You might also like
- Daily Plant Inspection ChecklistDocument1 pageDaily Plant Inspection Checklist8460272421No ratings yet
- Citroen C4 Picasso/Grand Picasso BilmetropolenDocument5 pagesCitroen C4 Picasso/Grand Picasso BilmetropolenAlberto Miglino100% (1)
- Daily Plant Inspection ChecklistDocument2 pagesDaily Plant Inspection ChecklistFeroz Gull100% (1)
- Heavy Equipment Inspection ChecklistDocument18 pagesHeavy Equipment Inspection ChecklistJuned Hamid Khan89% (9)
- Form 000.653.F0107c - Scissor LiftDocument2 pagesForm 000.653.F0107c - Scissor LiftMaitham Titan0% (1)
- Daily Plant Inspection ChecklistDocument2 pagesDaily Plant Inspection ChecklistFeroz GullNo ratings yet
- Incident Reporting Form InvestigationDocument3 pagesIncident Reporting Form InvestigationDarius Ade100% (1)
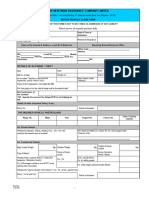
- United: Equipment Incident/Accident ReportDocument1 pageUnited: Equipment Incident/Accident Reportmalik jahanNo ratings yet
- Lamp Sesi 8.2 Investigasi SCATDocument2 pagesLamp Sesi 8.2 Investigasi SCATaab kanayaNo ratings yet
- E C 8 0520a Earthmoving Equipment Pre Mobilisation ChecklistDocument2 pagesE C 8 0520a Earthmoving Equipment Pre Mobilisation ChecklistOKPOTU GODWINNo ratings yet
- Eye-Opd 2Document16 pagesEye-Opd 2Abi Nan ThanNo ratings yet
- OHS Accident Investigation Report FormDocument2 pagesOHS Accident Investigation Report FormcoolariesatulNo ratings yet
- OMC PTW LiftingDocument2 pagesOMC PTW LiftingKarthik KarunanithiNo ratings yet
- Equipment Base Lab - 0Document15 pagesEquipment Base Lab - 0holysaatanNo ratings yet
- Checklist for Equipment Mobilization and DemobilizationDocument3 pagesChecklist for Equipment Mobilization and DemobilizationManish ChauhanNo ratings yet
- Incident Reporting Software: How To Use & Customize The TemplatesDocument23 pagesIncident Reporting Software: How To Use & Customize The TemplatesHung PhamNo ratings yet
- L02-02 Lifting Plan (Non Crane)Document2 pagesL02-02 Lifting Plan (Non Crane)Fabio CastroNo ratings yet
- Ptw-Lifting Operation (Daily) : General Information OMC Permit NoDocument2 pagesPtw-Lifting Operation (Daily) : General Information OMC Permit NoPHP DEVELOPERNo ratings yet
- Final Survey Report FormatDocument5 pagesFinal Survey Report FormatADHAR SHARMANo ratings yet
- Shovel ChecklistDocument2 pagesShovel Checklistjamal motaNo ratings yet
- Daily_Pre_Use_Checklist_Mobile_CraneDocument3 pagesDaily_Pre_Use_Checklist_Mobile_Craneahmad muzakkir mohamadNo ratings yet
- C822 Occupational Therapy Services Vehicle Modification AssessmentDocument6 pagesC822 Occupational Therapy Services Vehicle Modification AssessmentDawn CasuncadNo ratings yet
- Safety Inspection Checklist With OSHA References 2011 UpdatedDocument167 pagesSafety Inspection Checklist With OSHA References 2011 UpdatedphuyangNo ratings yet
- GB ATV-UTV Inspection FinalDocument2 pagesGB ATV-UTV Inspection Finalradu tiberiuNo ratings yet
- Form 000.653.F0107z - Air CompressorDocument1 pageForm 000.653.F0107z - Air CompressorMaitham TitanNo ratings yet
- Elevator, Escalator, and Lift Accident Report: BCD - Oregon.govDocument1 pageElevator, Escalator, and Lift Accident Report: BCD - Oregon.govMohd FadliNo ratings yet
- Job Sheet and Site-Specific Risk Assessment: Company NameDocument2 pagesJob Sheet and Site-Specific Risk Assessment: Company NameMajaga MabhenaNo ratings yet
- Employee Medical Incident ReportDocument1 pageEmployee Medical Incident ReportAiswarya SukumarNo ratings yet
- Daily Plant Inspection ChecklistDocument2 pagesDaily Plant Inspection ChecklistMuthu KumarNo ratings yet
- Contractors Plant-Claim FormDocument3 pagesContractors Plant-Claim FormCrawford BoydNo ratings yet
- Annual Fire Alarm Service ReportDocument10 pagesAnnual Fire Alarm Service ReportrisnaidiNo ratings yet
- Windscreen Claim FormDocument1 pageWindscreen Claim FormHihiNo ratings yet
- Incident Report Template PackDocument22 pagesIncident Report Template PackiSightSoftwareNo ratings yet
