You might also like
- Brain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1From EverandBrain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1No ratings yet
- Neurological ExaminationDocument5 pagesNeurological Examinationshubham rathodNo ratings yet
- Fact Sheet - Assessment Following Brain InjuryDocument7 pagesFact Sheet - Assessment Following Brain InjurySuman DeyNo ratings yet
- NEUROEXAMCHECKLISTDocument5 pagesNEUROEXAMCHECKLISTDarleneNo ratings yet
- Assessment of The Neurologic SystemDocument54 pagesAssessment of The Neurologic SystemPark chin-haeNo ratings yet
- General Neurological AssessmentDocument6 pagesGeneral Neurological Assessmenthellfire222No ratings yet
- Hypoxic-Ischaemic Encephalopathy (HIE) : Maternity and Neonatal Clinical GuidelineDocument27 pagesHypoxic-Ischaemic Encephalopathy (HIE) : Maternity and Neonatal Clinical GuidelineGordon InformationNo ratings yet
- Glasgow Coma Scale. GCS.Document3 pagesGlasgow Coma Scale. GCS.Amanda Rodriguez TejedaNo ratings yet
- How To Assess Reflexes - Neurologic Disorders - MSD Manual Professional EditionDocument3 pagesHow To Assess Reflexes - Neurologic Disorders - MSD Manual Professional Editionsiddhi meenaNo ratings yet
- Assessment: The Neurologic Exam: InterviewDocument10 pagesAssessment: The Neurologic Exam: InterviewJun ManNo ratings yet
- Neuro AssessmentDocument13 pagesNeuro Assessmentyassyrn100% (2)
- Neurologic Disorders:: Anatomy & PhysiologyDocument9 pagesNeurologic Disorders:: Anatomy & PhysiologyMaria Erlene SantosNo ratings yet
- Assessing The Neurological SystemDocument7 pagesAssessing The Neurological SystemEs CarlNo ratings yet
- Neuro and Cranial Nerve Assessment GuideDocument1 pageNeuro and Cranial Nerve Assessment GuidepriyaNo ratings yet
- NVS Written ReportDocument20 pagesNVS Written ReportbabiNo ratings yet
- Neurological AssessmentDocument8 pagesNeurological AssessmentSachin ParamashettiNo ratings yet
- Wall Neuro 2010Document34 pagesWall Neuro 2010Kath Jacinto100% (1)
- Glasgow Coma ScaleDocument3 pagesGlasgow Coma ScaleMaromi RaniloNo ratings yet
- Central Nervous System Examination: Overview & PurposeDocument5 pagesCentral Nervous System Examination: Overview & PurposebismahNo ratings yet
- Lec. 3 Providing Nursing Care of The Newborn 1-1Document62 pagesLec. 3 Providing Nursing Care of The Newborn 1-1talarashad2002No ratings yet
- Neurological AssessmentDocument5 pagesNeurological AssessmentVIDYANo ratings yet
- Assessment Nursing Diagnosis Planning Evaluation: Either Awake or Can Be Readily Awakened From Normal SleepDocument3 pagesAssessment Nursing Diagnosis Planning Evaluation: Either Awake or Can Be Readily Awakened From Normal SleepCharmaine Anne Olalde JulianoNo ratings yet
- Neurology - Part 2Document12 pagesNeurology - Part 2Fritz MirandaNo ratings yet
- 1 - Neuro Assessment 2021 - 336Document30 pages1 - Neuro Assessment 2021 - 336HADI BADWAN100% (2)
- 1300 1330 Valasek Treatment For Muscle Tension DysphoniaDocument10 pages1300 1330 Valasek Treatment For Muscle Tension DysphoniaGautam MalhotraNo ratings yet
- Dysphagia EBP HANDOUT FINALDocument1 pageDysphagia EBP HANDOUT FINALAnnabelleNo ratings yet
- Inbound 2795149120147640433Document52 pagesInbound 2795149120147640433elainemNo ratings yet
