You might also like
- Criminal Court Complaint Michael Olaf Schuett Gambling Bluetool WirecardDocument46 pagesCriminal Court Complaint Michael Olaf Schuett Gambling Bluetool WirecardhandreaderNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Free Version of Growthinks Vending Machine Business Plan TemplateDocument16 pagesFree Version of Growthinks Vending Machine Business Plan TemplateswdNo ratings yet
- RV Bey Default Judgment Sent Regular Mail - 20170531 - 0002Document7 pagesRV Bey Default Judgment Sent Regular Mail - 20170531 - 0002PriyaSiranEL100% (1)
- NHIF Universal Claim Form 2020Document2 pagesNHIF Universal Claim Form 2020joyce akoth74% (34)
- Nutrition Therapy For Upper Gastrointestinal Disorders Case QuestionsDocument11 pagesNutrition Therapy For Upper Gastrointestinal Disorders Case QuestionspeytonNo ratings yet
- Muscle & Fittness: Resents TheDocument34 pagesMuscle & Fittness: Resents TheauqaabNo ratings yet
- Citibank V.dinopol, GR 188412Document7 pagesCitibank V.dinopol, GR 188412vylletteNo ratings yet
- Fla. Motion To Dismiss1 - Foreclosure - D.Graham Esq.Document4 pagesFla. Motion To Dismiss1 - Foreclosure - D.Graham Esq.winstons2311100% (1)
- Bloodstain Patterns: Identification, Interpretation and ApplicationFrom EverandBloodstain Patterns: Identification, Interpretation and ApplicationRating: 5 out of 5 stars5/5 (1)
- Urge Surfing HandoutDocument1 pageUrge Surfing HandoutRene McLaughlinNo ratings yet
- Feasibility Study 1Document69 pagesFeasibility Study 1Andre Christian Ang100% (2)
- India 2030 PDFDocument188 pagesIndia 2030 PDFGray HouserNo ratings yet
- Indian Goat Farm Project ReportDocument5 pagesIndian Goat Farm Project ReportTariq Shah71% (7)
- Natual Death - 0001Document6 pagesNatual Death - 0001punnyapoonam1No ratings yet
- Philippine Health Insurance reiteration of PD claims filingDocument2 pagesPhilippine Health Insurance reiteration of PD claims filingMox LexNo ratings yet
- Medical Report MR Ibrahim AktasDocument6 pagesMedical Report MR Ibrahim AktasNiraNo ratings yet
- Yuliya Keaton 1Document10 pagesYuliya Keaton 1MarcusBrutus9No ratings yet
- 1 1a9b31b333Document1 page1 1a9b31b333Ajay yadavNo ratings yet
- Mirabel Halikhik 02Document1 pageMirabel Halikhik 02Dexter FumarNo ratings yet
- eZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoDocument1 pageeZH Ealth: Dosage Seq. Date (Mm/dd/yyyy) Vaccine Brand Name of Vaccinator Batch No. Lot NoRvBombetaNo ratings yet
- Formulir Kiriman: FL FL LLDocument2 pagesFormulir Kiriman: FL FL LLVtrock The'IlectraNo ratings yet
- Gingivitis Treatment and Plaque Control ClinicDocument22 pagesGingivitis Treatment and Plaque Control ClinicSari Meliani SasmiNo ratings yet
- CASHLESS REQUEST FORMDocument2 pagesCASHLESS REQUEST FORMRaju.PalNo ratings yet
- Request: YagjmleDocument3 pagesRequest: YagjmleDorian FloresNo ratings yet
- Medical Insurance Claim RequestDocument2 pagesMedical Insurance Claim RequestSaeed FaizNo ratings yet
- Citizenship c3 c4Document5 pagesCitizenship c3 c4yinjian0001No ratings yet
- PhilHealth Form Simplifies EnrollmentDocument3 pagesPhilHealth Form Simplifies EnrollmentAngelo PalamingNo ratings yet
- People of The Philippines vs. Novo Tanes y BelmonteDocument14 pagesPeople of The Philippines vs. Novo Tanes y BelmontebogoldoyNo ratings yet
