You might also like
- The Effect of DBT On AutismDocument11 pagesThe Effect of DBT On AutismJinny DavisNo ratings yet
- Cognitive Behavioral Treatment For Depressed AdolescentsDocument17 pagesCognitive Behavioral Treatment For Depressed Adolescentscharoline gracetiani nataliaNo ratings yet
- Problem Solving Therapy in the Clinical PracticeFrom EverandProblem Solving Therapy in the Clinical PracticeRating: 5 out of 5 stars5/5 (1)
- Head NurseDocument3 pagesHead NurseLiza Noble-RoaNo ratings yet
- Hospital Acquired InfectionsDocument51 pagesHospital Acquired Infectionstummalapalli venkateswara raoNo ratings yet
- School Health ServiceDocument43 pagesSchool Health ServiceAnitha Thankappan100% (1)
- Case Study of Placenta PreviaDocument24 pagesCase Study of Placenta Previajeelani saima86% (36)
- Subject: Health Grade: 4 UNIT 3: Substance Use and Abuse LESSON 3: Using Medicine Properly ObjectivesDocument4 pagesSubject: Health Grade: 4 UNIT 3: Substance Use and Abuse LESSON 3: Using Medicine Properly ObjectivesJerome Eziekel Posada PanaliganNo ratings yet
- The Effectiveness of 6 Versus 12-Months of DBTDocument16 pagesThe Effectiveness of 6 Versus 12-Months of DBTPechopalomo 90No ratings yet
- Self-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaDocument13 pagesSelf-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaArif IrpanNo ratings yet
- EstigmaDocument8 pagesEstigmaAna Carolina RibasNo ratings yet
- DRT2012-460419Document11 pagesDRT2012-460419Sapto SutardiNo ratings yet
- Development and Psychometric Properties The Barriers To Access To Care Evaluation Scale (BACE) Related To People With Mental Ill HealthDocument11 pagesDevelopment and Psychometric Properties The Barriers To Access To Care Evaluation Scale (BACE) Related To People With Mental Ill HealthReem AlkaabiNo ratings yet
- Brightside BMC ArticleDocument10 pagesBrightside BMC ArticlePsydocNo ratings yet
- The Feasibility of Mindfulness-Based Cognitive Therapy For People With Bipolar Disorder: A Qualitative StudyDocument12 pagesThe Feasibility of Mindfulness-Based Cognitive Therapy For People With Bipolar Disorder: A Qualitative StudyTehseenah ZaraNo ratings yet
- s12888 019 2412 0Document12 pagess12888 019 2412 0Estrella Esperanza Montoya PantojaNo ratings yet
- Barriers to Treatment for Borderline Personality DisorderDocument15 pagesBarriers to Treatment for Borderline Personality Disordereuropython100% (1)
- Nediskriminacija - RadDocument11 pagesNediskriminacija - RadivanNo ratings yet
- Structural Stigma and Its Impact On Healthcare For Borderline Personality Disorder: A Scoping ReviewDocument41 pagesStructural Stigma and Its Impact On Healthcare For Borderline Personality Disorder: A Scoping Reviewconsulta.nicolaslabbeNo ratings yet
- Clinical Guidelines For The Management of DepressiDocument10 pagesClinical Guidelines For The Management of Depressiverdeoros uaemexNo ratings yet
- Effectiveness of single-session therapy for adult common mental disorders a systematic reviewDocument15 pagesEffectiveness of single-session therapy for adult common mental disorders a systematic reviewVitor GuidaNo ratings yet
- Study Protocol of A Multicenter Randomized Controlled Trial of Mindfulness-Based Cognitive Therapy and Treatment As Usual in Bipolar DisorderDocument10 pagesStudy Protocol of A Multicenter Randomized Controlled Trial of Mindfulness-Based Cognitive Therapy and Treatment As Usual in Bipolar Disorderzuhrul_baladNo ratings yet
