You might also like
- Beeswax Craft RecipesDocument19 pagesBeeswax Craft RecipesCpetrean100% (3)
- Stonehell Dungeon 1 Down Night Haunted Halls (LL)Document138 pagesStonehell Dungeon 1 Down Night Haunted Halls (LL)some dude100% (9)
- Form Ibpr Haul Road PDFDocument2 pagesForm Ibpr Haul Road PDFelvandi100% (1)
- Your Best Game EverDocument240 pagesYour Best Game EverUgly Panda100% (4)
- Dungeon World RevisedDocument34 pagesDungeon World RevisedMichael Welker100% (3)
- @MedicalBooksStore Mayo Clinic Body MRI Case Review (2014) PDFDocument881 pages@MedicalBooksStore Mayo Clinic Body MRI Case Review (2014) PDFKahkashan Hameed100% (1)
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- CS Risk and Crisis Management FinalDocument62 pagesCS Risk and Crisis Management FinaldangermanNo ratings yet
- Trilemma Adventures BestiaryDocument17 pagesTrilemma Adventures BestiaryZamak50% (2)
- GROUP 4 EBP On Renal NursingDocument7 pagesGROUP 4 EBP On Renal Nursingczeremar chanNo ratings yet
- Standards en 81 20 and en 81 50 - tcm45 19055 PDFDocument4 pagesStandards en 81 20 and en 81 50 - tcm45 19055 PDFSrgjan DimitrieskiNo ratings yet
- PDF Stoneell DLDocument7 pagesPDF Stoneell DLMarcin CiekalskiNo ratings yet
- Chest Imaging CasesDocument378 pagesChest Imaging CasesGeorgian Diaconu100% (1)
- Engineering ManualDocument27 pagesEngineering ManualThousif Rahman67% (3)
- Robert A. Emmons - Thanks! - How The New Science of Gratitude Can Make You HappierDocument251 pagesRobert A. Emmons - Thanks! - How The New Science of Gratitude Can Make You HappierSheilaMariePamfilo92% (24)
- Effects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasDocument5 pagesEffects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasGgssNo ratings yet
- IDPN BENEFITS FOR HD PATIENTSDocument7 pagesIDPN BENEFITS FOR HD PATIENTSCarlos Miguel Mendoza LlamocaNo ratings yet
- Ten-Year Single-Center Experience of The Ketogenic Diet: Factors in Uencing Efficacy, Tolerability, and ComplianceDocument8 pagesTen-Year Single-Center Experience of The Ketogenic Diet: Factors in Uencing Efficacy, Tolerability, and ComplianceMarcin CiekalskiNo ratings yet
- Effect of Intradialytic Parenteral Nutrition On Quality of Life in Hemodialysis PatientsDocument6 pagesEffect of Intradialytic Parenteral Nutrition On Quality of Life in Hemodialysis PatientsCarlos Miguel Mendoza LlamocaNo ratings yet
- Dietary counselling and food fortification improves outcomes in COPDDocument7 pagesDietary counselling and food fortification improves outcomes in COPDJames Cojab SacalNo ratings yet
- A.S.P.E.N. Clinical Guidelines Nutrition Support of Hospitalized Adult Patients With Obesity.Document9 pagesA.S.P.E.N. Clinical Guidelines Nutrition Support of Hospitalized Adult Patients With Obesity.Madalina TalpauNo ratings yet
- Krebs2010 PDFDocument7 pagesKrebs2010 PDFkalelNo ratings yet
- Negative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDocument8 pagesNegative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDaniela HernandezNo ratings yet
- Efficacy of the Autoimmune Protocol Diet for Inflammatory Bowel DiseaseDocument7 pagesEfficacy of the Autoimmune Protocol Diet for Inflammatory Bowel DiseaseNejc KovačNo ratings yet
- Lin 2017Document23 pagesLin 2017Marcin CiekalskiNo ratings yet
- 1 AntecedentesDocument1 page1 AntecedentesEdgar RomeroNo ratings yet
- A Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionDocument7 pagesA Prospective Randomized Controlled Trial On The Value of Prophylactic Supplementation Pral NutritionOkky IrawanNo ratings yet
