You might also like
- BITSEA Brief Guide For Professionals: What Is The BITSEA?Document4 pagesBITSEA Brief Guide For Professionals: What Is The BITSEA?Mihaela GrigoroiuNo ratings yet
- Basic Incident Command System Course: Activity Packet For TraineesDocument12 pagesBasic Incident Command System Course: Activity Packet For TraineesPELIGRO RAMIENo ratings yet
- (Brandao de Carvalho, Joaquim) Lenition and FortitionDocument607 pages(Brandao de Carvalho, Joaquim) Lenition and FortitionLevente JambrikNo ratings yet
- Current Issues in Nursing EducationDocument12 pagesCurrent Issues in Nursing EducationMhel Es QuiadNo ratings yet
- Factors Influencing The Health Seeking Behaviors of Wo - 2021 - International JoDocument9 pagesFactors Influencing The Health Seeking Behaviors of Wo - 2021 - International JoRonald QuezadaNo ratings yet
- Preventive Medicine: Shristi Bhochhibhoya, Page D. Dobbs, Sarah B. ManessDocument9 pagesPreventive Medicine: Shristi Bhochhibhoya, Page D. Dobbs, Sarah B. ManessRolando NavarroNo ratings yet
- Falope RM Chapter 1 (18518)Document7 pagesFalope RM Chapter 1 (18518)falopetaiwo.12No ratings yet
- Advancing Genetic Nursing Knowledge 2004 Nursing OutlookDocument7 pagesAdvancing Genetic Nursing Knowledge 2004 Nursing OutlookSeeta NanooNo ratings yet
- Ca MamaeDocument7 pagesCa MamaeAnonymous vkq7UwNo ratings yet
- Foster2018 PDFDocument1 pageFoster2018 PDFFake_Me_No ratings yet
- The International Glossary On Infertility and Fertility Care, 2017Document14 pagesThe International Glossary On Infertility and Fertility Care, 2017Zurya UdayanaNo ratings yet
- 1 s2.0 S2414644721000877 MainDocument5 pages1 s2.0 S2414644721000877 MainSome LaNo ratings yet
- IDocument2 pagesIAllysa Megan OrpillaNo ratings yet
- Breast Cancer ReflectionDocument4 pagesBreast Cancer ReflectionCAJES NOLINo ratings yet
- Enc 1101 - Project 2 Research Proposal and Annotated Bibliography - Spring 2024Document5 pagesEnc 1101 - Project 2 Research Proposal and Annotated Bibliography - Spring 2024api-742553212No ratings yet
- Gakunga 2019Document8 pagesGakunga 2019FaidurrahmanNo ratings yet
- Breast Cancer Knowledge Among College Students Justice King Vidourek Merianos 2018Document10 pagesBreast Cancer Knowledge Among College Students Justice King Vidourek Merianos 2018Marc BantilanNo ratings yet
- Oncology Nurse Managers' Perceptions of Palliative Care and End-of-Life CommunicationDocument13 pagesOncology Nurse Managers' Perceptions of Palliative Care and End-of-Life CommunicationRatih puspita DewiNo ratings yet
- Breast ThesisDocument4 pagesBreast Thesisafjrpomoe100% (2)
- Breast Cancer Awareness Among Health ProfessionalsDocument3 pagesBreast Cancer Awareness Among Health ProfessionalsWac GunarathnaNo ratings yet
- Obesity and Breast Reconstruction: Complications and Patient-Reported Outcomes in A Multicenter, Prospective StudyDocument10 pagesObesity and Breast Reconstruction: Complications and Patient-Reported Outcomes in A Multicenter, Prospective StudyMehmet SürmeliNo ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- Patient Education and Counseling: Joelle I. Rosser, Betty Njoroge, Megan J. HuchkoDocument6 pagesPatient Education and Counseling: Joelle I. Rosser, Betty Njoroge, Megan J. HuchkoTrysna Ayu SukardiNo ratings yet
- Research ReportDocument13 pagesResearch Reportapi-662910690No ratings yet
- FTP PDFDocument5 pagesFTP PDFRismayantiNo ratings yet
- EJ1078866Document12 pagesEJ1078866valentinasecivirNo ratings yet
- Clinical Oncology: World Journal ofDocument13 pagesClinical Oncology: World Journal ofMATEJ MAMICNo ratings yet
- Oalibj 2020102215471650Document19 pagesOalibj 2020102215471650Balali GadafiNo ratings yet
- Use of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitDocument18 pagesUse of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitHanisha EricaNo ratings yet
- Nursing CourseDocument8 pagesNursing Coursepatel ravirajNo ratings yet