- Enls V 4 0 Protocol Antw FinalDocument28 pagesEnls V 4 0 Protocol Antw Finalsucipto suciptoNo ratings yet
- EINC2 - Students' NotesDocument5 pagesEINC2 - Students' NotesLau RenNo ratings yet
- Learning Objectives For EXAM 1Document13 pagesLearning Objectives For EXAM 1bcvaughn019No ratings yet
- Neurological ExaminationDocument14 pagesNeurological Examinationwam.ahNo ratings yet
- Cerebellar Examination OSCE GuideDocument11 pagesCerebellar Examination OSCE GuideLeen abusarhanNo ratings yet
- Central Nervous System AssessmentDocument37 pagesCentral Nervous System AssessmentVIDYANo ratings yet
- Case Analysis: Neuro CaseDocument7 pagesCase Analysis: Neuro CaseKyle AndrewNo ratings yet
- Screenshot - TMJ and Head ComplexDocument5 pagesScreenshot - TMJ and Head Complexno nameNo ratings yet
- So After ABC - Neuro-IsabilityDocument5 pagesSo After ABC - Neuro-IsabilityXavier FungNo ratings yet
- 7 Detailed Cranial Nerve ExamDocument3 pages7 Detailed Cranial Nerve Exambsm8gf6szxNo ratings yet
- Newborn Nursing Care Plan With ReferncesDocument6 pagesNewborn Nursing Care Plan With Referncesneuronurse92% (63)
- W2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsDocument6 pagesW2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsKyla L. Madjad100% (1)
- Cranial NerveDocument3 pagesCranial NerveMatty JolbitadoNo ratings yet
- Glasgow Coma Scale or GCS Is A: Best Eye Response (E)Document3 pagesGlasgow Coma Scale or GCS Is A: Best Eye Response (E)Eunice Kristia EsteleydesNo ratings yet
- Azrin and Nunn 1973 Habit Reversal A Method of Eliminating Nervous Habits and TicsDocument10 pagesAzrin and Nunn 1973 Habit Reversal A Method of Eliminating Nervous Habits and TicsDavid ThomsonNo ratings yet
- 1.halliwck Child Principios - Halliwick - en - Nino PDFDocument7 pages1.halliwck Child Principios - Halliwick - en - Nino PDFmuhammad yaminNo ratings yet
- Appendix: Field Neurological AssessmentDocument10 pagesAppendix: Field Neurological AssessmentLeon LellaNo ratings yet
- Nystagmus 1Document35 pagesNystagmus 1syed mohammed hussain100% (1)
- All Clinical Examinations GuideDocument29 pagesAll Clinical Examinations Guideasalizwa ludlalaNo ratings yet
- CNS AhnDocument190 pagesCNS Ahni am sigmaNo ratings yet
- Assesment of NewbornDocument3 pagesAssesment of NewbornBhawna PandhuNo ratings yet
- Neurological AssessmentDocument18 pagesNeurological AssessmentMackenzie GaranNo ratings yet
- 01 Neurologic Conditions W 2 PDFDocument127 pages01 Neurologic Conditions W 2 PDFGerald BatugalNo ratings yet
- NCM 116 RLE Week 3Document32 pagesNCM 116 RLE Week 3Christel Mariz SantellaNo ratings yet
- Script For OrientationDocument2 pagesScript For OrientationAngela CudiaNo ratings yet
- Pediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TDocument30 pagesPediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TCharisse Ann GasatayaNo ratings yet
- Posture: Sign Neuro-Muscular Maturity Score Sign ScoreDocument14 pagesPosture: Sign Neuro-Muscular Maturity Score Sign ScoreerylekateNo ratings yet
- NCP For StrokeDocument4 pagesNCP For StrokeJASON OGALESCONo ratings yet
- Examination of The CNS in Children: Professor Low Poh Sim Department of Paediatrics UcmiDocument40 pagesExamination of The CNS in Children: Professor Low Poh Sim Department of Paediatrics UcmiVanessa HermioneNo ratings yet
