You might also like
- ICJ Case Summary: Antara v. Ravaria Suthan Referendum DisputeDocument22 pagesICJ Case Summary: Antara v. Ravaria Suthan Referendum DisputeNawaz Sharif100% (1)
- QP-SSOP-02 Condition and Cleanliness of Food Contact Surfaces - v1.0Document2 pagesQP-SSOP-02 Condition and Cleanliness of Food Contact Surfaces - v1.0Marisse CruzNo ratings yet
- Positioning TableDocument12 pagesPositioning TableJonathanNo ratings yet
- The Idea of Indigenous PeopleDocument7 pagesThe Idea of Indigenous PeopleShah KamaruzamanNo ratings yet
- KFC TeachingDocument24 pagesKFC TeachingJai VNo ratings yet
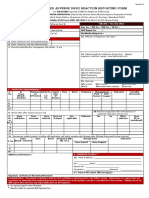
- ADRnewReporting Form 1.4Document2 pagesADRnewReporting Form 1.4Sourabh kundara0% (1)
- Final Case Study Neuro 1Document3 pagesFinal Case Study Neuro 1api-390014321No ratings yet
- Complete Eye Exam GuideDocument20 pagesComplete Eye Exam GuideJhaztene Mae BaniquedNo ratings yet
- The New Epoch - Codex 2 - EquipmentDocument126 pagesThe New Epoch - Codex 2 - EquipmentJonathan FriedmanNo ratings yet
- 10th English 1Document35 pages10th English 1PoojaNo ratings yet
- POSAV V5 Ethernet Disk Logging ICD Rev18Document117 pagesPOSAV V5 Ethernet Disk Logging ICD Rev18Filip SkultetyNo ratings yet
- Research Paper Chapter 1 3Document34 pagesResearch Paper Chapter 1 3Lyca jean PascuaNo ratings yet
- Patient Care Handouts October 2021Document16 pagesPatient Care Handouts October 2021Saadventure dobidobiNo ratings yet
- Motor Neuron Disease GuideDocument5 pagesMotor Neuron Disease Guidekath-kathNo ratings yet
- Assessment of OrthopedicVersus Neurologic Causes of Gait Change in Dogs and CatsDocument9 pagesAssessment of OrthopedicVersus Neurologic Causes of Gait Change in Dogs and CatsAristoteles Esteban Cine VelazquezNo ratings yet
- Sample Output From Hazard Hunter - 160705-Hazard-Assessment-ReportDocument7 pagesSample Output From Hazard Hunter - 160705-Hazard-Assessment-ReportrollramsNo ratings yet
- High Median Nerve InjuriesDocument10 pagesHigh Median Nerve InjuriesKarime TapiaNo ratings yet
- LPRZTDocument2 pagesLPRZTjaydrath sindhavNo ratings yet
- Combination Control Module Models 170, 210Document37 pagesCombination Control Module Models 170, 210Vu HoiNo ratings yet
- Mohit Sharma Vertical HeadDocument3 pagesMohit Sharma Vertical HeadKriday SharmaNo ratings yet
- Vibrio CholeraeDocument14 pagesVibrio CholeraeAnzo SimonNo ratings yet
- Nazdar 2300 Uv Uv-Led Screen Ink SeriesDocument5 pagesNazdar 2300 Uv Uv-Led Screen Ink SeriesEduardo Ruiz JrNo ratings yet
- TNTR - IFHRMS - EMPLOYEES - PAYSLIP - USER MANUAL - ENGLISH - VERSION 1.1Document15 pagesTNTR - IFHRMS - EMPLOYEES - PAYSLIP - USER MANUAL - ENGLISH - VERSION 1.1uvaarajNo ratings yet
- Form No. Ogfr-2 (See Rule-63)Document3 pagesForm No. Ogfr-2 (See Rule-63)kajal sahuNo ratings yet
- Human Eye ? and The Colourful WorldDocument19 pagesHuman Eye ? and The Colourful WorldNivas KumarNo ratings yet
- Corporate finance quizDocument43 pagesCorporate finance quizPriyanka MahajanNo ratings yet
- BIOLOGYExamDocument3 pagesBIOLOGYExamDanna SanchezNo ratings yet
- Alinhador Fixturlaser DirigoDocument2 pagesAlinhador Fixturlaser DirigoJossesmsNo ratings yet
- Albert's Diamond Jewelers ComplaintDocument17 pagesAlbert's Diamond Jewelers ComplaintKenan FarrellNo ratings yet
- Nursing Research - InitialDocument25 pagesNursing Research - InitialNur SanaaniNo ratings yet
- Assessment of the Eyes and EarsDocument31 pagesAssessment of the Eyes and EarsShahmeerNo ratings yet
- Marathon NotesDocument341 pagesMarathon NotesLokesh Agarwalla100% (1)
- CSPs MPT Test-II and KeyDocument16 pagesCSPs MPT Test-II and KeyAbdul Aleem Khoso100% (1)
- Silicone Oil in Vitreoretinal SurgeryDocument30 pagesSilicone Oil in Vitreoretinal SurgeryBhumika RathNo ratings yet
