You might also like
- Congenital Cataract-Approach and Management ReviewDocument6 pagesCongenital Cataract-Approach and Management ReviewFirgietaPotterNo ratings yet
- Basic Eye ExamDocument8 pagesBasic Eye ExamLisa AguilarNo ratings yet
- Childhood Cataracts: Aetiology and Management: Indian Supplement Editorial BoardDocument4 pagesChildhood Cataracts: Aetiology and Management: Indian Supplement Editorial Boardnugroho2212No ratings yet
- Childhood Cataracts and Other JadiDocument49 pagesChildhood Cataracts and Other JadiSania NadianisaNo ratings yet
- Student Handbook Orthoptics.Document13 pagesStudent Handbook Orthoptics.Nur AminNo ratings yet
- Fact Sheet Optic Nerve AtrophyDocument4 pagesFact Sheet Optic Nerve Atrophyaryans1976No ratings yet
- Corneal Opacities in The Neonate: Education GapsDocument10 pagesCorneal Opacities in The Neonate: Education GapsOMAR ORENo ratings yet
- Congenital Cataract GuideDocument18 pagesCongenital Cataract GuideMohamad Hafyfy75% (4)
- Policy Statement Red Reflex Examination in Neonates, Infants and ChildrenDocument6 pagesPolicy Statement Red Reflex Examination in Neonates, Infants and ChildrenLore Sirpa MNo ratings yet
- Literature Review On Refractive ErrorsDocument5 pagesLiterature Review On Refractive Errorsafmzfvlopbchbe100% (1)
- Congenital Preventable Blindness: of ChildDocument4 pagesCongenital Preventable Blindness: of ChildJustin Michal DassNo ratings yet
- Eye Assessment: OptometristsDocument8 pagesEye Assessment: OptometristsLiam MaghanoyNo ratings yet
- Jurnal MataDocument8 pagesJurnal MatamarinarizkiNo ratings yet
- 1403-Einstein v7n3p376-82 PDFDocument7 pages1403-Einstein v7n3p376-82 PDFsuzela widya sariNo ratings yet
- Current Management of Childhood Amblyopia: Shin Hae ParkDocument12 pagesCurrent Management of Childhood Amblyopia: Shin Hae ParkSyarifah Thalita NabillaNo ratings yet
- Journal Article 5 48Document3 pagesJournal Article 5 48LorenaNo ratings yet
- Clinical and Experimental Advances in Congenital and Paediatric CataractsDocument16 pagesClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiNo ratings yet
- 1 - MyopiaDocument9 pages1 - MyopiaSpislgal PhilipNo ratings yet
- BIOLOGY INVESTIGATORY - Docx2.oDocument27 pagesBIOLOGY INVESTIGATORY - Docx2.oK GhatageNo ratings yet
- Guidelines for Prescribing Eyeglasses in Young ChildrenDocument18 pagesGuidelines for Prescribing Eyeglasses in Young Childrenratujelita100% (1)
- Blurred VisionDocument7 pagesBlurred VisionRichi CiriacoNo ratings yet
- Cortical BlindnessDocument2 pagesCortical BlindnessAmal AlmutiriNo ratings yet
- Pediatric Vision Screening For The Family PhysicianDocument15 pagesPediatric Vision Screening For The Family PhysicianPaula LottiNo ratings yet
- Anterior Segment Examination: 15 Section II. Comprehensive Ophthalmic EvaluationDocument6 pagesAnterior Segment Examination: 15 Section II. Comprehensive Ophthalmic EvaluationRaulLopezJaimeNo ratings yet
- Name - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreDocument11 pagesName - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreKrishna ChouhanNo ratings yet
- Diagnosis BandingDocument10 pagesDiagnosis BandingIntan Rahmi NasyaNo ratings yet
- Protrusion OjoDocument16 pagesProtrusion OjoAntonio ReaNo ratings yet