- 7.1 Altered PerceptionDocument129 pages7.1 Altered PerceptionAlexander Blanche PajelaNo ratings yet
- Maximising Your Intellectual Abilities: Learn how to make the most of your intelligenceFrom EverandMaximising Your Intellectual Abilities: Learn how to make the most of your intelligenceNo ratings yet
- Applicationform Draft Print For AllDocument3 pagesApplicationform Draft Print For AllRajveerNo ratings yet
- Application Form Draft Print For AllDocument3 pagesApplication Form Draft Print For AllRajveerNo ratings yet
- Application Form Draft Print For AllDocument3 pagesApplication Form Draft Print For AllRajveerNo ratings yet
- 05 03 2020 Ergonomics at The Work Place RMH CPD 05.03.2020Document43 pages05 03 2020 Ergonomics at The Work Place RMH CPD 05.03.2020RajveerNo ratings yet
- SpeakerDocument25 pagesSpeakerRajveerNo ratings yet
- Application Form Draft Print For AllDocument3 pagesApplication Form Draft Print For AllRajveerNo ratings yet
- Application Form Draft Print For AllDocument4 pagesApplication Form Draft Print For AllRajveerNo ratings yet
- Cms - Ed Prospectus-1Document19 pagesCms - Ed Prospectus-1RajveerNo ratings yet
- List of Fake Universities As On 10 08 1994 To Till Date EnglishDocument49 pagesList of Fake Universities As On 10 08 1994 To Till Date EnglishRajveerNo ratings yet
- BreathlessnessDocument29 pagesBreathlessnessRajveerNo ratings yet
- Prospect of Pharmacy CourseDocument3 pagesProspect of Pharmacy CourseRajveerNo ratings yet
- Abdominal IncisionsDocument39 pagesAbdominal IncisionsRajveerNo ratings yet
- Roprioceptive Euromuscular AcilitationDocument24 pagesRoprioceptive Euromuscular AcilitationRajveerNo ratings yet
- Heart SoundsDocument36 pagesHeart SoundsRajveer100% (1)
- Brain Functional AreasDocument1 pageBrain Functional AreasRajveerNo ratings yet
- Cerebrum 130906013333Document12 pagesCerebrum 130906013333RajveerNo ratings yet
- Brachial PlexusDocument5 pagesBrachial PlexusRajveerNo ratings yet
- Bell's PalsyDocument9 pagesBell's PalsyRajveerNo ratings yet
- Spinal StabilityDocument14 pagesSpinal StabilityRajveerNo ratings yet
- Nerve Injury Classification, Nerve Degeneration, Regeneration and Repair TechniquesDocument50 pagesNerve Injury Classification, Nerve Degeneration, Regeneration and Repair TechniquesRajveerNo ratings yet
- Arthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveDocument4 pagesArthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveRajveerNo ratings yet
- Discover K Taping®: Course CatalogueDocument28 pagesDiscover K Taping®: Course CatalogueRajveerNo ratings yet
- Q AngleDocument4 pagesQ AngleRajveerNo ratings yet
- Rood's ApproachDocument11 pagesRood's ApproachRajveer100% (1)
- Delayed and MalunionDocument3 pagesDelayed and MalunionRajveerNo ratings yet
- SOAP Notes: HistoryDocument5 pagesSOAP Notes: HistoryRajveerNo ratings yet
- Sop For Covid 19Document16 pagesSop For Covid 19RajveerNo ratings yet
- AmjadDocument1 pageAmjadRajveerNo ratings yet
- Eating Attitudes Test (EAT-40) J-swinbourne-ThesisDocument442 pagesEating Attitudes Test (EAT-40) J-swinbourne-ThesisMilosNo ratings yet
- Stat501.101 SU14Document2 pagesStat501.101 SU14Hafizah HalimNo ratings yet