- MATLAB Practical File (Codes) by Priyanshu SinhaDocument35 pagesMATLAB Practical File (Codes) by Priyanshu SinhaPriyanshu SinhaNo ratings yet
- ENG MATH 2 IM No.21Document4 pagesENG MATH 2 IM No.21Ghea SafiloNo ratings yet
- Moeller DM4 ManualDocument194 pagesMoeller DM4 ManualFranco Sanchez QuirogaNo ratings yet
- CASE STUDY-RAJAHMUNDRY - ED - ApprovedDocument3 pagesCASE STUDY-RAJAHMUNDRY - ED - ApprovedInderjeet HoodaNo ratings yet
- Liu 2013Document3 pagesLiu 2013Gonzalo BenavidesNo ratings yet
- Iep BlackedDocument8 pagesIep Blackedapi-652789369No ratings yet
- BS 2151.01, 2151.011-U Manual de ManttoDocument28 pagesBS 2151.01, 2151.011-U Manual de ManttoAndrés Rivera MartínezNo ratings yet
- Cif Flag Football RulesDocument15 pagesCif Flag Football Rulesapi-573133901No ratings yet
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocument55 pagesFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997No ratings yet
- CM 725 Technical Data SheetDocument2 pagesCM 725 Technical Data SheetNarimane Benty100% (1)
- NCM 103 Rle: Far Eastern University - Nicanor Reyes Medical FoundationDocument4 pagesNCM 103 Rle: Far Eastern University - Nicanor Reyes Medical FoundationMarby BalingdanNo ratings yet
- TFN Case ScenarioDocument13 pagesTFN Case ScenarioDUQUE, GEORGETTE FLOREANNE L.No ratings yet
- Provisional Certificate BSc MLT Pass MarksDocument5 pagesProvisional Certificate BSc MLT Pass MarksPraveen PraviNo ratings yet
- Attock Refinery Limited: Low Gravity Residual Fuel OilDocument7 pagesAttock Refinery Limited: Low Gravity Residual Fuel OilshahNo ratings yet
- BORROWING COST CALCULATIONSDocument4 pagesBORROWING COST CALCULATIONSKiran Kumar KBNo ratings yet
- Harris SX-1 Operators ManualDocument46 pagesHarris SX-1 Operators ManualLuis AhmedNo ratings yet
- Curriculumguide 2324Document35 pagesCurriculumguide 2324api-331852116No ratings yet
- The Basics LearnIt WebSAMPLEDocument22 pagesThe Basics LearnIt WebSAMPLEPhong Lê ĐìnhNo ratings yet
- Monarchies - StudentDocument8 pagesMonarchies - StudentBispo Miguel ÂngeloNo ratings yet
- Renaissance Physicians Guide to Facial Beauty MaximizationDocument31 pagesRenaissance Physicians Guide to Facial Beauty MaximizationKentVilandkaNo ratings yet
- Oil and Natural Gas Corporation Limited Ankleshwar Asset, AnkleshwarDocument8 pagesOil and Natural Gas Corporation Limited Ankleshwar Asset, Ankleshwardattesh vasavaNo ratings yet
- Cambridge IGCSE™: Geography 0460/12 May/June 2021Document18 pagesCambridge IGCSE™: Geography 0460/12 May/June 2021Aja Saidylee.No ratings yet
- G-Force Watch Ltd 2018 Profits Tax CalculationDocument7 pagesG-Force Watch Ltd 2018 Profits Tax Calculation日日日No ratings yet
- Imposing Native Speakers' Prosody On Non-Native (2007)Document10 pagesImposing Native Speakers' Prosody On Non-Native (2007)habib roisNo ratings yet
- iNetVu User Manual - Beacon Receiver - Rev 2.1.2Document55 pagesiNetVu User Manual - Beacon Receiver - Rev 2.1.2msyunakaNo ratings yet
- Peripheral Nerve-1Document35 pagesPeripheral Nerve-1Manirarora EtienneNo ratings yet
- Osteoporosis and OsteomalaciaDocument56 pagesOsteoporosis and OsteomalaciabismahNo ratings yet
- AcneDocument49 pagesAcnebismahNo ratings yet
- SquintDocument36 pagesSquintbismahNo ratings yet
- Role of Imaging in MSKDocument19 pagesRole of Imaging in MSKbismahNo ratings yet
- RH 2Document23 pagesRH 2bismahNo ratings yet
- Rehabilitative Management Part IIDocument23 pagesRehabilitative Management Part IIbismahNo ratings yet
- Repro CBLDocument1 pageRepro CBLbismahNo ratings yet
- Renal Tubular AcidosisDocument29 pagesRenal Tubular AcidosisbismahNo ratings yet
- Compartment SyndromeDocument13 pagesCompartment SyndromebismahNo ratings yet
