You might also like
- Neonatal Resuscitation in FMC NigeriaDocument55 pagesNeonatal Resuscitation in FMC NigeriaIghodaro IsokenNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Resuscitarea-Lectie 1 Rezidenti 2024Document33 pagesResuscitarea-Lectie 1 Rezidenti 2024ioanadianaonofreiNo ratings yet
- Basic Life Support (BLS) Provider HandbookFrom EverandBasic Life Support (BLS) Provider HandbookRating: 5 out of 5 stars5/5 (2)
- Neonatal CareDocument59 pagesNeonatal CareKeith LajotNo ratings yet
- Neonatal Resuscitation JincyDocument78 pagesNeonatal Resuscitation JincyVivek PrabhakarNo ratings yet
- Neonatal EmergencyDocument40 pagesNeonatal EmergencyTamia PutriNo ratings yet
- NRP Overview and Principles of ResuscitationDocument27 pagesNRP Overview and Principles of ResuscitationMia FernandezNo ratings yet
- NRPDocument15 pagesNRPmohamed mowafeyNo ratings yet
- 39 Neonatal ResuscitationDocument38 pages39 Neonatal ResuscitationbenNo ratings yet
- Neonatal ResuscitationDocument46 pagesNeonatal ResuscitationAsaliwe BorahNo ratings yet
- Neonatal Resuscitation: Vineetha.T 1 Year MSC NursingDocument106 pagesNeonatal Resuscitation: Vineetha.T 1 Year MSC NursingVineetha ThachedathNo ratings yet
- Neonatal ResuscitationDocument83 pagesNeonatal ResuscitationАлександра КондряNo ratings yet
- Then Ewborn: By: Zosi Farah W. Fernandez, RNDocument64 pagesThen Ewborn: By: Zosi Farah W. Fernandez, RNindirinoor5No ratings yet
- Neonatal ResuscitationDocument34 pagesNeonatal ResuscitationAthul IgnatiusNo ratings yet
- II. AsfiksiaDocument41 pagesII. AsfiksiahazelelNo ratings yet
- Neonatal Resuscitation Techniques and EquipmentDocument54 pagesNeonatal Resuscitation Techniques and EquipmentdrkiranmNo ratings yet
- Transient &tachypnea of The Newborn: Prepared By: Laith Abd Alhameed Jabar Supervised By: Dr. Oğr Üyesi Erdal ÜnlüDocument16 pagesTransient &tachypnea of The Newborn: Prepared By: Laith Abd Alhameed Jabar Supervised By: Dr. Oğr Üyesi Erdal ÜnlüAli FalihNo ratings yet
- Neonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathDocument23 pagesNeonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathPraveen RamasamyNo ratings yet
- Neonatal ResuscitationDocument138 pagesNeonatal ResuscitationAbcdeNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- Neonatal ResuscitationDocument36 pagesNeonatal ResuscitationDemelash SolomonNo ratings yet
- Helping Baby To BreathDocument49 pagesHelping Baby To BreathmohdmaghyrehNo ratings yet
- Neonatal ResuscitationDocument51 pagesNeonatal ResuscitationAbdulkadir HasanNo ratings yet
- Lesson 1: Overview and Principles of Resuscitation: Neonatal Resuscitation Program Slide Presentation KitDocument32 pagesLesson 1: Overview and Principles of Resuscitation: Neonatal Resuscitation Program Slide Presentation KitChauthiran AgamudaiyarNo ratings yet
- Neonatal ResuscitationDocument35 pagesNeonatal ResuscitationR. Abhishek MishraNo ratings yet
- Cme NRPDocument73 pagesCme NRPpayapaya.pipacyclineNo ratings yet
- New Born ResuscitationDocument34 pagesNew Born ResuscitationPAUL NDEKINo ratings yet
- NeonatalresuscitationDocument67 pagesNeonatalresuscitationfidaNo ratings yet
- Nursing Care of High-Risk NewbornsDocument83 pagesNursing Care of High-Risk NewbornsChari RivoNo ratings yet
- Neonatal ResuscitationDocument15 pagesNeonatal ResuscitationAmruta GadeNo ratings yet
- Apnea in NewbornDocument58 pagesApnea in NewbornCharan RajNo ratings yet
- Neonatal Resuscitation Principles for Cardio-Maternal EmergenciesDocument65 pagesNeonatal Resuscitation Principles for Cardio-Maternal Emergencieserna moetNo ratings yet