- Evaluating The Quality of Life of Adult Patients oDocument1 pageEvaluating The Quality of Life of Adult Patients opspd anakNo ratings yet
- Nutrients: Micronutrient Status in 153 Patients With Anorexia NervosaDocument10 pagesNutrients: Micronutrient Status in 153 Patients With Anorexia NervosaReza Yusna HanastaNo ratings yet
- Intestinal - Rehabilitation - Programs - in - The Pediatric Failure and Shhort Bowel SyndromeDocument9 pagesIntestinal - Rehabilitation - Programs - in - The Pediatric Failure and Shhort Bowel SyndromeMinosska Pinto LazoNo ratings yet
- 11 JCO-2005-Ravasco-1431-8Document8 pages11 JCO-2005-Ravasco-1431-8Samuel Kyei-BoatengNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDocument13 pagesRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoNo ratings yet
- Journal Stress OksidatifDocument8 pagesJournal Stress OksidatifMiftakhur RohmahNo ratings yet
- Subjective Global Nutrition Assessment ChildrenDocument7 pagesSubjective Global Nutrition Assessment Childrenmaricarmen IbarraNo ratings yet
- Risk of Small Intestinal Bacterial Overgrowth in Patients Receiving Proton Pump Inhibitors Versus Proton Pump Inhibitors Plus ProkineticsDocument7 pagesRisk of Small Intestinal Bacterial Overgrowth in Patients Receiving Proton Pump Inhibitors Versus Proton Pump Inhibitors Plus ProkineticsfalmvenNo ratings yet
- HHS Public Access: Intermittent Fasting: Is The Wait Worth The Weight?Document22 pagesHHS Public Access: Intermittent Fasting: Is The Wait Worth The Weight?Franklin Howley-Dumit SerulleNo ratings yet
- Faecal Microbial Flora and Disease Activity in Rheumatoid Arthritis During A Vegan DietDocument5 pagesFaecal Microbial Flora and Disease Activity in Rheumatoid Arthritis During A Vegan DietHendra SudaryonoNo ratings yet
- Gastrico Vs TranspiloricaDocument6 pagesGastrico Vs TranspiloricaMagali FloresNo ratings yet
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaNo ratings yet
- Corticosteroid Dosing in Pediatric Acute Severe Ulcerative Colitis: A Propensity Score AnalysisDocument7 pagesCorticosteroid Dosing in Pediatric Acute Severe Ulcerative Colitis: A Propensity Score AnalysisfandyNo ratings yet
- Article CritiqueDocument5 pagesArticle Critiqueapi-437831510No ratings yet
- Apt 12695Document13 pagesApt 12695Hadi KuriryNo ratings yet
- Eichen - Case Study SboDocument30 pagesEichen - Case Study Sboapi-246480452No ratings yet
- Chiba 2018Document9 pagesChiba 2018Fred MeyerNo ratings yet
- GIZIDO Volume 6 No. 2 November 2014 Suplementasi Protein Vera T. Harikedua, DKKDocument9 pagesGIZIDO Volume 6 No. 2 November 2014 Suplementasi Protein Vera T. Harikedua, DKKFatrah MokodompitNo ratings yet
- On Dan SentronDocument7 pagesOn Dan SentronLia MirawatiNo ratings yet
- Both Fecal Calprotectin and Imuno Test in Children IBDDocument13 pagesBoth Fecal Calprotectin and Imuno Test in Children IBDdichafrNo ratings yet
- Gastritis AutoinmunrDocument15 pagesGastritis Autoinmunrfiolit13No ratings yet
- 10 6133@apjcn 2015 24 1 07Document9 pages10 6133@apjcn 2015 24 1 07Lilik FitrianaNo ratings yet
- Gastroenteritis Therapies in Developed Countries: Systematic Review and Meta-AnalysisDocument21 pagesGastroenteritis Therapies in Developed Countries: Systematic Review and Meta-AnalysisMarinaNo ratings yet
- AbstractsDocument92 pagesAbstractsmissrinwaNo ratings yet
- Implementation of Dietitian Recommendations For Enteral Nutrition Results in Improved OutcomesDocument4 pagesImplementation of Dietitian Recommendations For Enteral Nutrition Results in Improved OutcomesAlHanouf ASNo ratings yet
