You might also like
- Peds 2013-2958Document11 pagesPeds 2013-2958Sean SubtesteNo ratings yet
- Cognitive Behavioral Interventions For Sexually Abused Children Exhibiting PTSD SymptomatologyDocument15 pagesCognitive Behavioral Interventions For Sexually Abused Children Exhibiting PTSD SymptomatologyalmaNo ratings yet
- CBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyDocument12 pagesCBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyWildan AnrianNo ratings yet
- GLOSSARY (Communication Skills Terms)Document12 pagesGLOSSARY (Communication Skills Terms)Janie100% (1)
- Atlas Cancer CervicalDocument458 pagesAtlas Cancer CervicalihsansabridrNo ratings yet
- Impact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenDocument10 pagesImpact of Executive Function Deficits and Attention-Deficit/Hyperactivity Disorder (ADHD) On Academic Outcomes in ChildrenEunice_Pinto_1725No ratings yet
- The Effects of Divorce on Children: A Mother-Son PerspectiveFrom EverandThe Effects of Divorce on Children: A Mother-Son PerspectiveNo ratings yet
- Laoang Elementary School School Boy Scout Action Plan Objectives Activities Time Frame Persons Involve Resources NeededDocument3 pagesLaoang Elementary School School Boy Scout Action Plan Objectives Activities Time Frame Persons Involve Resources NeededMillie Lagonilla100% (5)
- Istqb Questions and AnswersDocument105 pagesIstqb Questions and Answersnrguru_sun100% (1)
- Lesson PlanDocument8 pagesLesson PlanMarvi Joyce Caballero100% (1)
- Importance of Philippine HistoryDocument2 pagesImportance of Philippine HistoryJoyce Peñaescocia100% (2)
- Chang 2018Document14 pagesChang 2018spaciugNo ratings yet
- Anselmi 2008Document9 pagesAnselmi 2008Elton MatsushimaNo ratings yet
- Psychopathology in Non-Clinically Referred Sexually Abused Children - Mcleer, S. V. Et. Al.Document8 pagesPsychopathology in Non-Clinically Referred Sexually Abused Children - Mcleer, S. V. Et. Al.martiinrv100% (1)
- Brief ReportDocument6 pagesBrief Reportsebastoto778No ratings yet
- Prevalence and Genetic Architecture of Child Behavior Checklist-Juvenile Bipolar DisorderDocument7 pagesPrevalence and Genetic Architecture of Child Behavior Checklist-Juvenile Bipolar DisorderOana MarcociNo ratings yet
- 1 s2.0 S0022395606001981 MainDocument9 pages1 s2.0 S0022395606001981 MainCláudia Isabel SilvaNo ratings yet
- 1 s2.0 S0306453018302968 MainDocument6 pages1 s2.0 S0306453018302968 MainSamuelRexyNo ratings yet
- Sex Differences in The Developmental Trajectories of Autism SpectrumDocument12 pagesSex Differences in The Developmental Trajectories of Autism SpectrumBárbaraLaureanoNo ratings yet
- Gender Variance Among Youth With Autism Spectrum Disorders: A Retrospective Chart ReviewDocument7 pagesGender Variance Among Youth With Autism Spectrum Disorders: A Retrospective Chart ReviewMilo DueNo ratings yet
- Janssen 2016Document6 pagesJanssen 2016Carla VieiraNo ratings yet
- 2002-Conversion Disorder in Children and Adolescents A 4-Year Follow-Up StudyDocument5 pages2002-Conversion Disorder in Children and Adolescents A 4-Year Follow-Up StudyJuan Francisco YelaNo ratings yet
- Cognitive Distortions and Psychiatric Diagnosis in Dually Diagnosed AdolescentsDocument6 pagesCognitive Distortions and Psychiatric Diagnosis in Dually Diagnosed AdolescentsBosondos BedooNo ratings yet
- Impact of Early Medical Treatment For Transgender Youth: Protocol For The Longitudinal, Observational Trans Youth Care StudyDocument10 pagesImpact of Early Medical Treatment For Transgender Youth: Protocol For The Longitudinal, Observational Trans Youth Care StudycatalinavillenaNo ratings yet
