You might also like
- Natural Cancer Remedies That WorkDocument48 pagesNatural Cancer Remedies That WorkAlessio Anam100% (1)
- Administering An Intramuscular InjectionDocument3 pagesAdministering An Intramuscular Injectionapi-26570979100% (4)
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Document289 pagesHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaNo ratings yet
- NAVLE - ReviewsDocument3 pagesNAVLE - ReviewsEvaldo Mamedes0% (1)
- CPG Management of Haemophilia 20191024 PDFDocument21 pagesCPG Management of Haemophilia 20191024 PDFwinnie yewNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Ovarian CancerDocument27 pagesOvarian CancerJohn Alcantara100% (1)
- CKD PathophysiologyDocument1 pageCKD Pathophysiologylloyd_santino67% (3)
- Pulmonary EmbolismDocument14 pagesPulmonary EmbolismMutaz Dredei100% (5)
- Geriatric Pharmacotherapy PDFDocument6 pagesGeriatric Pharmacotherapy PDFverry aswardsNo ratings yet
- The Poor Prognosis and Influencing Factors of HighDocument8 pagesThe Poor Prognosis and Influencing Factors of HighI Al WNo ratings yet
- Association Between D-Dimer Levels and Mortality in Patients With Coronavirus Disease 2019 (COVID-19) : A Systematic Review and Pooled AnalysisDocument7 pagesAssociation Between D-Dimer Levels and Mortality in Patients With Coronavirus Disease 2019 (COVID-19) : A Systematic Review and Pooled AnalysisRia GandaNo ratings yet
- Jurnal 2Document6 pagesJurnal 2fitri juliantiNo ratings yet
- Journal of Infection: Letter To The EditorDocument3 pagesJournal of Infection: Letter To The Editorjose steven garciaNo ratings yet
- Vitamin D Supplementation, COVID-19 and Disease Severity: A Meta-AnalysisDocument7 pagesVitamin D Supplementation, COVID-19 and Disease Severity: A Meta-AnalysisChairul LatiefNo ratings yet
- JMV 25961Document9 pagesJMV 25961damar soebandNo ratings yet
- Machine-Learning-Based COVID-19 Mortality Prediction Model and Identification of Patients at Low and High Risk of DyingDocument14 pagesMachine-Learning-Based COVID-19 Mortality Prediction Model and Identification of Patients at Low and High Risk of DyingMOBNo ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19Document6 pagesDiagnostic Utility of Clinical Laboratory Data Determinationsfor Patients With The Severe COVID 19junior rodriguesNo ratings yet
- JPM 12 01775 v2Document11 pagesJPM 12 01775 v2Cesare PaolinoNo ratings yet
- 10 1002@jmv 25819Document6 pages10 1002@jmv 25819Maya Angela LisalNo ratings yet
- JMV 26509Document12 pagesJMV 26509a27091No ratings yet
- Correlation of Chest Radiological Findings With Biochemical Markers On Oxygen Requirement in COVID 19 Patients A Retrospective AnalysisDocument11 pagesCorrelation of Chest Radiological Findings With Biochemical Markers On Oxygen Requirement in COVID 19 Patients A Retrospective AnalysisAthenaeum Scientific PublishersNo ratings yet
- Efficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisDocument5 pagesEfficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisJuan José Cardona GiraldoNo ratings yet
- Efficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisDocument21 pagesEfficacy of Various Treatment Modalities For nCOV-2019: A Systematic Review and Meta-AnalysisJuan José Cardona GiraldoNo ratings yet
- Covid and CancerDocument11 pagesCovid and Cancerriska silviaNo ratings yet
- 2022 - Factors Associated With Hospitalizations For Covid-19 in Patients With Rheumatoid Arthritis Data From The Reumacov Brazil RegistryDocument8 pages2022 - Factors Associated With Hospitalizations For Covid-19 in Patients With Rheumatoid Arthritis Data From The Reumacov Brazil RegistryGustavo ResendeNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument8 pagesDiabetes & Metabolic Syndrome: Clinical Research & Reviewslama rashedNo ratings yet
- Revisión Sistemática Sobre La Utilidad Pronóstica Del Dímero-D, Coagulación Intravascular Diseminada y Tratamiento Anticoagulante en Pacientes Graves Con COVID-19Document14 pagesRevisión Sistemática Sobre La Utilidad Pronóstica Del Dímero-D, Coagulación Intravascular Diseminada y Tratamiento Anticoagulante en Pacientes Graves Con COVID-19Brian ValenciaNo ratings yet
- Research Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 PatientsDocument10 pagesResearch Article: Machine Learning-Based Model To Predict The Disease Severity and Outcome in COVID-19 Patientsamin mohNo ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Document18 pagesDiagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Carla CANo ratings yet
- Research and Practice in Thrombosis and Haemostasis - 2022 - Zhang - How To Use and Report Data On D Dimer Testing in TheDocument2 pagesResearch and Practice in Thrombosis and Haemostasis - 2022 - Zhang - How To Use and Report Data On D Dimer Testing in ThetochtliNo ratings yet
- Deficiencia de Vitamina D y Sepsis PDFDocument8 pagesDeficiencia de Vitamina D y Sepsis PDFEšmęrąldą ŤôrôNo ratings yet
- Stroke in CovidDocument13 pagesStroke in CovidAbdul AzeezNo ratings yet
- Biomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-AnalysisDocument12 pagesBiomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-AnalysisPedro Luz da RosaNo ratings yet