- Patient Perspectives On Non-Response To Psychotherapy For Borderline Personality Disorder: A Qualitative StudyDocument15 pagesPatient Perspectives On Non-Response To Psychotherapy For Borderline Personality Disorder: A Qualitative StudyAndrea Carolina Avalos QuizhpiNo ratings yet
- Representations of Personalised Medicine in Family HealthDocument9 pagesRepresentations of Personalised Medicine in Family HealthAbCcNo ratings yet
- Barriers To Care For Adolescents With Borderline Personality DisorderDocument7 pagesBarriers To Care For Adolescents With Borderline Personality DisorderMaria Jesus ZaldivarNo ratings yet
- Bipolar I Disorder I. A Qualitative Study of The Viewpoints of Family MembersDocument12 pagesBipolar I Disorder I. A Qualitative Study of The Viewpoints of Family MembersPsichologijos StudentaiNo ratings yet
- Content ServerDocument11 pagesContent ServerALONDRA FERNANDA RODRIGUEZ HERRERANo ratings yet
- A Case Series of 223 Patients With Depersonalization-Derealization SyndromeDocument11 pagesA Case Series of 223 Patients With Depersonalization-Derealization SyndromeRavennaNo ratings yet
- Recent Advances in Understanding and Managing BodyDocument6 pagesRecent Advances in Understanding and Managing BodyFábio LopesNo ratings yet
- Guided Self-Help For Anxiety ADocument13 pagesGuided Self-Help For Anxiety Amonaliza jessieNo ratings yet
- Management of Behavioral and Psychological Symptoms of DementiaDocument11 pagesManagement of Behavioral and Psychological Symptoms of DementiaCindy GautamaNo ratings yet
- Diagnosis and Management of ADHDDocument12 pagesDiagnosis and Management of ADHDAdinda Ratna PuspitaNo ratings yet
- Burnout Syndrome in Healthcare Professionals Who Care For Patients With Prolonged Disorders of Consciousness: A Cross-Sectional SurveyDocument10 pagesBurnout Syndrome in Healthcare Professionals Who Care For Patients With Prolonged Disorders of Consciousness: A Cross-Sectional SurveyPuujee12 11No ratings yet
- Da3623 Appendix 1. Beds Luton BPDDocument24 pagesDa3623 Appendix 1. Beds Luton BPDNada KhanNo ratings yet
- effectiveness-of-acceptance-and-commitment-therapy-in-improving-interpersonal-problems-quality-of-7508Document7 pageseffectiveness-of-acceptance-and-commitment-therapy-in-improving-interpersonal-problems-quality-of-7508tati rodriguesNo ratings yet
- Empowerment and Serius Mental Illness-02Document12 pagesEmpowerment and Serius Mental Illness-02pepe pinitoNo ratings yet
- Palliative Care For People With Schizophrenia: A Qualitative Study of An Under-Serviced Group in NeedDocument11 pagesPalliative Care For People With Schizophrenia: A Qualitative Study of An Under-Serviced Group in Needadri90No ratings yet
- Betts2018 Article APsychoeducationalGroupInterveDocument7 pagesBetts2018 Article APsychoeducationalGroupInterveCralosNo ratings yet
- Psychiatry's Role in The Prevention of Post-Intensive Care Mental Health Impairment: Stakeholder SurveyDocument9 pagesPsychiatry's Role in The Prevention of Post-Intensive Care Mental Health Impairment: Stakeholder SurveyJosue GarciaNo ratings yet
- Antoniades2014 Article EfficacyOfDepressionTreatmentsDocument12 pagesAntoniades2014 Article EfficacyOfDepressionTreatmentsdidi monroeNo ratings yet
- Jurnal 5Document14 pagesJurnal 5Ika Agitra NingrumNo ratings yet