- Carlos Slay DocumentsDocument90 pagesCarlos Slay DocumentsPhil AmmannNo ratings yet
- Defendant Kevin Kelleher's Answer To Righthaven Complaint (Filed August 5, 2010)Document6 pagesDefendant Kevin Kelleher's Answer To Righthaven Complaint (Filed August 5, 2010)www.righthavenlawsuits.comNo ratings yet
- People vs. Ventura, G.R. No. L-15079Document5 pagesPeople vs. Ventura, G.R. No. L-15079Ina Villarica100% (1)
- Edilln"K: 1168011uu4468281 Card UerDocument6 pagesEdilln"K: 1168011uu4468281 Card UerD'sie Rose LagrosasNo ratings yet
- Acute Flaccid Paralysis Case FormDocument2 pagesAcute Flaccid Paralysis Case FormPaul Angelo E. Caliva0% (1)
- E D G V 16 - 0 5 8 S - 1: Case NumberDocument2 pagesE D G V 16 - 0 5 8 S - 1: Case NumberdiazNo ratings yet
- Ic Extract FormDocument1 pageIc Extract FormSyed DzafeerNo ratings yet
- PhilHealth Circular 11 Series of 2011Document6 pagesPhilHealth Circular 11 Series of 2011Pia VSNo ratings yet
- Blood Prescription and Administration Charts Whole - DC15081 - PDF 89212507Document7 pagesBlood Prescription and Administration Charts Whole - DC15081 - PDF 89212507Dawood MisbahNo ratings yet
- ,,.,R /A, Lt.Y: ? Re FLL - , Jj.Document3 pages,,.,R /A, Lt.Y: ? Re FLL - , Jj.Tehvul GarciaNo ratings yet
- (. Cum: Cif Bon, CF...., Owe I'DIC R: Rcer'""°" - .'"Is,"' W ', I!a E.ez, R, RssDocument1 page(. Cum: Cif Bon, CF...., Owe I'DIC R: Rcer'""°" - .'"Is,"' W ', I!a E.ez, R, RssLouisse Vivien Santos LopezNo ratings yet
- SOP For HelplineDocument8 pagesSOP For Helplinemahender singhNo ratings yet
- Percentage Differently AbledDocument10 pagesPercentage Differently Abledayushbgmi6232No ratings yet
- Final DeclarationDocument9 pagesFinal Declarationsasta jiNo ratings yet
- 53 People VS LimsonDocument2 pages53 People VS LimsonEun Ae YinNo ratings yet
- Mental Health Court ApplicationDocument5 pagesMental Health Court ApplicationAshley GoodmanNo ratings yet
- CTA upholds dismissal of Hedcor's P4.2M VAT refund claimDocument7 pagesCTA upholds dismissal of Hedcor's P4.2M VAT refund claimClaire RoxasNo ratings yet
- Remittance Application FormDocument2 pagesRemittance Application FormasifwtNo ratings yet
- Vaccination or ProphylaxisDocument2 pagesVaccination or ProphylaxisUtira ChenNo ratings yet
- Binary Solutions Pvt. Ltd.Document1 pageBinary Solutions Pvt. Ltd.SouravDasNo ratings yet
- RDS W9 2023Document1 pageRDS W9 2023juyla5479No ratings yet
- A Legal Requirement: Reporting Suspicious TransactionsDocument4 pagesA Legal Requirement: Reporting Suspicious TransactionsM Kaleem AbidNo ratings yet
- DI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEDocument12 pagesDI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEsandeepNo ratings yet
- Memo For Brokers: I / Z SecurrnesDocument32 pagesMemo For Brokers: I / Z SecurrnesRenEleponioNo ratings yet
- South African. Serv) Ce: PoliceDocument7 pagesSouth African. Serv) Ce: PoliceSagwadi Mastermind MalulekeNo ratings yet
- Scan10001 PDFDocument1 pageScan10001 PDFgraceNo ratings yet
- Toyota Liable for Unpaid Commissions Despite Justified FiringDocument8 pagesToyota Liable for Unpaid Commissions Despite Justified FiringAnnabelle BustamanteNo ratings yet
