You might also like
- Lab Results and Drug Study - Feu NRMF (Head Nursing)Document8 pagesLab Results and Drug Study - Feu NRMF (Head Nursing)Hayzel Rivera RemotoNo ratings yet
- Flagging XT Series: Product Specialist PT. Saba IndomedikaDocument58 pagesFlagging XT Series: Product Specialist PT. Saba IndomedikaDiah Puspita RiniNo ratings yet
- FlaggingDocument65 pagesFlaggingTony KurniawanNo ratings yet
- Theoretical Foundations in Nursing: Learning OutcomesDocument32 pagesTheoretical Foundations in Nursing: Learning OutcomesCarlyne LaneteNo ratings yet
- A Manual For Buddhism and Deep EcologyDocument171 pagesA Manual For Buddhism and Deep EcologyajksuskdjNo ratings yet
- Covid Report-Self AnalysisDocument2 pagesCovid Report-Self AnalysisMuhammad Masood HaiderNo ratings yet
- Laboratory FindingsDocument51 pagesLaboratory FindingsALYSSA PACHECONo ratings yet
- Diagnostic Test W/ Normal Values Result Interpretat ION Significance Nursing Responsibility RE MA RKSDocument2 pagesDiagnostic Test W/ Normal Values Result Interpretat ION Significance Nursing Responsibility RE MA RKSjanna mae patriarcaNo ratings yet
- LABS Part 2Document3 pagesLABS Part 2Jordz PlaciNo ratings yet
- Acep Evidencecare Covid19severitytoolDocument3 pagesAcep Evidencecare Covid19severitytoolShariq IqbalNo ratings yet
- Board CECDocument3 pagesBoard CECCarlos DNo ratings yet
- Instrument Introduction: Automatic Hematology Analyzer Seeing Beyond LimitDocument2 pagesInstrument Introduction: Automatic Hematology Analyzer Seeing Beyond LimitCarla YcoNo ratings yet
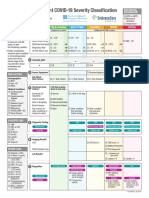
- Emergency Department COVID-19 Severity ClassificationDocument3 pagesEmergency Department COVID-19 Severity ClassificationAsti YumnaNo ratings yet
- LABS Part 2 Jagna SchistosomiasisDocument3 pagesLABS Part 2 Jagna SchistosomiasisJordz PlaciNo ratings yet
- LabsDocument3 pagesLabsJan DamesNo ratings yet
- Laboratory TestDocument3 pagesLaboratory TestKim TangoNo ratings yet
- BONAVERA COUNT 5R BroucherDocument4 pagesBONAVERA COUNT 5R BroucherAnurag VermaNo ratings yet
- Group F DXDocument2 pagesGroup F DXmyer pasandalanNo ratings yet
- Reagent Definition T BIL: Document Number: 841076 - 13 - Applic - T BIL, Date: 10/09, S.W. 7.2Document2 pagesReagent Definition T BIL: Document Number: 841076 - 13 - Applic - T BIL, Date: 10/09, S.W. 7.2Sud007jbNo ratings yet
- Validatie Document Omron EVOLVDocument4 pagesValidatie Document Omron EVOLVKokou GbeganNo ratings yet
- DiagnosticDocument2 pagesDiagnosticakroma092No ratings yet
- Reagent Definition D BIL: Document Number: 841096 - 13 - Applic - D BIL, Date: 10/09, S.W. 7.2Document2 pagesReagent Definition D BIL: Document Number: 841096 - 13 - Applic - D BIL, Date: 10/09, S.W. 7.2Sud007jbNo ratings yet
- Labs of Common Medical ConditionsDocument3 pagesLabs of Common Medical Conditionszezma GamingNo ratings yet
- Reagent Definition CREA Jaffe: Document Number: D00758 - 11 - Applic - CREA Jaffe, Date: 10/09, S.W. 7.2Document2 pagesReagent Definition CREA Jaffe: Document Number: D00758 - 11 - Applic - CREA Jaffe, Date: 10/09, S.W. 7.2Sud007jbNo ratings yet
- ProBrochure PDFDocument2 pagesProBrochure PDFCarlos José DiazNo ratings yet
- Normal RangesDocument1 pageNormal RangesLayalNo ratings yet
- Normal ValuesDocument8 pagesNormal ValuesJOHN CARLO APATANNo ratings yet
- LABORATORY EXAM WPS OfficeDocument5 pagesLABORATORY EXAM WPS OfficeLoveline Kate AlcedoNo ratings yet
- Laboratory and Diagnostic ProceduresDocument2 pagesLaboratory and Diagnostic ProceduresDomato Ayaon NawalNo ratings yet