- Journal of Psychosomatic Research: M.C. Shedden-Mora, B. Groß, K. Lau, A. Gumz, K. Wegscheider, B. LöweDocument8 pagesJournal of Psychosomatic Research: M.C. Shedden-Mora, B. Groß, K. Lau, A. Gumz, K. Wegscheider, B. LöweSeva RenandoNo ratings yet
- Effectiveness of A Psychoeducation Group Intervention Conducted by Primary Healthcare Nurses in Patients With Depression and Physical Comorbidity: Study Protocol For A Randomized, Controlled TrialDocument9 pagesEffectiveness of A Psychoeducation Group Intervention Conducted by Primary Healthcare Nurses in Patients With Depression and Physical Comorbidity: Study Protocol For A Randomized, Controlled TrialCarmena CuNo ratings yet
- A Psychoeducational Group Intervention For FamilyDocument8 pagesA Psychoeducational Group Intervention For FamilyIoannis MalogiannisNo ratings yet
- Information Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewDocument18 pagesInformation Needs and Sources of Information Among People With Depression and Anxiety: A Scoping ReviewVince MartinezNo ratings yet
- Psychological interventions for bipolar disorderDocument9 pagesPsychological interventions for bipolar disorderFausiah Ulva MNo ratings yet
- A Health Promoting-Lifestyle Prediction Model For Dementia Prevention Among Chinese Adults: Based On The Health Belief ModelDocument11 pagesA Health Promoting-Lifestyle Prediction Model For Dementia Prevention Among Chinese Adults: Based On The Health Belief ModelFrans LandiNo ratings yet
- Changes in Attitudes Toward Mental Illness in Healthcare Professionals and StudentsDocument14 pagesChanges in Attitudes Toward Mental Illness in Healthcare Professionals and StudentsleticiaNo ratings yet
- Fmed 09 1024022Document12 pagesFmed 09 1024022Nicolás Mosso F.No ratings yet
- Benefits and Drawbacks of Medical Model of Mental IllnessDocument19 pagesBenefits and Drawbacks of Medical Model of Mental IllnessNazish JavedNo ratings yet
- Chibanda 2016Document9 pagesChibanda 2016Lhawal YemmyNo ratings yet
- Experiences of Psychotherapists Working With RefugeesDocument8 pagesExperiences of Psychotherapists Working With RefugeesYang GuoNo ratings yet
- Prevention of Depresssion in Childhood and AdolescenceDocument18 pagesPrevention of Depresssion in Childhood and AdolescenceNatalia VielmaNo ratings yet
- Psychosocial Interventions For Patients With Chronic DiseaseDocument6 pagesPsychosocial Interventions For Patients With Chronic DiseaseRonel DayoNo ratings yet
- COSTE-EFICIENCIA Effectiveness and Cost-Effectiveness ofDocument9 pagesCOSTE-EFICIENCIA Effectiveness and Cost-Effectiveness ofLauraNo ratings yet
- s40479 023 00233 0Document9 pagess40479 023 00233 0nurazizahsn11No ratings yet
- Advances in Integrative Mental Health ApproachesDocument2 pagesAdvances in Integrative Mental Health ApproachesVictor Raul JuramaNo ratings yet
- Bipolar DisordersDocument9 pagesBipolar DisordersSabiha PazaracNo ratings yet
- Molino Et Al 2022 Transitioning From in Person To Telehealth Cognitive Behavioral Therapy For Social Anxiety DisorderDocument18 pagesMolino Et Al 2022 Transitioning From in Person To Telehealth Cognitive Behavioral Therapy For Social Anxiety DisorderIqbal BurhaniNo ratings yet
- 2016 Article 43Document8 pages2016 Article 43André LuizNo ratings yet
- The MomentumDocument12 pagesThe MomentumOlivia NasarreNo ratings yet
- FINAL Assessment 4Document11 pagesFINAL Assessment 4Ituuza KosiaNo ratings yet
- 000 SLR Existing Conceptualisation in AdolescentDocument14 pages000 SLR Existing Conceptualisation in AdolescentKumala WindyaNo ratings yet