- Short StatureDocument15 pagesShort Staturedr. YofaniNo ratings yet
- Dialectical Behavior Therapy of Anorexia and Bulimia Nervosa Among Adolescents A Case SeriesDocument11 pagesDialectical Behavior Therapy of Anorexia and Bulimia Nervosa Among Adolescents A Case SeriesMarietta_MonariNo ratings yet
- Pediatrics 129 No.3Document8 pagesPediatrics 129 No.3cdsaludNo ratings yet
- 2019 Article 1336Document6 pages2019 Article 1336Eduardo LimaNo ratings yet
- CPR5Document20 pagesCPR5Laura HdaNo ratings yet
- Caspi Et Al - Genes and Its Influence On BehaviorDocument2 pagesCaspi Et Al - Genes and Its Influence On Behaviorlavannya aNo ratings yet
- Cortisol and ACTH Responses To The Dex/CRH Test: Influence of TemperamentDocument8 pagesCortisol and ACTH Responses To The Dex/CRH Test: Influence of TemperamentFrontiersNo ratings yet
- Obsessive-Compulsive Disorder: Retrospective Study On Clinical Characteristics and Family History in Outpatients CareDocument8 pagesObsessive-Compulsive Disorder: Retrospective Study On Clinical Characteristics and Family History in Outpatients CareTJPRC PublicationsNo ratings yet
- An Investigation of Health Anxiety in FamiliesDocument12 pagesAn Investigation of Health Anxiety in FamiliesAndreea NicolaeNo ratings yet
- Children and Adolescents With Gender Identity Disorder Referred To A Pediatric Medical CenterDocument10 pagesChildren and Adolescents With Gender Identity Disorder Referred To A Pediatric Medical CenterusernarcisaNo ratings yet
- Crissman Et Al DSD Parent Experience 2011Document11 pagesCrissman Et Al DSD Parent Experience 2011windawindut94No ratings yet
- Kaminski Clausse (2017)Document24 pagesKaminski Clausse (2017)Nuria Moreno RománNo ratings yet
- Ocd Family TXDocument12 pagesOcd Family TXdnutter012576No ratings yet
- Caspi Et Al 2003 - 1Document1 pageCaspi Et Al 2003 - 1oliventeroNo ratings yet
- Psychiatric Characterization of Children With Genetic Causes of HyperandrogenismDocument10 pagesPsychiatric Characterization of Children With Genetic Causes of HyperandrogenismnigoNo ratings yet
- CJP May 06 Nickel OR5Document8 pagesCJP May 06 Nickel OR5haddig8No ratings yet
- Factor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisDocument9 pagesFactor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisCris RodriguesNo ratings yet
- Male Fertility psychiatricPIIS0015028211028032Document6 pagesMale Fertility psychiatricPIIS0015028211028032annisa habibullohNo ratings yet
- The Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To ChildDocument12 pagesThe Behavior of Anxious Parents Examining Mechanisms of Transmission of Anxiety From Parent To Child方科惠No ratings yet
- Body Dissatisfaction and Mental HealthDocument9 pagesBody Dissatisfaction and Mental HealthBammy SiriratNo ratings yet
- E541 FullDocument9 pagesE541 FullAlba VilaNo ratings yet
- Child Psychology Psychiatry - 2012 - Simonoff - Severe Mood Problems in Adolescents With Autism Spectrum DisorderDocument10 pagesChild Psychology Psychiatry - 2012 - Simonoff - Severe Mood Problems in Adolescents With Autism Spectrum DisorderlidiaNo ratings yet
- Ni Hms 45279Document14 pagesNi Hms 45279Espíritu CiudadanoNo ratings yet
- Appi Ajp 157 6 917Document7 pagesAppi Ajp 157 6 917crismg1No ratings yet
- 2007 - III. The Current StudyDocument12 pages2007 - III. The Current Studyjennyhe0819No ratings yet