- Dr. Taufiq - Breathing - TaufiqabdullahDocument51 pagesDr. Taufiq - Breathing - TaufiqabdullahAziz AzizahNo ratings yet
- Newborn Resuscitation Programme NRPDocument52 pagesNewborn Resuscitation Programme NRPHala BahaaNo ratings yet
- Nursing Care of A Family C NewbornDocument18 pagesNursing Care of A Family C NewbornAudreySalvadorNo ratings yet
- Respiratory - Distress (1) 2 PDFDocument8 pagesRespiratory - Distress (1) 2 PDFSatya Prakash TiwariNo ratings yet
- Emergency Nursing: BLS: Prepared By: Ms. Cherry Ann G. Garcia, RNDocument73 pagesEmergency Nursing: BLS: Prepared By: Ms. Cherry Ann G. Garcia, RNcherryann_12No ratings yet
- Special Considerations for Resuscitation of Premature BabiesDocument30 pagesSpecial Considerations for Resuscitation of Premature BabieswahyuwirawanNo ratings yet
- Newborn Resuscitation Program (NRP) TechniquesDocument47 pagesNewborn Resuscitation Program (NRP) TechniquesNethera Kiza ImperialNo ratings yet
- Pediatric Advanced Life Support: Jan Bazner-Chandler CPNP, CNS, MSN, RNDocument65 pagesPediatric Advanced Life Support: Jan Bazner-Chandler CPNP, CNS, MSN, RNد. محمد فريد الغنامNo ratings yet
- High Risk Newborn (8 Priorities)Document48 pagesHigh Risk Newborn (8 Priorities)Raquel MonsalveNo ratings yet
- Respiratory Emergencies GuideDocument71 pagesRespiratory Emergencies GuideChristian JaraNo ratings yet
- Neonatal Resuscitation: DR Hassan Abdullahi ElechiDocument17 pagesNeonatal Resuscitation: DR Hassan Abdullahi ElechiHadiza Adamu AuduNo ratings yet
- Resusitasi Neonatus PedomanDocument89 pagesResusitasi Neonatus PedomanDarma KomboNo ratings yet
- I. EmergencyDocument10 pagesI. EmergencyGloryJaneNo ratings yet
- 10 Newborn1Document129 pages10 Newborn1Gerlian Kyle QueridoNo ratings yet
- CTG-skills LabDocument33 pagesCTG-skills Labjimwelluismagno27No ratings yet
- Emergency Nursing & Critical CareDocument74 pagesEmergency Nursing & Critical Carenursereview100% (14)
- Neonatal-Resuscitation Prog NRP 2023Document30 pagesNeonatal-Resuscitation Prog NRP 2023Shariti DeviNo ratings yet
- WISE 2019 NICU RepairedDocument209 pagesWISE 2019 NICU RepairedVanessa YunqueNo ratings yet
- Neonatal Resuscitation Power PointDocument29 pagesNeonatal Resuscitation Power PointsameerarswNo ratings yet
- Neonatal ResuscitationDocument38 pagesNeonatal Resuscitationramanand chaudharyNo ratings yet
- Asphyxia NeonatorumDocument34 pagesAsphyxia NeonatorumListya Paramita100% (1)
- Hyaline Membrane Disease-1Document24 pagesHyaline Membrane Disease-1JOSLIN100% (1)
- NRP - Ima-IsaDocument55 pagesNRP - Ima-IsaPeter RamNo ratings yet
- Pediatric Basic and Advanced Cardiac Life SupportDocument26 pagesPediatric Basic and Advanced Cardiac Life SupportZoe Jeanne GarcianoNo ratings yet
- European Resuscitation Council Guidelines 2021Document69 pagesEuropean Resuscitation Council Guidelines 2021Kiran PantheeNo ratings yet
- INFECTION Control and PREVENTION-1Document49 pagesINFECTION Control and PREVENTION-1Jerry AbleNo ratings yet
- Oxford Newborn Care Unit: Neonatal Equipment: Information For Parents and CarersDocument12 pagesOxford Newborn Care Unit: Neonatal Equipment: Information For Parents and CarersJerry AbleNo ratings yet
- Safety Guidelines For Chemotherapy and Radiation Therapy: By: Prof. Marites L. RoblezaDocument32 pagesSafety Guidelines For Chemotherapy and Radiation Therapy: By: Prof. Marites L. RoblezaJerry Able100% (1)
