Avinews Int Sept 22mohamed helmyNo ratings yet
- Pharmaceutical Care Plan - Sample Version: (Dispensing and Medication Safety)Document4 pagesPharmaceutical Care Plan - Sample Version: (Dispensing and Medication Safety)Angela Pabico RosarioNo ratings yet
- Gce 221 NoteDocument18 pagesGce 221 NoteAyiri TieNo ratings yet
- Quiz 1A Hema LecDocument17 pagesQuiz 1A Hema LecAngela ReyesNo ratings yet
- A) State and Describe Various Stages of A Biodegradation StudyDocument6 pagesA) State and Describe Various Stages of A Biodegradation StudyAbdulkadir AlbabaNo ratings yet
- Karen Horney's Theory of Alienation and NeurosisDocument12 pagesKaren Horney's Theory of Alienation and NeurosisfridayantiNo ratings yet
- Blood (Notes)Document12 pagesBlood (Notes)Angel Rose BrillanteNo ratings yet
- Cyanide Clean-Up at Chumbwe Gold Mine in ZambiaDocument19 pagesCyanide Clean-Up at Chumbwe Gold Mine in ZambiaRamoutar (Ken) SeecharranNo ratings yet
- High Voltage Galvanic Current Lecture PDFDocument22 pagesHigh Voltage Galvanic Current Lecture PDFdespNo ratings yet
- Osmosis in Plant & Animal CellsDocument2 pagesOsmosis in Plant & Animal CellsBrooke MorganNo ratings yet
- The Antibacterial and Antifungal Activity of Essential Oil Derived From The Flesh of Nutmeg Fruit 6155Document6 pagesThe Antibacterial and Antifungal Activity of Essential Oil Derived From The Flesh of Nutmeg Fruit 6155Zyuha AiniiNo ratings yet
- The Land Bridge WorksheetDocument2 pagesThe Land Bridge Worksheetapi-306692383No ratings yet
- Los 12 Pilares de La Inteligencia, Adrian Owen PDFDocument6 pagesLos 12 Pilares de La Inteligencia, Adrian Owen PDFYasmina Itzel Murillo LopezNo ratings yet
- 09 10716 Perkembangan Larva Oryzias Javanicus Sebagai Kandidat Biota Formatedfinal2Document9 pages09 10716 Perkembangan Larva Oryzias Javanicus Sebagai Kandidat Biota Formatedfinal2Al- RezimNo ratings yet
- Actin and Actin-Binding Proteins: Thomas D. PollardDocument19 pagesActin and Actin-Binding Proteins: Thomas D. PollardArkha OnNo ratings yet
- Algorithms For The Design of A Multi-Stage Adaptive Kanban SystemDocument33 pagesAlgorithms For The Design of A Multi-Stage Adaptive Kanban SystemKharisma ElanNo ratings yet
- Activity 8 MycologyDocument3 pagesActivity 8 MycologyBrent Lee100% (1)
- Lab1 HistotechniqueDocument26 pagesLab1 HistotechniqueGitta Lakshita AnggariniNo ratings yet
- Notice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsDocument2 pagesNotice: Environmental Statements Notice of Intent: U. S. Navy Surveillance Towed Array Sensor System Low Frequency Active Sonar OperationsJustia.comNo ratings yet
- 2019 Book TheCapsicumGenome PDFDocument244 pages2019 Book TheCapsicumGenome PDFrosa_g11233No ratings yet
- ALL QB's PDFDocument36 pagesALL QB's PDFanimesh0gargNo ratings yet
- Soft Computing Unit-2Document61 pagesSoft Computing Unit-2namak sung loNo ratings yet
- Species RichnessDocument4 pagesSpecies RichnessFarhad HossainNo ratings yet
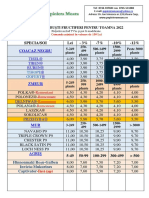
- 2oferta Arbusti Toamna2022Document3 pages2oferta Arbusti Toamna2022MariusTudoreanNo ratings yet
- WHO 4th Intl Standard For HCVDocument2 pagesWHO 4th Intl Standard For HCVSagir AlvaNo ratings yet
- Chemical Analysis of MANOIR XM AlloyDocument3 pagesChemical Analysis of MANOIR XM Alloyogun tokucNo ratings yet
- Blakemore Frith 2005 The Leaning BrainDocument221 pagesBlakemore Frith 2005 The Leaning BrainVictor MN100% (2)