- Literature Review Breast Self Examination ResearchDocument7 pagesLiterature Review Breast Self Examination ResearchaflsigakfNo ratings yet
- POSITIVEDocument12 pagesPOSITIVEtabaresgonzaloNo ratings yet
- Maternity MainDocument13 pagesMaternity Mainbayu purnomoNo ratings yet
- Family Support and Self-Esteem of Patient With Breast CancerDocument5 pagesFamily Support and Self-Esteem of Patient With Breast CancerDean Rex Azriel TelaumbanuaNo ratings yet
- Cut Off2Document15 pagesCut Off2Odiyana Prayoga GriadhiNo ratings yet
- Information Needs of Women With Breast Cancer: A Review of The LiteratureDocument16 pagesInformation Needs of Women With Breast Cancer: A Review of The LiteratureHina SardarNo ratings yet
- The Role of Nursing in Cervical Cancer Prevention and TreatmentDocument5 pagesThe Role of Nursing in Cervical Cancer Prevention and TreatmentLytiana WilliamsNo ratings yet
- 1 PDFDocument7 pages1 PDFSarah AryaNo ratings yet
- A Study To Assess The Knowledge Regarding Cervical Cancer Among Women in Selected Community Setting, ChennaiDocument3 pagesA Study To Assess The Knowledge Regarding Cervical Cancer Among Women in Selected Community Setting, ChennaiEditor IJTSRDNo ratings yet
- Decision Aids On Breast ConserDocument15 pagesDecision Aids On Breast Consersatria divaNo ratings yet
- Journal Pone 0253373Document17 pagesJournal Pone 0253373ElormNo ratings yet
- The Role and Contribution of Psychology Inthe Navigation of Oncology PatientsDocument6 pagesThe Role and Contribution of Psychology Inthe Navigation of Oncology PatientsSabrina JonesNo ratings yet
- BreastfeedDocument5 pagesBreastfeedBetHsy Pascua100% (1)
- A Protocol For A Cluster Randomized Controlled Trial of A Self Help Psycho Education Programme To Reduce Diagnosis Delay in Women With Breast Cancer Symptoms in IndonesiaDocument8 pagesA Protocol For A Cluster Randomized Controlled Trial of A Self Help Psycho Education Programme To Reduce Diagnosis Delay in Women With Breast Cancer Symptoms in Indonesiaflorentina dianNo ratings yet
- 503 837 1 PBDocument14 pages503 837 1 PB5m7m2c2kryNo ratings yet
- Rosen's Breast Pathology IntroductionDocument18 pagesRosen's Breast Pathology IntroductionyoussNo ratings yet
- Summary of Third Expert Report 2018Document116 pagesSummary of Third Expert Report 2018Diego12001No ratings yet
- Sobrevivientes Del Cancer GinecológicoDocument10 pagesSobrevivientes Del Cancer GinecológicoMIGUEL MORENONo ratings yet
- Knowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Women Visiting Primary Health Care Centres in BahrainDocument6 pagesKnowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Women Visiting Primary Health Care Centres in BahrainAnonymous N74eaOhdfkNo ratings yet
- Developing A Web-Based Shared Decision-Making Tool For Fertility Preservation Among Reproductive-Age Women With Breast CancerDocument10 pagesDeveloping A Web-Based Shared Decision-Making Tool For Fertility Preservation Among Reproductive-Age Women With Breast Cancer郭竹瑩No ratings yet
- Research Project 1Document9 pagesResearch Project 1Sangeeta SahaNo ratings yet
- Health Professionals ' Views On Maternity Care For Women With Physical Disabilities: A Qualitative StudyDocument11 pagesHealth Professionals ' Views On Maternity Care For Women With Physical Disabilities: A Qualitative StudyNabilaNo ratings yet
- Mojwh 08 00237Document9 pagesMojwh 08 00237EndalkNo ratings yet
- Thesis Cancer HospitalDocument7 pagesThesis Cancer HospitalCollegePaperWritingServiceCanada100% (2)
- Literature Review On Birth PreparednessDocument5 pagesLiterature Review On Birth Preparednessmgrekccnd100% (1)
- Pathogenesis Prevention Diagnosis and Treatment ofDocument18 pagesPathogenesis Prevention Diagnosis and Treatment ofMubarak Abubakar yaroNo ratings yet
- A Review of 10 Years of Vasectomy Programming andDocument14 pagesA Review of 10 Years of Vasectomy Programming andtashaNo ratings yet
- Guideline 2013 Breast Recon Expanders ImplantsDocument23 pagesGuideline 2013 Breast Recon Expanders ImplantsBogdan TudorNo ratings yet