- Barriers To Online Learning in The Time of COVID-19: A National Survey of Medical Students in The PhilippinesDocument19 pagesBarriers To Online Learning in The Time of COVID-19: A National Survey of Medical Students in The PhilippinesJohn Paull CuaNo ratings yet
- Essential Antenatal, Perinatal and Postpartum Care: Training ModulesDocument392 pagesEssential Antenatal, Perinatal and Postpartum Care: Training ModulesReybs -isabella CalubNo ratings yet
- Informed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceDocument18 pagesInformed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceJerry AbleNo ratings yet
- Related Literature - New Normal Educatonal SystemDocument20 pagesRelated Literature - New Normal Educatonal SystemJerry AbleNo ratings yet
- Informed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceDocument18 pagesInformed Consent: Lena Haygood (R) RT Radiology Instructor: Arizona Western Community College SourceJerry AbleNo ratings yet
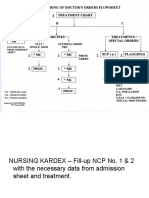
- Nursing Kardex and Treatment Chart SetupDocument21 pagesNursing Kardex and Treatment Chart SetupJerry AbleNo ratings yet
- The Learner Support System For Distance EducationDocument5 pagesThe Learner Support System For Distance EducationJerry AbleNo ratings yet
- INFECTION Control and PREVENTION-1Document49 pagesINFECTION Control and PREVENTION-1Jerry AbleNo ratings yet
- St. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideDocument14 pagesSt. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideJerry AbleNo ratings yet
- Emergency Red Flags: DR - Magdy Khames AlyDocument58 pagesEmergency Red Flags: DR - Magdy Khames AlyJerry AbleNo ratings yet
- Handbook On Facilitating Flexible LearningDocument54 pagesHandbook On Facilitating Flexible LearningJack Ricardo Sánchez Campo100% (1)
- Emergency Department Triage ProcessDocument27 pagesEmergency Department Triage ProcessJerry AbleNo ratings yet
- St. Anthony'S College - Nursing Department: Theoretical Foundations in NursingDocument86 pagesSt. Anthony'S College - Nursing Department: Theoretical Foundations in NursingCandido Kenneth JohnNo ratings yet
- Chronic Kidney Disease Pathophysiology Schematic DiagramDocument3 pagesChronic Kidney Disease Pathophysiology Schematic DiagramJerry AbleNo ratings yet
- St. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideDocument15 pagesSt. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideJerry AbleNo ratings yet
- OB - CPG Health Assessment 2018-2019Document21 pagesOB - CPG Health Assessment 2018-2019Jerry AbleNo ratings yet
- Able-Cordero NCM 103 CPGDocument36 pagesAble-Cordero NCM 103 CPGJerry AbleNo ratings yet
- Personalhygiene 120531235008 Phpapp01Document41 pagesPersonalhygiene 120531235008 Phpapp01Mar JinitaNo ratings yet
- St. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideDocument15 pagesSt. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideJerry AbleNo ratings yet
- St. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideDocument14 pagesSt. Anthony'S College San Jose, Antique: Outcomes-Based Curriculum Pacing GuideJerry AbleNo ratings yet
- Po1 Po2 Po3 Po4 Po5 Po6 Po7 Po8 Po9 Po10 Po11 Po12 Po13 Po14Document16 pagesPo1 Po2 Po3 Po4 Po5 Po6 Po7 Po8 Po9 Po10 Po11 Po12 Po13 Po14Jerry AbleNo ratings yet
- June 2012 Nurse Licensure Examination Results Performance of Nursing SchoolsDocument19 pagesJune 2012 Nurse Licensure Examination Results Performance of Nursing SchoolsRay Andrew del RosarioNo ratings yet
- Film ReviewDocument2 pagesFilm ReviewJerry AbleNo ratings yet