- Lifting Work PermitDocument1 pageLifting Work PermitRadha BuildtechNo ratings yet
- Application For Airside Vehicle Operators PermitDocument2 pagesApplication For Airside Vehicle Operators Permitt59t2c9qf5No ratings yet
- Incident Investigation Form EnglishDocument2 pagesIncident Investigation Form EnglishSayed DarwishNo ratings yet
- ics form 218, support vehicle-equipment inventory (v3)Document3 pagesics form 218, support vehicle-equipment inventory (v3)rahmawanianNo ratings yet
- At22 MaintenanceDocument37 pagesAt22 MaintenancefabuleukalengaNo ratings yet
- HSE-F-313 Passenger-Material Hoist Extension ChecklistDocument2 pagesHSE-F-313 Passenger-Material Hoist Extension ChecklistAhmad RazaNo ratings yet
- ITR ELQ (Equipment)Document8 pagesITR ELQ (Equipment)mahmoudNo ratings yet
- HC172Document6 pagesHC172Dawn CasuncadNo ratings yet
- Work at Heights PermitDocument4 pagesWork at Heights PermitFerdinand M. TurbanosNo ratings yet
- StudentStudymet581161 4Document4 pagesStudentStudymet581161 4CM VendhenNo ratings yet
- F.841 - Certificate of Thorough Examination of Manlift - MEWP Rev.02Document2 pagesF.841 - Certificate of Thorough Examination of Manlift - MEWP Rev.02YasirNo ratings yet
- new india claim form 2Document2 pagesnew india claim form 2Ravi GoswamiNo ratings yet
- 89 Gas and Oilfield Safety Inspection ChecklistDocument14 pages89 Gas and Oilfield Safety Inspection Checklistdilip matalNo ratings yet
- Crane and Lifting PermitDocument10 pagesCrane and Lifting Permitron.farleyNo ratings yet
- Contractor Incident Report SystemDocument11 pagesContractor Incident Report SystemLen JganNo ratings yet
- Annual Fire Alarm Service ReportDocument10 pagesAnnual Fire Alarm Service ReportAnonymous utxGVB5VyNo ratings yet
- FC 4.1.22 - Mobile Drill Machine Daily ChecklistDocument1 pageFC 4.1.22 - Mobile Drill Machine Daily Checklistkhrayzie bhoneNo ratings yet
- Heavy Duty Equip Tech Stat DecDocument3 pagesHeavy Duty Equip Tech Stat DecAsif JavedNo ratings yet
- Safety Daily Site Checklist Mastoura co-SA-1-12Document12 pagesSafety Daily Site Checklist Mastoura co-SA-1-12LawrenceNo ratings yet
- Att Job Safety Assessment (Jsa) Rev F Dated 9-22-15Document2 pagesAtt Job Safety Assessment (Jsa) Rev F Dated 9-22-15Brandon Moore0% (1)
- Accident Reporting Form - V4Document2 pagesAccident Reporting Form - V4numair khanNo ratings yet
- Supervisor's Investigative Report Form and InsructionsDocument2 pagesSupervisor's Investigative Report Form and InsructionsRyan FlemingNo ratings yet
- Notice of Installation of A Boiler or Pressure VESSEL (An "Object")Document1 pageNotice of Installation of A Boiler or Pressure VESSEL (An "Object")Mohammed YcfssNo ratings yet
- ISS-1001-TMP-00007 New Starter &visitor Site Induction FormDocument3 pagesISS-1001-TMP-00007 New Starter &visitor Site Induction Formbubbles82No ratings yet
- Job Safety Analysis WorksheetDocument5 pagesJob Safety Analysis WorksheetDean Delon NanlohyNo ratings yet
- Mormugao Port Trust - Pass Section: (Application Form For Temporary Permits - Individuals / Vehicles)Document2 pagesMormugao Port Trust - Pass Section: (Application Form For Temporary Permits - Individuals / Vehicles)Vipin KrishnanNo ratings yet
- Identification 0varification 030520 SkaDocument14 pagesIdentification 0varification 030520 SkaRahul VishwakarmaNo ratings yet
- Gray Matter: Aviation Mechanics Most Frequently Asked QuestionsFrom EverandGray Matter: Aviation Mechanics Most Frequently Asked QuestionsNo ratings yet
- ITC.224.1 Assessment Answer-MITDocument4 pagesITC.224.1 Assessment Answer-MITNoel SumangaNo ratings yet
- Itc.326.1 00 - Cover Page-MitDocument3 pagesItc.326.1 00 - Cover Page-MitNoel SumangaNo ratings yet
- ITC.326.1 01 - Product Presentation-MITDocument29 pagesITC.326.1 01 - Product Presentation-MITNoel SumangaNo ratings yet
- Itc.326.1 00 - Cover Page-MitDocument3 pagesItc.326.1 00 - Cover Page-MitNoel SumangaNo ratings yet
- R.A. 7920Document21 pagesR.A. 7920Jezreel P. ImportanteNo ratings yet