- ConjunctivitisDocument15 pagesConjunctivitisbismahNo ratings yet
- Community Based RehabilitationDocument18 pagesCommunity Based RehabilitationbismahNo ratings yet
- 1 s2.0 S1665268122002186 MainDocument4 pages1 s2.0 S1665268122002186 MainJulián DuránNo ratings yet
- Allergic RhinitisDocument226 pagesAllergic RhinitisGustavo Graco100% (1)
- PERINÉ PPT - PPSXDocument10 pagesPERINÉ PPT - PPSXCuscatleca Extra suaveNo ratings yet
- Orange SurgeryDocument3 pagesOrange SurgeryMichele Fantin100% (1)
- ASJA BOYS’ COLLEGE END OF TERM EXAMDocument16 pagesASJA BOYS’ COLLEGE END OF TERM EXAMYɵʉňğ ĢênnäNo ratings yet
- Assessment of Respiratory SystemDocument34 pagesAssessment of Respiratory SystemKristal Jade Yanto Esquillo100% (1)
- Leopold - S Maneuver and Ante Post Natal ExercisesDocument21 pagesLeopold - S Maneuver and Ante Post Natal ExercisesJosefina Isabel GullasNo ratings yet
- Hemodynamic Disorders ExplainedDocument114 pagesHemodynamic Disorders ExplainedlydNo ratings yet
- Hirschsprung PathophysiologyDocument4 pagesHirschsprung PathophysiologyJona SuarezNo ratings yet
- The Immune System in Children With Malnutrition-A Systemic Review PDFDocument19 pagesThe Immune System in Children With Malnutrition-A Systemic Review PDFNadiaNo ratings yet
- 2018 - Mouse Cre-LoxP SystemDocument13 pages2018 - Mouse Cre-LoxP SystemLucas PaulaNo ratings yet
- Histiocytic SarcomaDocument8 pagesHistiocytic SarcomadanishNo ratings yet
- Hemodynamic DisordersDocument85 pagesHemodynamic DisordersTofik Mohammed100% (1)
- Cardiovascular System Physiology LectureDocument28 pagesCardiovascular System Physiology LecturevincenzoNo ratings yet
- 1st Prof MBBS Supplementary 10 Years CompilationDocument67 pages1st Prof MBBS Supplementary 10 Years CompilationDebasis PramanikNo ratings yet
- Genbio Reviewer 1Document8 pagesGenbio Reviewer 1Franchezkka Mae Belaro100% (1)
- ChloroplastDocument9 pagesChloroplastJuan Sebastian Rosero GuarinNo ratings yet
- What Is Dynamic Neuromuscular Stabilization (DNS) ?: How Is The Core Stabilized?Document5 pagesWhat Is Dynamic Neuromuscular Stabilization (DNS) ?: How Is The Core Stabilized?HONGJYNo ratings yet
- EXAM1 Study Guide Biol 211 PalomarDocument21 pagesEXAM1 Study Guide Biol 211 PalomarKathleen RussellNo ratings yet
- Tripodi 2016Document8 pagesTripodi 2016Silvia PeresNo ratings yet
- FibrinolysisDocument26 pagesFibrinolysisCristinaGheorgheNo ratings yet
- C. RicciaDocument43 pagesC. RicciaCalvin Yudha L100% (1)
- Bone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthDocument3 pagesBone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthHarsh Kumar0% (3)
- Anatomy and Physiology of Digestive SystemDocument34 pagesAnatomy and Physiology of Digestive SystemIan IsidroNo ratings yet
- Cells and Microscope Practice TestDocument6 pagesCells and Microscope Practice TestlevchapNo ratings yet
- Absorption of Water and Minerals by RootsDocument2 pagesAbsorption of Water and Minerals by RootsOlivia LinNo ratings yet
- Childrens FBC Reference Ranges PDFDocument1 pageChildrens FBC Reference Ranges PDFCerianne BodionganNo ratings yet
- 4 Hodges and Tucker. Moving Differently in Pain. 2011Document9 pages4 Hodges and Tucker. Moving Differently in Pain. 2011ningaxshopNo ratings yet
- A Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportDocument6 pagesA Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportIJAR JOURNALNo ratings yet
- Gross and Histomorphological Study of The Ovary and Oviduct of Turkey Hen With Especial Emphasis On The Sperm-Host GlandDocument8 pagesGross and Histomorphological Study of The Ovary and Oviduct of Turkey Hen With Especial Emphasis On The Sperm-Host GlandImam HasanNo ratings yet