- R-Tinistry of Personnel, Public .Gi ",ievances Pensions Pensione, Rs WelfarejDocument2 pagesR-Tinistry of Personnel, Public .Gi ",ievances Pensions Pensione, Rs WelfarejNikhil BisuiNo ratings yet
- P2 P6 ClaimformDocument5 pagesP2 P6 ClaimformDevesh KhandareNo ratings yet
- IMG_0002Document2 pagesIMG_0002gopalakrishna panugantiNo ratings yet
- Hartman Court DocumentsDocument9 pagesHartman Court DocumentsWSETNo ratings yet
- Uni Versi Ty Of The Punj Ab: Ti Ree夕Document15 pagesUni Versi Ty Of The Punj Ab: Ti Ree夕saditha manjulahariNo ratings yet
- Cta 00 CV 03887 D 1988may31 RefDocument7 pagesCta 00 CV 03887 D 1988may31 RefNorjanisa DimaroNo ratings yet
- Hayne DPS Chief Pathologist ContractDocument7 pagesHayne DPS Chief Pathologist ContractMatt EichelbergerNo ratings yet
- Medical Bill Format of HESCOMDocument2 pagesMedical Bill Format of HESCOMEEE50% (2)
- The Nursing Process OverviewDocument26 pagesThe Nursing Process OverviewAYO NELSONNo ratings yet
- Solicitud de Material (Actualizado Al 01 de Diciembre 2020) Teleredes 1Document151 pagesSolicitud de Material (Actualizado Al 01 de Diciembre 2020) Teleredes 1Jjdfyiseth AmayajjdfNo ratings yet
- Turkey's Growing Healthcare Sector Driven by Private ProvidersDocument69 pagesTurkey's Growing Healthcare Sector Driven by Private ProviderssbulenterisNo ratings yet
- HR Selection Process & Global PerspectivesDocument30 pagesHR Selection Process & Global PerspectivesOsei Kwame PhilipNo ratings yet
- MIDAS QuestionnaireDocument1 pageMIDAS QuestionnaireNHFChicagoNo ratings yet
- Mapeh 10 QuizDocument1 pageMapeh 10 QuizMichelle Dela RosaNo ratings yet
- SEMI FINAL FINAL NCM 113 NotesDocument1 pageSEMI FINAL FINAL NCM 113 Notesmblanco.dchNo ratings yet
- SBFP Form 1 2021 Cebu Province Tubod Elementary SchoolDocument23 pagesSBFP Form 1 2021 Cebu Province Tubod Elementary SchoolJane Rodriguez LumacangNo ratings yet
- Zimmer Cemented CPTDocument20 pagesZimmer Cemented CPTJayjeet BhoiteNo ratings yet
- CrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)Document5 pagesCrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)TUTOR PAULO EDUARDO REDKVANo ratings yet
- SRNT 2015 Abstracts WEBDocument362 pagesSRNT 2015 Abstracts WEBSatya Ashok KumarNo ratings yet
- The Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032Document18 pagesThe Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032ArtemisNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
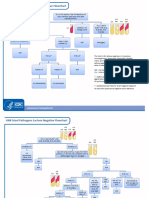
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- 9 ErDocument13 pages9 Ermartin Ignacio Zapata LaguadoNo ratings yet
- What Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasDocument24 pagesWhat Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasAisa VenturaNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- EMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Document17 pagesEMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Saka FelistarNo ratings yet
- DSP 15-12-23Document36 pagesDSP 15-12-23Fu'ad ParkhaniNo ratings yet
- Pe HRF 8Document3 pagesPe HRF 8Jefferson GonzalesNo ratings yet
- Dec 2 2022 Cot 1Document54 pagesDec 2 2022 Cot 1Estela AnchetaNo ratings yet
- Hospital Business ModelsDocument8 pagesHospital Business ModelsPOLOKO MHUSIWANo ratings yet