- Teori SpssDocument13 pagesTeori SpsssitarrrrrrrrrrrrrrrrrrrNo ratings yet
- Integrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionFrom EverandIntegrative Medicine for Vulnerable Populations: A Clinical Guide to Working with Chronic and Comorbid Medical Disease, Mental Illness, and AddictionNo ratings yet
- Major MineralsDocument31 pagesMajor MineralsmissirenaNo ratings yet
- Vitamins: Nutrition Departement Faculty of Medicine - North Sumatera UniversityDocument54 pagesVitamins: Nutrition Departement Faculty of Medicine - North Sumatera UniversityMuhammad FaizNo ratings yet
- Asma UISU Medan 2017Document41 pagesAsma UISU Medan 2017DhimasAjiZuandaNo ratings yet
- Paranoid Types of Schizophrenia: (Laporan Kasus)Document7 pagesParanoid Types of Schizophrenia: (Laporan Kasus)Khaidir OrochimaruNo ratings yet
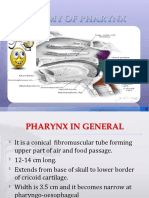
- Anatomy - of Nose, PharyngDocument24 pagesAnatomy - of Nose, PharyngrubyniNo ratings yet
- Diagnostic Laboratoric To Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked. Clin - Path. SPPKDocument41 pagesDiagnostic Laboratoric To Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked. Clin - Path. SPPKrubyniNo ratings yet
- Bronchiolitis Diagnosis and ManagementDocument25 pagesBronchiolitis Diagnosis and ManagementrubyniNo ratings yet
- k12, Pa, Pathology of Copd - rts1-k12Document46 pagesk12, Pa, Pathology of Copd - rts1-k12ashtridNo ratings yet
- Deep Vein Thrombosis Diagnostic and ManagementDocument20 pagesDeep Vein Thrombosis Diagnostic and ManagementrubyniNo ratings yet
- Congenital Malformation of The Lung and AirwaysDocument48 pagesCongenital Malformation of The Lung and AirwaysrubyniNo ratings yet
- K 30 (C) - Perdarahan, Henochslein PurpuraDocument18 pagesK 30 (C) - Perdarahan, Henochslein PurpurarubyniNo ratings yet
- K 30a - Perdarahan, ITP-3Document20 pagesK 30a - Perdarahan, ITP-3rubyniNo ratings yet
- Haematopoitik System: Prof - Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked - SPPKDocument43 pagesHaematopoitik System: Prof - Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked - SPPKrubyniNo ratings yet
- Diagnostic Laboratoric To Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked. Clin - Path. SPPKDocument41 pagesDiagnostic Laboratoric To Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked. Clin - Path. SPPKrubyniNo ratings yet
- Hematopoeitic System: Alya Amila Fitrie Lokot Donna LubisDocument80 pagesHematopoeitic System: Alya Amila Fitrie Lokot Donna LubisrubyniNo ratings yet
- Clasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKDocument46 pagesClasification of Anemia: Prof. Dr. Adi Koesoema Aman SPPK (KH) Dr. Malayana Nasutioan Mked - SPPKrubyniNo ratings yet
- Anemia: Clinical Approach and Management: Dairion Gatot, Savita Handayani, Heny Syahrini, Andri MardiaDocument22 pagesAnemia: Clinical Approach and Management: Dairion Gatot, Savita Handayani, Heny Syahrini, Andri MardiarubyniNo ratings yet
- Deep Vein Thrombosis Diagnostic and ManagementDocument20 pagesDeep Vein Thrombosis Diagnostic and ManagementrubyniNo ratings yet
- K 30 (C) - Perdarahan, Henochslein PurpuraDocument18 pagesK 30 (C) - Perdarahan, Henochslein PurpurarubyniNo ratings yet
- APLASTIC ANEMIA CRITERIA AND TREATMENT OPTIONSDocument11 pagesAPLASTIC ANEMIA CRITERIA AND TREATMENT OPTIONSrubyniNo ratings yet