- Ohms Law Formulas PDFDocument5 pagesOhms Law Formulas PDFAnonymous P1r2fMJ9No ratings yet
- Incident Report Form: Person Injured or Person Incurring DamageDocument3 pagesIncident Report Form: Person Injured or Person Incurring DamageNoel SumangaNo ratings yet
- Sample PPE Policies: InstructionsDocument9 pagesSample PPE Policies: InstructionsrejilkumarNo ratings yet
- Science 10 - Q1 - W5 - D2Document1 pageScience 10 - Q1 - W5 - D2zenaida a academiaNo ratings yet
- AICTE NoticeDocument1 pageAICTE NoticeThe WireNo ratings yet
- Prismatic Oil Level GaugeDocument2 pagesPrismatic Oil Level GaugevipulpanchotiyaNo ratings yet
- United States Government and PoliticsDocument21 pagesUnited States Government and PoliticsTony BuiNo ratings yet
- Chapter - 1 NetworksDocument61 pagesChapter - 1 NetworksSummiya JangdaNo ratings yet
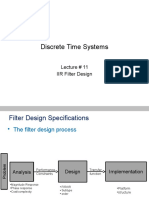
- DSP Lect 11 Iir DesignDocument50 pagesDSP Lect 11 Iir DesignSayyeda UmbereenNo ratings yet
- Mos Project Report-"Customer Satisfaction Survey: Telecom Sector"Document16 pagesMos Project Report-"Customer Satisfaction Survey: Telecom Sector"Kabejor Rahman Aka-NickyNo ratings yet
- Licence Acoknowledgement SlipDocument1 pageLicence Acoknowledgement SlipBicky ChoudhuryNo ratings yet
- Q12 KeyDocument3 pagesQ12 KeyMuhammad AbdullahNo ratings yet
- HyungJae Yang Sound Water EnvironmentDocument25 pagesHyungJae Yang Sound Water EnvironmentPepeNo ratings yet
- Test Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Document9 pagesTest Bank For Web Development and Design Foundations With Html5 6 e 6th Edition 0132783398Thomas White100% (23)
- 11608-Driving Women Fiction and PDFDocument240 pages11608-Driving Women Fiction and PDFAleksi KnuutilaNo ratings yet
- Ball ValveDocument12 pagesBall ValveIdabaNo ratings yet
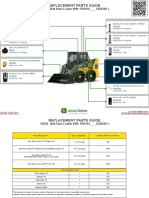
- 312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideDocument3 pages312GR Skid Steer Loader PIN 1T0312G G366358 Replacement Parts GuideNelson Andrade VelasquezNo ratings yet
- North American Free Trade Agreement: Prof. MakhmoorDocument15 pagesNorth American Free Trade Agreement: Prof. MakhmoorShikha ShuklaNo ratings yet
- Performance Appraisal at UFLEX Ltd.Document29 pagesPerformance Appraisal at UFLEX Ltd.Mohit MehraNo ratings yet
- 121-Ugong Issue 5.2 - FINAL - Doc - With Corrections-2nd RevisionDocument16 pages121-Ugong Issue 5.2 - FINAL - Doc - With Corrections-2nd RevisionMarq QoNo ratings yet
- Elevator PitchDocument2 pagesElevator PitchChandni SeelochanNo ratings yet
- Decentralization in the Philippines: A Review of Fiscal, Political and Service Delivery AspectsDocument13 pagesDecentralization in the Philippines: A Review of Fiscal, Political and Service Delivery AspectsDaniel Paulo MangampatNo ratings yet
- Nuclear Engineering and Design: Koki Hibi, Kunihiro Itoh, Kazuo Ikeda, Kenji KonashiDocument11 pagesNuclear Engineering and Design: Koki Hibi, Kunihiro Itoh, Kazuo Ikeda, Kenji KonashiWalid BadrNo ratings yet
- The Ultimate Experience With AvatradeDocument3 pagesThe Ultimate Experience With AvatradeAnonymous wk2GeJ8ERQNo ratings yet
- Qos/Qoe Techniques For Iptv Transmissions: June 2009Document9 pagesQos/Qoe Techniques For Iptv Transmissions: June 2009Hoàng Lam SơnNo ratings yet
- 638341140 (1)Document7 pages638341140 (1)Nishit BhanushaliNo ratings yet
- Combinational CircuitsDocument18 pagesCombinational CircuitsSalil TimalsinaNo ratings yet
- Seatwork 12 Analysis of Variance ANOVA Simple Linear RegressionDocument17 pagesSeatwork 12 Analysis of Variance ANOVA Simple Linear RegressionDanrey PasiliaoNo ratings yet
- Mobile Scaffold Inspection ChecklistDocument3 pagesMobile Scaffold Inspection Checklistanthony murphyNo ratings yet
- Razwan Iqbalcv1Document3 pagesRazwan Iqbalcv1razwaniqbalNo ratings yet
- The Threat Landscape Quiz ResultsDocument5 pagesThe Threat Landscape Quiz ResultsKaskusemail88 EmailNo ratings yet
- BSBPMG534 Task 2 - V2.4Document9 pagesBSBPMG534 Task 2 - V2.4Anoosha MazharNo ratings yet