- Analyze The Following: What Do You Think? Using The Text, Explain The Three Components of HardinessDocument3 pagesAnalyze The Following: What Do You Think? Using The Text, Explain The Three Components of HardinessMaria Camila Vangh-egas JNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptCorina IoanaNo ratings yet
- American J of Med Genetics PT B - 2018 - Piedimonte - Exploring Relationships Between Joint Hypermobility andDocument11 pagesAmerican J of Med Genetics PT B - 2018 - Piedimonte - Exploring Relationships Between Joint Hypermobility andKarel GuevaraNo ratings yet
- Adams - 2018 - Well-Being in Mothers of Children With Rare Genetic SyndromesDocument13 pagesAdams - 2018 - Well-Being in Mothers of Children With Rare Genetic SyndromesPetrutaNo ratings yet
- 1 s2.0 S0306453016307909 MainDocument4 pages1 s2.0 S0306453016307909 Mainloic.chevalley2No ratings yet
- The Department of Psychology Within A Pediatric Cardiac Transplant UnitDocument4 pagesThe Department of Psychology Within A Pediatric Cardiac Transplant UnitSanziana SavaNo ratings yet
- Bryson, Zwaigenbaum Et Al 2007Document13 pagesBryson, Zwaigenbaum Et Al 2007mariaNo ratings yet
- The Stability of Problem Behavior Across The Preschool Years An Empirical Approach in The General PopulationDocument12 pagesThe Stability of Problem Behavior Across The Preschool Years An Empirical Approach in The General Populationyanfang liNo ratings yet
- Συννοσηρή Ψυχοπαθολογία Και Κλινική Συμπτωματολογία Σε Παιδιά Και Εφήβους Με Ιδεοψυχαναγκαστική ΔιαταραχήDocument10 pagesΣυννοσηρή Ψυχοπαθολογία Και Κλινική Συμπτωματολογία Σε Παιδιά Και Εφήβους Με Ιδεοψυχαναγκαστική ΔιαταραχήEviKapaNo ratings yet
- Long-Term OutcomesDocument20 pagesLong-Term OutcomesCorina IoanaNo ratings yet
- Influence of Child Abuse On Adult Depression: Moderation by The Corticotropin-Releasing Hormone Receptor GeneDocument11 pagesInfluence of Child Abuse On Adult Depression: Moderation by The Corticotropin-Releasing Hormone Receptor GeneDian Sulistya EkaputriNo ratings yet
- Análisis Factorial y Prueba de Invarianza de Medición Longitudinal Del Inventario de Depresión Infantil (CDI) en La Adolescencia - 2019Document7 pagesAnálisis Factorial y Prueba de Invarianza de Medición Longitudinal Del Inventario de Depresión Infantil (CDI) en La Adolescencia - 2019Anonymous 7YP3VYNo ratings yet
- Is ADHD A Risk For Posttraumatic Stress Disorder PTSD Results From A Large Longitudinal Study of Referred Children With and Without ADHDDocument8 pagesIs ADHD A Risk For Posttraumatic Stress Disorder PTSD Results From A Large Longitudinal Study of Referred Children With and Without ADHDKyle RossNo ratings yet
- Clinical Features of Young Children Referred For Impairing Temper OutburstsDocument9 pagesClinical Features of Young Children Referred For Impairing Temper OutburstsRafael MartinsNo ratings yet
- Insecure Attachment in Severely Asthmatic Preschool ChildrenDocument5 pagesInsecure Attachment in Severely Asthmatic Preschool ChildrenMatt Van VelsenNo ratings yet
- Allen, 2017 - TFCBTDocument10 pagesAllen, 2017 - TFCBTOlga MichailidouNo ratings yet
- Social and Communication Development in Toddlers With Early and Later Diagnosis of Autism Spectrum DisordersDocument12 pagesSocial and Communication Development in Toddlers With Early and Later Diagnosis of Autism Spectrum DisordersPancha IabNo ratings yet
- McDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFDocument9 pagesMcDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFCristian jimènezNo ratings yet