- Global Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDocument5 pagesGlobal Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDea SaptanovaNo ratings yet
- Drisko 2006Document10 pagesDrisko 2006Elton MatsushimaNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityJosé Luis ChavesNo ratings yet
- Ruth 2013Document17 pagesRuth 2013Paul SimononNo ratings yet
- Can Postoperative Nutrition Be Favourably Maintained by Oral Diet in Patients With Emergency Temporary Ileostomy? A Tertiary Hospital Based StudyDocument5 pagesCan Postoperative Nutrition Be Favourably Maintained by Oral Diet in Patients With Emergency Temporary Ileostomy? A Tertiary Hospital Based StudydwirizqillahNo ratings yet
- Artigo - Compliance Oral Nutrition Supplement - ReviewDocument20 pagesArtigo - Compliance Oral Nutrition Supplement - ReviewFrancielle A.RNo ratings yet
- 16 Original 12Document9 pages16 Original 12Andrés Reyes JaraNo ratings yet
- Internasional PDFDocument7 pagesInternasional PDFseptianarifwandiniNo ratings yet
- Clinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese HospitalsDocument9 pagesClinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese Hospitalsmarco marcoNo ratings yet
- Update On Total Parenteral Nutrition: EditorialDocument2 pagesUpdate On Total Parenteral Nutrition: EditorialJavier VegaNo ratings yet
- Li 2021Document8 pagesLi 2021Neil Patrick AngelesNo ratings yet
- Relationship between nutrition knowledge and intake of energy, protein, phosphorus, and potassium in CKD patients undergoing regular hemodialysisDocument7 pagesRelationship between nutrition knowledge and intake of energy, protein, phosphorus, and potassium in CKD patients undergoing regular hemodialysisDaniel DarmawanNo ratings yet
- Therapeutic effects of zinc on acute diarrhea in childrenDocument7 pagesTherapeutic effects of zinc on acute diarrhea in childrenRizqulloh Taufiqul Hakim BarsahNo ratings yet
- 2014 Guideline For The Evaluation of Cholestatic Jaundice in InfantsDocument61 pages2014 Guideline For The Evaluation of Cholestatic Jaundice in InfantsHenry BarberenaNo ratings yet
- J Pediatr 2010 Mar 156 (3) 382-7Document9 pagesJ Pediatr 2010 Mar 156 (3) 382-7Hugo Velázquez GarciaNo ratings yet
- ESPEN Inflammatory Bowel DiseaseDocument27 pagesESPEN Inflammatory Bowel Diseasesilvio da costa guerreiroNo ratings yet
- Zhang 2020Document14 pagesZhang 2020Belen GaleraNo ratings yet
- Nutritional Status and Dietary Management According To Hemodialysis DurationDocument8 pagesNutritional Status and Dietary Management According To Hemodialysis DurationVione rizkiNo ratings yet
- Ketogenic Diet in Advanced Cancer A Pilot Feasibility and Safety Trial in The Veterans Affairs Cancer Patient Population 2167 0870.1000149Document5 pagesKetogenic Diet in Advanced Cancer A Pilot Feasibility and Safety Trial in The Veterans Affairs Cancer Patient Population 2167 0870.1000149maz mouNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- Avoiding Harm When Feeding Critically Ill PatientsDocument1 pageAvoiding Harm When Feeding Critically Ill PatientsthegridfanNo ratings yet
- SGNA NinosDocument7 pagesSGNA NinosjorgeNo ratings yet
- Essential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookFrom EverandEssential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookNo ratings yet
- Radiology Case Review Series: Interventional Radiology: March 2014Document2 pagesRadiology Case Review Series: Interventional Radiology: March 2014Marcin CiekalskiNo ratings yet