- WASH Guide for Teachers in EmergenciesDocument80 pagesWASH Guide for Teachers in EmergenciesJerry Able100% (1)
- Role Play - Rubric 1Document1 pageRole Play - Rubric 1Siti ShalihaNo ratings yet
- Leadership TheoryDocument31 pagesLeadership TheoryJerry AbleNo ratings yet
- 1851968974biology Class X For Sa-I 2015-16Document99 pages1851968974biology Class X For Sa-I 2015-16Afandi AmkajaNo ratings yet
- Mode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDateDocument16 pagesMode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDatedavimemNo ratings yet
- Impaired kidney function nursing careDocument21 pagesImpaired kidney function nursing careKate ManalastasNo ratings yet
- Exercises for Relaxing and Connecting in AfghanistanDocument33 pagesExercises for Relaxing and Connecting in AfghanistanPrincess ArceNo ratings yet
- CPT ChecklistDocument3 pagesCPT ChecklistMa. Angelica Alyssa RachoNo ratings yet
- The Superconscious MindDocument6 pagesThe Superconscious MindVictor LeeNo ratings yet
- (GHS - MSDS) TRIREX 3025N2 3556E (EN) 20171219 新Document7 pages(GHS - MSDS) TRIREX 3025N2 3556E (EN) 20171219 新DAVID LIMNo ratings yet
- Orgasm ControlDocument7 pagesOrgasm Controljulandrona100% (3)
- Day 1 PDFDocument5 pagesDay 1 PDFRavi NakarmiNo ratings yet
- Reading Comprehension Worksheets Key Science 4 PDFDocument13 pagesReading Comprehension Worksheets Key Science 4 PDFmbpmbpNo ratings yet
- Voice and DictionDocument13 pagesVoice and DictionAira NadineNo ratings yet
- hw499 Unit 8 Assignment Amartinez 2Document9 pageshw499 Unit 8 Assignment Amartinez 2api-698158741No ratings yet
- Inomax Manual de Operacion PDFDocument136 pagesInomax Manual de Operacion PDFalejandraNo ratings yet
- MTV 1000 VENTILADOR DE TRANSPORTE EMERGENCIADocument2 pagesMTV 1000 VENTILADOR DE TRANSPORTE EMERGENCIAFernando Trujillo100% (1)
- Sbar CommunicationDocument2 pagesSbar CommunicationSetina100% (1)
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternTrixie Anne Gamotin100% (3)
- Solutions Manual For Fluid Mechanics 5th PDFDocument20 pagesSolutions Manual For Fluid Mechanics 5th PDFchala nigussieNo ratings yet
- Biosys Biovent2020 enDocument11 pagesBiosys Biovent2020 enAmilcar Goyzueta100% (1)
- Updated One Manhyia HospitalDocument7 pagesUpdated One Manhyia HospitalJoseph Asare DuahNo ratings yet
- Neonatal ResuscitationDocument15 pagesNeonatal ResuscitationAmruta GadeNo ratings yet
- Suctioning HandoutsDocument3 pagesSuctioning HandoutsErika ArceoNo ratings yet
- Heart of London SanghaDocument9 pagesHeart of London SanghaEthan PollockNo ratings yet
- Free Meditation CourseDocument16 pagesFree Meditation CourseShallu ManchandaNo ratings yet
- Observing-Your-Breath Exercises For ParentsDocument2 pagesObserving-Your-Breath Exercises For ParentsrohailNo ratings yet
- Aromatherapy For The VoiceDocument4 pagesAromatherapy For The VoiceMegan Vivia van WykNo ratings yet
- Biol 1700 2019Document21 pagesBiol 1700 2019api-434583946No ratings yet
- Ashtanga Yoga Teacher Training Manual - ODKDocument85 pagesAshtanga Yoga Teacher Training Manual - ODKShana Flogie100% (3)
- NOTES CLASS7 L10 Respiration in Organisms-1Document6 pagesNOTES CLASS7 L10 Respiration in Organisms-1Blue PlayzNo ratings yet
- Safety Data Sheet Gelbrake (TM) 100: Product and Company Identification 1Document12 pagesSafety Data Sheet Gelbrake (TM) 100: Product and Company Identification 1izzybjNo ratings yet
- Adjustment To Extrauterine LifeDocument4 pagesAdjustment To Extrauterine LifeFrancine LaxaNo ratings yet