- Conjunction With Palliative Radiotherapy ForDocument9 pagesConjunction With Palliative Radiotherapy ForihsansabridrNo ratings yet
- Effects of Hypnosis, Cognitive Therapy, HypnoticDocument15 pagesEffects of Hypnosis, Cognitive Therapy, HypnoticihsansabridrNo ratings yet
- Suicidal SI and Suicide in Depressed Adolescent Impact of Peer Victimization and BullyingDocument25 pagesSuicidal SI and Suicide in Depressed Adolescent Impact of Peer Victimization and BullyingihsansabridrNo ratings yet
- PAP TEST Criterios 2020Document26 pagesPAP TEST Criterios 2020Geovanna BorjaNo ratings yet
- Care of Women With Invasive Cervical CancerDocument30 pagesCare of Women With Invasive Cervical CancerihsansabridrNo ratings yet
- Hypnosedation CervixDocument8 pagesHypnosedation CervixihsansabridrNo ratings yet
- Schizophrenia ResearchDocument9 pagesSchizophrenia ResearchihsansabridrNo ratings yet
- Visceral and Somatic Pain Modalities RevealDocument54 pagesVisceral and Somatic Pain Modalities RevealihsansabridrNo ratings yet
- Results of A Phase I-II Study On Laser TherapyDocument12 pagesResults of A Phase I-II Study On Laser TherapyihsansabridrNo ratings yet
- J Bullying 8Document10 pagesJ Bullying 8ihsansabridrNo ratings yet
- Ilovepdf MergedDocument23 pagesIlovepdf MergedihsansabridrNo ratings yet
- The Impact of Dementia On The ClinicalDocument8 pagesThe Impact of Dementia On The ClinicalihsansabridrNo ratings yet
- Chemotherapy-Induced Neuroinflammation Is Associated With Disrupted Colonic and Bacterial Homeostasis in Female MiceDocument16 pagesChemotherapy-Induced Neuroinflammation Is Associated With Disrupted Colonic and Bacterial Homeostasis in Female MiceihsansabridrNo ratings yet
- Chemotherapy-Enhanced Inflammation May Lead To The Failure of Therapy and MetastasisDocument9 pagesChemotherapy-Enhanced Inflammation May Lead To The Failure of Therapy and MetastasisihsansabridrNo ratings yet
- J Bullying 2Document13 pagesJ Bullying 2ihsansabridrNo ratings yet
- Jurnal 35Document7 pagesJurnal 35ihsansabridrNo ratings yet
- J Bullying 4Document15 pagesJ Bullying 4ihsansabridrNo ratings yet
- Jurnal 36Document23 pagesJurnal 36ihsansabridrNo ratings yet
- Cancer Statistics 2019Document28 pagesCancer Statistics 2019marcellojunNo ratings yet
- Associations Between Chinese Adolescents Subjected To Traditional and Cyber Bullying and Suicidal Ideation, Self-Harm and Suicide AttemptsDocument8 pagesAssociations Between Chinese Adolescents Subjected To Traditional and Cyber Bullying and Suicidal Ideation, Self-Harm and Suicide AttemptsNurul Fatehah Binti KamaruzaliNo ratings yet
- Raja 2020Document7 pagesRaja 2020Julian GorositoNo ratings yet
- J Bullying 1Document11 pagesJ Bullying 1ihsansabridrNo ratings yet
- McDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFDocument9 pagesMcDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFCristian jimènezNo ratings yet
- Eliminating Stroop Effects With Post-Hypnotic Instructions BrainDocument8 pagesEliminating Stroop Effects With Post-Hypnotic Instructions BrainihsansabridrNo ratings yet
- Chronic Pain Disrupts Ability To Work by Interfering With SocialDocument6 pagesChronic Pain Disrupts Ability To Work by Interfering With SocialihsansabridrNo ratings yet
- Clinical Hypnosis in Paediatric OncologyDocument7 pagesClinical Hypnosis in Paediatric OncologyihsansabridrNo ratings yet