- Childhood GlaucomaDocument60 pagesChildhood Glaucomaeyemd_in_training100% (1)
- Ocular Emergencies 2017Document18 pagesOcular Emergencies 2017Sebastian BarreraNo ratings yet
- Strabismus: Kammi B. Gunton,, Barry N. Wasserman,, Caroline DebenedictisDocument15 pagesStrabismus: Kammi B. Gunton,, Barry N. Wasserman,, Caroline DebenedictisWendy Garduño SandovalNo ratings yet
- StrabismusDocument27 pagesStrabismuspason1988No ratings yet
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectGopikrishna united67% (3)
- Eye Infections PDFDocument10 pagesEye Infections PDFDara Agusti MaulidyaNo ratings yet
- Reffractive ErrorsDocument13 pagesReffractive ErrorsSagiraju SrinuNo ratings yet
- Cataract PTDocument9 pagesCataract PTPreeti SharmaNo ratings yet
- Cataract PTDocument9 pagesCataract PTpreeti sharmaNo ratings yet
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsFrom EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsNo ratings yet
- Pediatr Clin Na 2014 Jun 61 (3) 495Document9 pagesPediatr Clin Na 2014 Jun 61 (3) 495mickymed_No ratings yet
- Background: FrequencyDocument10 pagesBackground: FrequencyJenylia HapsariNo ratings yet
- New Rich Text DocumentDocument4 pagesNew Rich Text DocumentAisha TahirNo ratings yet
- Year MSC Optometry Student) : University of Gondar Cmhs Departement of OptometryDocument63 pagesYear MSC Optometry Student) : University of Gondar Cmhs Departement of Optometryhaymanot aynalemNo ratings yet
- MR 180 EditedDocument6 pagesMR 180 EditedfatmadianaNo ratings yet
- Pediatric Eye Exam Guide for ParentsDocument14 pagesPediatric Eye Exam Guide for ParentsDrSyed Rahil IqbalNo ratings yet
- Vitreous Floaters: Publication DetailsDocument6 pagesVitreous Floaters: Publication Detailsmithaa octoviagnesNo ratings yet
- Ocular Pathology of Hyperopic Patients Presenting To The Tertiary Health Care CentreDocument7 pagesOcular Pathology of Hyperopic Patients Presenting To The Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- 1 s2.0 S2352396421001535 MainDocument13 pages1 s2.0 S2352396421001535 MainAmy Lalringhluani ChhakchhuakNo ratings yet
- Investrigatory Project (Term I) : Subject - BIOLOGYDocument20 pagesInvestrigatory Project (Term I) : Subject - BIOLOGYRehan RazaNo ratings yet
- Myopia by NamanDocument19 pagesMyopia by NamanAkshit ChitkaraNo ratings yet
- Optokinetic Nystagmus TestDocument3 pagesOptokinetic Nystagmus TestRegina CaeciliaNo ratings yet
- Medical Case of Retinoblastoma in a 2-Year Old ChildDocument14 pagesMedical Case of Retinoblastoma in a 2-Year Old ChildRafieLugassektiNo ratings yet
- Prevalence and Progression of Myopia in Children at RaipurDocument9 pagesPrevalence and Progression of Myopia in Children at RaipurInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Infantile Leukocoria The White Pupil PDFDocument4 pagesInfantile Leukocoria The White Pupil PDFDian HapsariNo ratings yet
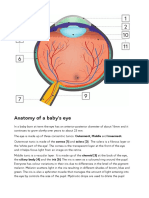
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocument2 pagesAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverNo ratings yet
- Pediatric Optic Neuritis 2016 PDFDocument7 pagesPediatric Optic Neuritis 2016 PDFangelia beanddaNo ratings yet