- Campaign Creator Print File - TabloidDocument10 pagesCampaign Creator Print File - TabloidYannarNo ratings yet
- Mothership Hive Mind (Issue 01)Document40 pagesMothership Hive Mind (Issue 01)Marcin CiekalskiNo ratings yet
- Systematic Review of Ketogenic Diet Use in Adult Patients With Status EpilepticusDocument12 pagesSystematic Review of Ketogenic Diet Use in Adult Patients With Status EpilepticusMarcin CiekalskiNo ratings yet
- Worlds of AdventureDocument41 pagesWorlds of AdventureVolneyNo ratings yet
- A Prospective Study: Growth and Nutritional Status of Children Treated With The Ketogenic DietDocument6 pagesA Prospective Study: Growth and Nutritional Status of Children Treated With The Ketogenic DietMarcin CiekalskiNo ratings yet
- Homebrew World 1.5.1Document24 pagesHomebrew World 1.5.1Marcin CiekalskiNo ratings yet
- Accepted Manuscript: 10.1016/j.nut.2013.11.017Document25 pagesAccepted Manuscript: 10.1016/j.nut.2013.11.017Marcin CiekalskiNo ratings yet
- Lin 2017Document23 pagesLin 2017Marcin CiekalskiNo ratings yet
- Duconmix CRP 400Document2 pagesDuconmix CRP 400FounTech612No ratings yet
- Sps 500 (STD) ProgramDocument164 pagesSps 500 (STD) Programwahyu100% (1)
- Exxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDocument6 pagesExxonmobil High Density Polyethylene Product Guide: Extrusion MoldingDaikinllcNo ratings yet
- SorghumDocument13 pagesSorghumMohaajanan AliNo ratings yet
- 4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipesDocument2 pages4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipespeteNo ratings yet
- CardiovascularDocument155 pagesCardiovascularEric VeranoNo ratings yet
- Reactor & Impeller Design in Hydrogenation: GBHE Technical Bulletin CTB #79Document13 pagesReactor & Impeller Design in Hydrogenation: GBHE Technical Bulletin CTB #79manuNo ratings yet
- The QuestionnaireDocument3 pagesThe QuestionnaireMaximo C. Nayanga Jr.No ratings yet
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- Technical Data Sheet PDFDocument2 pagesTechnical Data Sheet PDFLuis VilelaNo ratings yet
- Ecosystem Components and InteractionsDocument31 pagesEcosystem Components and InteractionsBirraa TajuNo ratings yet
- Benign EntitiesDocument37 pagesBenign EntitiesleartaNo ratings yet
- Understanding Immunomodulatory DrugsDocument4 pagesUnderstanding Immunomodulatory DrugsMark Russel Sean LealNo ratings yet
- 4 ReactorsDocument58 pages4 ReactorsKiran ShresthaNo ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
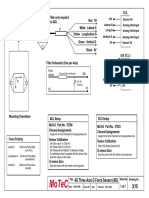
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- ELCO Brochure FGR (ENG) 1.2Document16 pagesELCO Brochure FGR (ENG) 1.2Mohd Bismillah AnsariNo ratings yet
- Performance Evaluation of Sewage Treatment Plants (STPS) in Multistoried BuildingsDocument6 pagesPerformance Evaluation of Sewage Treatment Plants (STPS) in Multistoried BuildingsAnonymous iTzCnMNo ratings yet
- 2requirements Permit PDFDocument1 page2requirements Permit PDFHazel CorralNo ratings yet
- Predicting Natural Hazards PowerPointDocument29 pagesPredicting Natural Hazards PowerPointZarlene SierraNo ratings yet
- Casa de Moda DolcegabbanaDocument4 pagesCasa de Moda Dolcegabbanadianaionelav23No ratings yet
- Candidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Document3 pagesCandidate 1 (Reservoir Engineering Panel) : ONGC SAMPLE INTERVIEW QUESTIONS (Based Upon Memory of Appeared Candidates)Neha AhiraoNo ratings yet
- Refrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 ObjectivesDocument10 pagesRefrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 Objectivesjhon milliNo ratings yet