- ESH-IP 2010 Validation of Omron M3W (HEM-7202-E)Document4 pagesESH-IP 2010 Validation of Omron M3W (HEM-7202-E)Pub PleNo ratings yet
- Co Memory Ate (March 2022)Document5 pagesCo Memory Ate (March 2022)Maria Renee Lian NobleNo ratings yet
- Labs Finals Case PreDocument4 pagesLabs Finals Case Prereized02No ratings yet
- Hemolytic Disease of The NewbornDocument47 pagesHemolytic Disease of The NewbornJanine CabreraNo ratings yet
- Lab ProceduresDocument7 pagesLab Procedureslaurie.charlynjaneNo ratings yet
- Dايناس على باب اللوق2Document1 pageDايناس على باب اللوق2shoshoeng359No ratings yet
- Laboratory FindingsDocument1 pageLaboratory FindingsJade ParkNo ratings yet
- HDL Direct-Erba XL 600Document1 pageHDL Direct-Erba XL 600sangNo ratings yet
- Applic ASODocument2 pagesApplic ASOBianca HardutNo ratings yet
- Laboratory Study: Complete Blood CountDocument5 pagesLaboratory Study: Complete Blood CountNicole Angeli ManuelNo ratings yet
- Management of Patients With Nonmalignant Hematologic DisordersDocument97 pagesManagement of Patients With Nonmalignant Hematologic DisordersJulia Rae Delos SantosNo ratings yet
- DF5020 231123 104954Document2 pagesDF5020 231123 104954Osama Ben DawNo ratings yet
- Thrombus Burden: Case Processing SummaryDocument7 pagesThrombus Burden: Case Processing SummaryAldianMLokariaNo ratings yet
- Reagent Definition UREA: Document Number: D00548 - 09 - Applic - UREA, Date: 10/09, S.W. 7.2Document2 pagesReagent Definition UREA: Document Number: D00548 - 09 - Applic - UREA, Date: 10/09, S.W. 7.2Sud007jbNo ratings yet
- Mcfarland DensitometerDocument3 pagesMcfarland DensitometerAkbar SaleemNo ratings yet
- Nama: Dita Desinta Amalia NIM: 33178K19031 Semester: 4B Tugas BiostatistikDocument9 pagesNama: Dita Desinta Amalia NIM: 33178K19031 Semester: 4B Tugas BiostatistikSyifa ZahraNo ratings yet
- Lab PediaDocument10 pagesLab PediaInosanto May AnnNo ratings yet
- Digital Wattmeter Varmeter With Builtin Transducer 6Document2 pagesDigital Wattmeter Varmeter With Builtin Transducer 6Gopichand GaddamNo ratings yet
- ESH-IP 2010 Validation of Nissei DSK-1031Document3 pagesESH-IP 2010 Validation of Nissei DSK-1031Pub PleNo ratings yet
- 1.parasuicide and DVT Ward Round Presentation FinalDocument16 pages1.parasuicide and DVT Ward Round Presentation Finalavile ngqolosiNo ratings yet
- Red Cells & Whole Blood DosageDocument4 pagesRed Cells & Whole Blood DosageVictor ChanNo ratings yet
- The Role of Antithrombin III in Neonatal Sepsis - Novie AmeliaDocument26 pagesThe Role of Antithrombin III in Neonatal Sepsis - Novie AmeliaBayu KurniawanNo ratings yet
- Revil Lab Fem WardDocument2 pagesRevil Lab Fem WardJohn Emmanuel RevilNo ratings yet
- Labs of Common Medical ConditionsDocument2 pagesLabs of Common Medical Conditionszezma GamingNo ratings yet
- IFU - BM6010 e UIBC 1Document2 pagesIFU - BM6010 e UIBC 1Imas NurhayatiNo ratings yet
- This Worksheet Plots Two-Way Linear Interaction Effects Estimated Via Regression AnalysisDocument5 pagesThis Worksheet Plots Two-Way Linear Interaction Effects Estimated Via Regression AnalysisRhouenNo ratings yet
- Echo Report : (Abridged)Document4 pagesEcho Report : (Abridged)Ajay KarolNo ratings yet
- Case Study LaboratoryDocument4 pagesCase Study LaboratoryKJay SolijonNo ratings yet
- Algoritm Disfunctie DiastolicaDocument1 pageAlgoritm Disfunctie DiastolicaNeacsu OvidiuNo ratings yet
- BCC3000 Service Manual New)Document54 pagesBCC3000 Service Manual New)mustakim gma100% (1)
- Zoghbi ASE Guidelines MR AR FINAL - Updated - 0Document34 pagesZoghbi ASE Guidelines MR AR FINAL - Updated - 0DenisseRangelNo ratings yet