- Senile Cataract Clinical Presentation and CausesDocument4 pagesSenile Cataract Clinical Presentation and CausesAhmad FahroziNo ratings yet
- Senile Cataract Clinical Presentation and CausesDocument4 pagesSenile Cataract Clinical Presentation and CausesAhmad Fahrozi100% (1)
- Leung Et Al-2018-Clinical and Experimental OptometryDocument9 pagesLeung Et Al-2018-Clinical and Experimental Optometryangeles sanchez clariaNo ratings yet
- Study of Vision Screening in School Children Between 5 and 15 YearsDocument16 pagesStudy of Vision Screening in School Children Between 5 and 15 YearsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Guia Nice de Cad 2020Document15 pagesGuia Nice de Cad 2020Laura Camila ParraNo ratings yet
- (1479683X - European Journal of Endocrinology) Subclinical Hypothyroidism - To Treat or Not To TreatDocument10 pages(1479683X - European Journal of Endocrinology) Subclinical Hypothyroidism - To Treat or Not To TreatXimena ParedesNo ratings yet
- Management of Edema in NSDocument8 pagesManagement of Edema in NSmNo ratings yet
- Acute Kidney Injury Diagnosis and Management in ChildrenDocument8 pagesAcute Kidney Injury Diagnosis and Management in ChildrensrikandiNo ratings yet
- Acute Otitis Media in Children. BJM 2020 OkDocument8 pagesAcute Otitis Media in Children. BJM 2020 OkXimena ParedesNo ratings yet
- CostEffectiveness of Nasal High Flow Versus CPAP For Newborn. PEDIATRICS AGOST 2021 OKDocument11 pagesCostEffectiveness of Nasal High Flow Versus CPAP For Newborn. PEDIATRICS AGOST 2021 OKXimena ParedesNo ratings yet
- Early Use of Bronchodilators and Outcomes in Bronchiolitis. PEDIATRICS AGOST 2021 OK OKDocument9 pagesEarly Use of Bronchodilators and Outcomes in Bronchiolitis. PEDIATRICS AGOST 2021 OK OKXimena ParedesNo ratings yet
- Pancreatitis: Education GapsDocument13 pagesPancreatitis: Education GapsXimena ParedesNo ratings yet
- Pediatric Neurology: Jordan Cole, MD, Emily Evans, MD, Martin Mwangi, MD, Soe Mar, MDDocument9 pagesPediatric Neurology: Jordan Cole, MD, Emily Evans, MD, Martin Mwangi, MD, Soe Mar, MDXimena ParedesNo ratings yet
- Acute Otitis Media in Children. BJM 2020 OkDocument8 pagesAcute Otitis Media in Children. BJM 2020 OkXimena ParedesNo ratings yet
- Influence of HT On The Development of Thyroid Nodules and CancerDocument10 pagesInfluence of HT On The Development of Thyroid Nodules and CancerXimena ParedesNo ratings yet
- Acute Otitis Media in Children. BJM 2020 OkDocument8 pagesAcute Otitis Media in Children. BJM 2020 OkXimena ParedesNo ratings yet
- Guia Nice de Cad 2020Document15 pagesGuia Nice de Cad 2020Laura Camila ParraNo ratings yet
- Acute Otitis Media in Children. BJM 2020 OkDocument8 pagesAcute Otitis Media in Children. BJM 2020 OkXimena ParedesNo ratings yet
- ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic Ketoacidosis and The Hyperglycemic Hyperosmolar StateDocument23 pagesISPAD Clinical Practice Consensus Guidelines 2018: Diabetic Ketoacidosis and The Hyperglycemic Hyperosmolar StateJulietPérezNo ratings yet
- Is Fever A Red Flag For Bacterial Pneumonia in Children With Viral Bronchiolitis?Document4 pagesIs Fever A Red Flag For Bacterial Pneumonia in Children With Viral Bronchiolitis?Ximena ParedesNo ratings yet