- Conjunction With Palliative Radiotherapy ForDocument9 pagesConjunction With Palliative Radiotherapy ForihsansabridrNo ratings yet
- Chronic Pain As A Symptom IASPDocument9 pagesChronic Pain As A Symptom IASPihsansabridrNo ratings yet
- ch14Document7 pagesch14Ahmed AliNo ratings yet
- Rochester College Lesson Plan TemplateDocument14 pagesRochester College Lesson Plan Templateapi-348350634No ratings yet
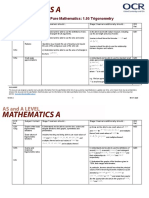
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 pagesTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyNo ratings yet
- PDP Report ExampleDocument41 pagesPDP Report ExampleDipaa LakshmiNo ratings yet
- Godrej Interio Education Range Dossier 2023-24 - v1 WebDocument138 pagesGodrej Interio Education Range Dossier 2023-24 - v1 WebSingareni power training Institute (SPTI)No ratings yet
- Literature Review Template: Writing CentreDocument1 pageLiterature Review Template: Writing CentreSyed Imam BakharNo ratings yet
- English IV: 3 Partial Week 4Document17 pagesEnglish IV: 3 Partial Week 4Luis Manuel GonzálezNo ratings yet
- Books - MY - JOURNEY - IN - SCIENCE - Autobiography - of - An Indian Scientist - Hardev Singh Virk PDFDocument216 pagesBooks - MY - JOURNEY - IN - SCIENCE - Autobiography - of - An Indian Scientist - Hardev Singh Virk PDFHarjinder Singh DhaliwalNo ratings yet
- Anderson Piano Syllabus 2020-2021Document5 pagesAnderson Piano Syllabus 2020-2021Desmond AndersonNo ratings yet
- Building Blocks of Vedic AstrologyDocument4 pagesBuilding Blocks of Vedic AstrologySrinath PrabhakarNo ratings yet
- Draft MC 2019Document8 pagesDraft MC 2019Simran GillNo ratings yet
- Experience 5 Year: Career SummaryDocument2 pagesExperience 5 Year: Career SummaryAshok SharmaNo ratings yet
- 1.3 Compare One'S Pecs With Those of A Practitioner/Entrepreneur 1.4 Align One'S Pecs With Those of A Practitioner/EntrepreneurDocument3 pages1.3 Compare One'S Pecs With Those of A Practitioner/Entrepreneur 1.4 Align One'S Pecs With Those of A Practitioner/EntrepreneurNoli ZamoraNo ratings yet
- Sow SPS201 NagoorDocument4 pagesSow SPS201 NagoorRose Ann ChanNo ratings yet
- Tablante, Caesar Cyril L.-UpdDocument1 pageTablante, Caesar Cyril L.-UpdCaesar Cyril TablanteNo ratings yet
- Stress and Anxiety: Essay SampleDocument3 pagesStress and Anxiety: Essay SampleAshley Jane MacapayadNo ratings yet
- Chapter - Motivation: Md. Imran Hossain Assistant Professor Dept: of Finance Jagannath UniversityDocument43 pagesChapter - Motivation: Md. Imran Hossain Assistant Professor Dept: of Finance Jagannath Universityjh shuvoNo ratings yet
- PRACTICAL RESEARCH PAPER 1111111 IiidoloDocument32 pagesPRACTICAL RESEARCH PAPER 1111111 Iiidoloskylark fannyNo ratings yet
- 10 Quality Engineer Interview Questions and AnswersDocument7 pages10 Quality Engineer Interview Questions and AnswersniensjvrNo ratings yet
- English ProjectDocument15 pagesEnglish Projectpranit.saluja.ps.2324No ratings yet
- Music Discoveries: Discover More at The ShopDocument3 pagesMusic Discoveries: Discover More at The ShopyolandaferniNo ratings yet
- JCLP 23114Document12 pagesJCLP 23114Rachel Wakefield-DrohanNo ratings yet
- Balwinder Kaur-MlsDocument2 pagesBalwinder Kaur-Mlsharjeet aulakhNo ratings yet
- Anatomy and Surgical Approaches To Lateral VentriclesDocument39 pagesAnatomy and Surgical Approaches To Lateral VentriclesKaramsi Gopinath NaikNo ratings yet
- Edci 514 Lesson Plan PWP Module 3Document10 pagesEdci 514 Lesson Plan PWP Module 3api-265028034No ratings yet