- Improving Mammography ScreeningDocument8 pagesImproving Mammography ScreeningsylviaramisNo ratings yet
- Evidence-Based Practice in Maternal and Child HealthDocument1 pageEvidence-Based Practice in Maternal and Child HealthKaycee JoyNo ratings yet
- Oup Accepted Manuscript 2018Document7 pagesOup Accepted Manuscript 2018FaidurrahmanNo ratings yet
- FTP Three-Year Analysis of Treatment Efficacy, Cosmesis and ToxicityDocument9 pagesFTP Three-Year Analysis of Treatment Efficacy, Cosmesis and ToxicitySara SánNo ratings yet
- 5223-Article Text-23037-2-10-20200913Document10 pages5223-Article Text-23037-2-10-20200913m.sandra12340No ratings yet
- Preconception Health and Care: A Life Course ApproachFrom EverandPreconception Health and Care: A Life Course ApproachJill ShaweNo ratings yet
- Ijams: Parent-Assisted Learning Awareness and Performance of The Grade 7 Students in EnglishDocument12 pagesIjams: Parent-Assisted Learning Awareness and Performance of The Grade 7 Students in EnglishLeonilo B CapulsoNo ratings yet
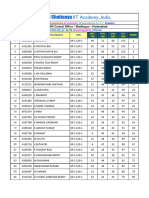
- 10-12-2023 - CTM-08 - Mains ResultsDocument21 pages10-12-2023 - CTM-08 - Mains ResultsinfinitylearmNo ratings yet
- Student Name 1st Aid 2023 Term 3Document18 pagesStudent Name 1st Aid 2023 Term 3vNo ratings yet
- First City Providential CollegeDocument4 pagesFirst City Providential Collegerommel rentoriaNo ratings yet
- Cs1020software Quality ManagementDocument1 pageCs1020software Quality Managementimmu747No ratings yet
- The Open Group IT Architect Certification: Certification Package Level 2: Master Certified IT Architect October 03, 2008 Revision 2.3Document48 pagesThe Open Group IT Architect Certification: Certification Package Level 2: Master Certified IT Architect October 03, 2008 Revision 2.3Rogerio CanoNo ratings yet
- 5CQBT05 Dang Thao Phi Vietnamese and English Verb PhrasesDocument17 pages5CQBT05 Dang Thao Phi Vietnamese and English Verb PhrasesBenjamin FranklinNo ratings yet
- Jira Ticket Templates-300124-152841Document5 pagesJira Ticket Templates-300124-152841Thu NguyenNo ratings yet
- MBA Project Guidelines-2021Document6 pagesMBA Project Guidelines-2021Madhuri BhanuNo ratings yet
- Polyglot Discord Server - Effective Learning PDFDocument8 pagesPolyglot Discord Server - Effective Learning PDFPetr BlinnikovNo ratings yet
- Brief Summary of Liminal Thinking 1 0Document7 pagesBrief Summary of Liminal Thinking 1 0Mayank SahuNo ratings yet
- Artikel 18 Kbat PecahanDocument5 pagesArtikel 18 Kbat PecahanSilvens Siga SilvesterNo ratings yet
- Dr. Kirk Kelly Cover Letter and Resume For Hamilton County School Superintendent PositionDocument2 pagesDr. Kirk Kelly Cover Letter and Resume For Hamilton County School Superintendent PositionNewsChannel 9 StaffNo ratings yet
- Senior High RoadmapDocument2 pagesSenior High Roadmapmikhael SantosNo ratings yet
- Mid Course WorkDocument112 pagesMid Course WorkT SeriesNo ratings yet
- Preston Dunlap - Sales Marketing Resume 10 23 15Document1 pagePreston Dunlap - Sales Marketing Resume 10 23 15api-299655525No ratings yet
- Introductionto RubricsDocument21 pagesIntroductionto Rubricsaa256850100% (1)
- SRC Guide 06Document192 pagesSRC Guide 06Joe EvansNo ratings yet
- Grad BulletinDocument164 pagesGrad BulletinPaulo AguilarNo ratings yet
- 2012.4 Comm Theory Scrapbook Final ProjectDocument13 pages2012.4 Comm Theory Scrapbook Final ProjectLoriAveryNo ratings yet
- SMTDocument42 pagesSMTMirjana PrekovicNo ratings yet
- Tesol Technology StandardsDocument15 pagesTesol Technology StandardsJim CabezasNo ratings yet
- Role of NursesDocument2 pagesRole of NursesShaira GumaruNo ratings yet
- 8th Karmapa, Mikyo Dorje, Life and WorksDocument536 pages8th Karmapa, Mikyo Dorje, Life and WorksSergey Sergey100% (4)
- 02 Course Structure - Fea - 19-20 - VelDocument6 pages02 Course Structure - Fea - 19-20 - Velrajamanickam sNo ratings yet
- 9th Form WritingDocument1 page9th Form WritingЧебан Агрипина 9-ВNo ratings yet