- Submitted By:: Tarnate, Hazel R. Bsba - 4B Submitted To: Professor Renilda MartinezDocument28 pagesSubmitted By:: Tarnate, Hazel R. Bsba - 4B Submitted To: Professor Renilda MartinezRomeo Fernon Sto. DomingoNo ratings yet
- Agoraphobia 1Document47 pagesAgoraphobia 1We Are HanakoNo ratings yet
- Nutech University Admission SlipDocument3 pagesNutech University Admission SlipaliiiiNo ratings yet
- Krista Pankau Cover LetterDocument3 pagesKrista Pankau Cover Letterapi-514564329No ratings yet
- (M2-MAIN) The Self From Various PerspectivesDocument120 pages(M2-MAIN) The Self From Various PerspectivesAngelo Payod100% (1)
- The Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationDocument4 pagesThe Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationSebastian PorcelNo ratings yet
- q2 Lesson 9 Concept PaperDocument4 pagesq2 Lesson 9 Concept PaperShiela May DelacruzNo ratings yet
- DR Ranjith CV PDFDocument4 pagesDR Ranjith CV PDFRanjith ArNo ratings yet
- College of Business and EconomicsDocument12 pagesCollege of Business and EconomicsMoti KasaNo ratings yet
- World War Two Unit PlanDocument22 pagesWorld War Two Unit Planapi-280689729100% (1)
- All English TensesDocument5 pagesAll English TensesIkram0% (1)
- Mode of VerificationDocument15 pagesMode of VerificationVincent LibreaNo ratings yet
- Hartmann 1931Document12 pagesHartmann 1931Matheus Pereira CostaNo ratings yet
- Brigada Eskwela Activities With PicsDocument6 pagesBrigada Eskwela Activities With PicsCharisse TocmoNo ratings yet
- Research 11 3Document3 pagesResearch 11 3Josefa GandaNo ratings yet
- Information Technology Project Management - Fifth Edition: by Jack T. Marchewka Northern Illinois UniversityDocument31 pagesInformation Technology Project Management - Fifth Edition: by Jack T. Marchewka Northern Illinois UniversitytofuNo ratings yet
- Chess With MatthewDocument9 pagesChess With MatthewsalihNo ratings yet
- HIST123 - Chapter - Church of The Immaculate Conception, SpinkhillDocument3 pagesHIST123 - Chapter - Church of The Immaculate Conception, SpinkhillcheggNo ratings yet
- SCIENCE G8-Q2-Module 4Document18 pagesSCIENCE G8-Q2-Module 4honey g100% (1)
- Bystander Effect Corpuz&Reyes BSPsyIIIDocument16 pagesBystander Effect Corpuz&Reyes BSPsyIIIJanine Mae Villostas CorpuzNo ratings yet
- Advances in Teaching Sign Language Interpreters Chp1Document30 pagesAdvances in Teaching Sign Language Interpreters Chp1Lucanezul100% (1)
- Gr5.Mathematics Teachers Guide JPDocument149 pagesGr5.Mathematics Teachers Guide JPRynette FerdinandezNo ratings yet
- Probability Calculation in MinesweeperDocument2 pagesProbability Calculation in MinesweeperBrayan Perez ContrerasNo ratings yet
- VONG 1 - 2020-2021 - Key - CTDocument2 pagesVONG 1 - 2020-2021 - Key - CTKhánh LinhNo ratings yet
- Etd 2017 8048Document323 pagesEtd 2017 8048Rafaely VelosoNo ratings yet
- Commerce BrochureDocument3 pagesCommerce BrochureSampath KumarNo ratings yet
- ESPEN LLL - Registration & Module Download GuideDocument18 pagesESPEN LLL - Registration & Module Download GuidePandu HarsarapamaNo ratings yet
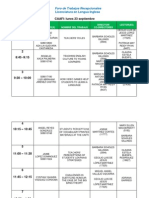
- Foro de ER - Sept - FinalThisOneDocument5 pagesForo de ER - Sept - FinalThisOneAbraham CastroNo ratings yet