- Love Me If You Dare - A Complex Romantic RelationshipDocument2 pagesLove Me If You Dare - A Complex Romantic RelationshipXimena ParedesNo ratings yet
- 2010-12 600 800 Rush Switchback RMK Service Manual PDFDocument430 pages2010-12 600 800 Rush Switchback RMK Service Manual PDFBrianCook73% (11)
- Membandingkan Recall 24 Jam Nutri Survey Dengan TkpiDocument7 pagesMembandingkan Recall 24 Jam Nutri Survey Dengan TkpiFransisca SihotangNo ratings yet
- OMR Sheet Has Been Attached at The End: EST Erial ODocument8 pagesOMR Sheet Has Been Attached at The End: EST Erial OSangeeta BansalNo ratings yet
- Continuous Sampling PlanDocument2 pagesContinuous Sampling PlanAnonymous wA6NGuyklDNo ratings yet
- InteliLite AMF20-25Document2 pagesInteliLite AMF20-25albertooliveira100% (2)
- Week 1 Gec 106Document16 pagesWeek 1 Gec 106Junjie FuentesNo ratings yet
- 1571-1635319494618-Unit 04 Leadership and ManagementDocument48 pages1571-1635319494618-Unit 04 Leadership and ManagementdevindiNo ratings yet
- Lineapelle: Leather & Non-LeatherDocument16 pagesLineapelle: Leather & Non-LeatherShikha BhartiNo ratings yet
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- FM 5130Document66 pagesFM 5130Aswini Kr KarmakarNo ratings yet
- Design ThinkingDocument16 pagesDesign ThinkingbhattanitanNo ratings yet
- XXCCCDocument17 pagesXXCCCwendra adi pradanaNo ratings yet
- WEEK 8. - Gen Math-PortfolioDocument12 pagesWEEK 8. - Gen Math-PortfolioOreo ProductionsNo ratings yet
- GRP Product CatalogueDocument57 pagesGRP Product CatalogueMulyana alcNo ratings yet
- Ringkasan LaguDocument4 pagesRingkasan LaguJoe PyNo ratings yet
- Starting A Business Candle Making 2009Document2 pagesStarting A Business Candle Making 2009Carlo Fabros Junio100% (4)
- Muv PDFDocument6 pagesMuv PDFDenisse PxndithxNo ratings yet
- Angelomorphic Christology and The Book of Revelation - Matthias Reinhard HoffmannDocument374 pagesAngelomorphic Christology and The Book of Revelation - Matthias Reinhard HoffmannEusebius325100% (2)
- Useful Relations in Quantum Field TheoryDocument30 pagesUseful Relations in Quantum Field TheoryDanielGutierrez100% (1)
- Eagle Test ReportDocument25 pagesEagle Test ReportMuhammad FahadNo ratings yet
- Astm D 664 - 07Document8 pagesAstm D 664 - 07Alfonso MartínezNo ratings yet
- Ahu, Chiller, Fcu Technical Bid TabulationDocument15 pagesAhu, Chiller, Fcu Technical Bid TabulationJohn Henry AsuncionNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Plastic Welding: We Know HowDocument125 pagesPlastic Welding: We Know Howprabal rayNo ratings yet
- Chirag STDocument18 pagesChirag STchiragNo ratings yet
- SS1c MIDTERMS LearningModuleDocument82 pagesSS1c MIDTERMS LearningModuleBryce VentenillaNo ratings yet
- Telecommunications TechnicianDocument4 pagesTelecommunications Technicianapi-78381064No ratings yet
- SCJP 1.6 Mock Exam Questions (60 QuestionsDocument32 pagesSCJP 1.6 Mock Exam Questions (60 QuestionsManas GhoshNo ratings yet
- Environmental Threats Differentiated Reading Comprehension Ver 1Document20 pagesEnvironmental Threats Differentiated Reading Comprehension Ver 1Camila DiasNo ratings yet
- Project Report Software and Web Development Company: WWW - Dparksolutions.inDocument12 pagesProject Report Software and Web Development Company: WWW - Dparksolutions.inRavi Kiran Rajbhure100% (1)