- 3M Protocol Rc222Document1 page3M Protocol Rc222Rommel SacramentoNo ratings yet
- Cerebrospinal Fluid: Learning ObjectivesDocument18 pagesCerebrospinal Fluid: Learning ObjectivesJonalyn LumantasNo ratings yet
- Current Scenario On Application of Computational Tools in Biological SystemsDocument12 pagesCurrent Scenario On Application of Computational Tools in Biological SystemsAnkit AgrawalNo ratings yet
- 01st Semester Fall General Schedule 2023 2024 Academic Year Groups Individual Study Plans Class of 2029Document44 pages01st Semester Fall General Schedule 2023 2024 Academic Year Groups Individual Study Plans Class of 2029nikkrixoNo ratings yet
- 12.4.3: Evolution Fill in The Blank WithDocument3 pages12.4.3: Evolution Fill in The Blank Withapi-25965241No ratings yet
- Introductory Immunology - Basic Concepts For Interdisciplinary Applications, 3e (Feb 6, 2023) - (0443153086) - (Academic Press) 3rd Edition ActorDocument43 pagesIntroductory Immunology - Basic Concepts For Interdisciplinary Applications, 3e (Feb 6, 2023) - (0443153086) - (Academic Press) 3rd Edition Actorwilliam.vickers704100% (6)
- Sunlight & CancerDocument13 pagesSunlight & CancerMarcoSaliniNo ratings yet
- PreviewpdfDocument111 pagesPreviewpdfnadela noviaNo ratings yet
- Ekg Plain and Simple 4th Edition Ellis Test BankDocument35 pagesEkg Plain and Simple 4th Edition Ellis Test Banknicoledickersonwmncpoyefk100% (20)
- Solution PreparationDocument2 pagesSolution PreparationFauzi Akhbar AnugrahNo ratings yet
- Biotechnology Principles and ProcessesDocument12 pagesBiotechnology Principles and ProcessesPartha SheeNo ratings yet
- Annual Report 2011 2012Document132 pagesAnnual Report 2011 2012Colly PoenyaNo ratings yet
- Biogeografia Spain PDFDocument82 pagesBiogeografia Spain PDFMarcos Noos EspíanNo ratings yet
- 8.1. Reading - Social Networking - Ex22.QT12 - VOCABULARYDocument3 pages8.1. Reading - Social Networking - Ex22.QT12 - VOCABULARYDiệu Anh HoàngNo ratings yet
- 100 Years of Child & Parenting Development Theories: From Freud To BrazeltonDocument28 pages100 Years of Child & Parenting Development Theories: From Freud To BrazeltonGeoffrey Tolentino-Unida100% (1)
- Gram StainingDocument9 pagesGram StainingGayatri PandaNo ratings yet
- Alcohol - WikipediaDocument14 pagesAlcohol - WikipediaMorteza YazdaniNo ratings yet
- New Plant Breeding Techniques. State-Of-The-Art and Prospects For Commercial DevelopmentDocument220 pagesNew Plant Breeding Techniques. State-Of-The-Art and Prospects For Commercial DevelopmentJulian Andres Tovar MedinaNo ratings yet
- Vpat 101:: Veterinary General PathologyDocument4 pagesVpat 101:: Veterinary General PathologyHarleanne ParkNo ratings yet
- Growth and Culturing of BacteriaDocument103 pagesGrowth and Culturing of BacteriaAbd ahmadNo ratings yet
- 12 Bio CH 24 MCQsDocument19 pages12 Bio CH 24 MCQsAhmad NawazNo ratings yet
- MCC - CH 1 AnswersDocument5 pagesMCC - CH 1 Answersaileen-brito-6525No ratings yet
- Lesson 3.2: Human Major Body Organs (Grade 4)Document8 pagesLesson 3.2: Human Major Body Organs (Grade 4)Rica Jean IbcasNo ratings yet
- Etymology: PantheraDocument4 pagesEtymology: PantheraMaximos ManiatisNo ratings yet
- ZEN SoftwareDocument28 pagesZEN SoftwarePc FastNo ratings yet
- Section 1 Nature and Variety of Living OrganismDocument23 pagesSection 1 Nature and Variety of Living OrganismelikaNo ratings yet
- Implications To PracticeDocument483 pagesImplications To PracticeBernard CarpioNo ratings yet
- ReagentsDocument12 pagesReagentsKimscey Yvan DZ SulitNo ratings yet