- CHM 1002 Chemstry B CHAPTER 3: Physical Chemistry - Chemical EquilibriumDocument33 pagesCHM 1002 Chemstry B CHAPTER 3: Physical Chemistry - Chemical EquilibriumrubyniNo ratings yet
- Thesis PosterDocument1 pageThesis Posterapi-418424753No ratings yet
- The Benefits and Challenges of E-Health Applications in Developing Nations: A ReviewDocument10 pagesThe Benefits and Challenges of E-Health Applications in Developing Nations: A ReviewbennyNo ratings yet
- Monitoring Proses, Jaka, HISSI JatimDocument22 pagesMonitoring Proses, Jaka, HISSI JatimRINA FEBRIYANTINo ratings yet
- Knowledge, Attitude, Awareness and Perception of Dental Implants Among Undergraduate Dental StudentsDocument4 pagesKnowledge, Attitude, Awareness and Perception of Dental Implants Among Undergraduate Dental StudentsInternational Journal of Innovative Science and Research Technology0% (1)
- Head Nursing: University of Cebu - BaniladDocument30 pagesHead Nursing: University of Cebu - BaniladVjay DingNo ratings yet
- Articol ,,pain Medicine'' - Pain Management A Fundamental Human Right Frank BrennanDocument17 pagesArticol ,,pain Medicine'' - Pain Management A Fundamental Human Right Frank BrennanAnonymous KgUtPlkjNo ratings yet
- AdhdDocument5 pagesAdhdAndreea VanăNo ratings yet
- SF424R-R Biosketchsample VerCDocument5 pagesSF424R-R Biosketchsample VerCPeter ShenNo ratings yet
- Breaking Bad NewsDocument26 pagesBreaking Bad News8625g8xmbpNo ratings yet
- Brought To You by Sam Agency: To Join Us Click Here Facebook or TelegramDocument4 pagesBrought To You by Sam Agency: To Join Us Click Here Facebook or TelegramJoan Manabat BugnaNo ratings yet
- WASH Actionplan 22Document4 pagesWASH Actionplan 22marielNo ratings yet
- MSM Degree Plan and CoursesDocument8 pagesMSM Degree Plan and Coursesmaverick auburnNo ratings yet
- AGP Procedures and PPE GuidanceDocument4 pagesAGP Procedures and PPE GuidanceAhmed Ben BellaNo ratings yet
- INICET Jul 23 1st Round-Website CompressedDocument486 pagesINICET Jul 23 1st Round-Website CompressedSTEP TO MEDICOSNo ratings yet
- Latest Resume BuelaDocument3 pagesLatest Resume BuelaCleeve Humprey BuelaNo ratings yet
- Clinical Practice GuidelinesDocument1 pageClinical Practice GuidelinesGrace MellaineNo ratings yet
- Day in the ERDocument2 pagesDay in the ERGenevieve MundalaNo ratings yet
- Pediatrics Overview: Development, Socio-cultural Issues, Environment and Community RoleDocument3 pagesPediatrics Overview: Development, Socio-cultural Issues, Environment and Community RoledadaNo ratings yet
- Communication Skills: DR Bob KlajoDocument10 pagesCommunication Skills: DR Bob KlajoBob JohnNo ratings yet
- DentalUM Fall 2012Document40 pagesDentalUM Fall 2012umdentNo ratings yet
- Shayla 2020 ResumeDocument3 pagesShayla 2020 Resumeapi-519400915No ratings yet
- Bioavailability & Bioequivalence Pharmacokinetic PrinciplesDocument24 pagesBioavailability & Bioequivalence Pharmacokinetic PrinciplesKoya AnushareddyNo ratings yet
- Pelaksanaan Sistem Informasi Kesehatan Daerah (SIKDA) Generik Di Unit Rekam Medis Puskesmas Siak Hulu Tahun 2020 Muhammad Dedi Widodo, Reno RenaldiDocument6 pagesPelaksanaan Sistem Informasi Kesehatan Daerah (SIKDA) Generik Di Unit Rekam Medis Puskesmas Siak Hulu Tahun 2020 Muhammad Dedi Widodo, Reno RenaldiRiri LangoyNo ratings yet
- ANM001 MeritList 11-2019Document69 pagesANM001 MeritList 11-2019manojsingh474No ratings yet
- Borderline Manual Ol enDocument72 pagesBorderline Manual Ol enbasakerpolatNo ratings yet