- Correlations of CT Scan With High-Sensitivity C-ReDocument5 pagesCorrelations of CT Scan With High-Sensitivity C-ReAnthony ChristantoNo ratings yet
- Nomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsDocument12 pagesNomogram Model For Predicting The Risk of Multidrug-Resistant Bacteria Infection in Diabetic Foot PatientsMai BasionyNo ratings yet
- Development and Validation of A Nomogram Using On Admission Routine Laboratory Parameters To Predict In-Hospital Survival of Patients With COVID-19Document23 pagesDevelopment and Validation of A Nomogram Using On Admission Routine Laboratory Parameters To Predict In-Hospital Survival of Patients With COVID-19dariusNo ratings yet
- Alterations in CRP, D-Dimer and LDH Levels in Patients With Covid 19Document8 pagesAlterations in CRP, D-Dimer and LDH Levels in Patients With Covid 19Impact JournalsNo ratings yet
- Ahead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsDocument6 pagesAhead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsSana AbbasNo ratings yet
- Jurnal Soal DDocument15 pagesJurnal Soal DrianarahmadhanyNo ratings yet
- A Breif Study of Haematological Parameters in Covid 19Document5 pagesA Breif Study of Haematological Parameters in Covid 19IJAR JOURNALNo ratings yet
- Chakra - Factors Associated With Complications of C DiffDocument8 pagesChakra - Factors Associated With Complications of C DiffCherry SmileNo ratings yet
- Thrombosis Research: Full Length ArticleDocument7 pagesThrombosis Research: Full Length ArticleAugusto MáximoNo ratings yet
- Covid y CoagulaciónDocument6 pagesCovid y CoagulaciónMaría JoséNo ratings yet
- Amp B Vs Azoles Vs Echinocandins Comparation For Teratment of CandidiasisDocument13 pagesAmp B Vs Azoles Vs Echinocandins Comparation For Teratment of CandidiasisveliaberlianaNo ratings yet
- InternacionalDocument9 pagesInternacionalbryan ronaldNo ratings yet
- Journal Reading 1Document25 pagesJournal Reading 1tikaNo ratings yet
- RMV 2225Document18 pagesRMV 2225Iziza LunaskhiNo ratings yet
- 2020 08 03 20167361v1 FullDocument28 pages2020 08 03 20167361v1 FullNovel SaputraNo ratings yet
- Anticoagulant TreatmentDocument6 pagesAnticoagulant TreatmentMonica AngNo ratings yet
- Henry2020Document8 pagesHenry2020TisaNo ratings yet
- Journal of Medical Virology - 2021 - Demir - Vitamin D Deficiency Is Associated With COVID 19 Positivity and Severity ofDocument8 pagesJournal of Medical Virology - 2021 - Demir - Vitamin D Deficiency Is Associated With COVID 19 Positivity and Severity ofMiguel Díaz HidalgoNo ratings yet
- Sars-Cov-2 Positivity Rates Associated With Circulating 25-Hydroxyvitamin D LevelsDocument10 pagesSars-Cov-2 Positivity Rates Associated With Circulating 25-Hydroxyvitamin D Levelsnina purnamasariNo ratings yet
- 1 s2.0 S0924857920302211 MainDocument3 pages1 s2.0 S0924857920302211 MainYuniati ValentinaNo ratings yet
- Laboratory Findings of Libyan Patients With COVID-19 in Intensive Care UnitDocument6 pagesLaboratory Findings of Libyan Patients With COVID-19 in Intensive Care UnitMediterr J Pharm Pharm SciNo ratings yet
- Sars-Cov-2 Vaccine Effectiveness Against Infection, Symptomatic and Severe Covid-19: A Systematic Review and Meta-AnalysisDocument12 pagesSars-Cov-2 Vaccine Effectiveness Against Infection, Symptomatic and Severe Covid-19: A Systematic Review and Meta-AnalysisChengwustZhangNo ratings yet
- Correlation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive AnalysisDocument7 pagesCorrelation of Demographic Profile With Laboratory Parameters and Clinical Factors As Predictors of Covid-19 Severity: A Comprehensive Analysisindex PubNo ratings yet
- CALL Score PCP V1Document10 pagesCALL Score PCP V1Jose Emmanuel FranciaNo ratings yet
- Predictors of Mortality in Hospitalised Patients With COVID-19: A 1-Year Case-Control StudyDocument12 pagesPredictors of Mortality in Hospitalised Patients With COVID-19: A 1-Year Case-Control Studystardust.m002No ratings yet
- 1 s2.0 S0147956323002443 MainDocument8 pages1 s2.0 S0147956323002443 Mainfadilababyonggo99No ratings yet
- Critical Reviews in Oncology / Hematology: SciencedirectDocument9 pagesCritical Reviews in Oncology / Hematology: SciencedirectFCS CoordinaciónNo ratings yet
- Jurnal 7 TridaraDocument9 pagesJurnal 7 TridaraLuckyNawaNo ratings yet
- Genetic Analysis of Covid 19Document27 pagesGenetic Analysis of Covid 19Debabrata SahaNo ratings yet
- To Study The Correlation of CT Severity Score With Oxygen Saturation and Inflammatory Biomarkers in Patients With Covid - 19 InfectionDocument4 pagesTo Study The Correlation of CT Severity Score With Oxygen Saturation and Inflammatory Biomarkers in Patients With Covid - 19 InfectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Relationship of D-Dimer With Severity and Mortality in Sars-Cov-2 Patients: A Meta-AnalysisDocument6 pagesRelationship of D-Dimer With Severity and Mortality in Sars-Cov-2 Patients: A Meta-AnalysisDendyNo ratings yet
- Specific Features of The Hemostatic System in Covid-19Document4 pagesSpecific Features of The Hemostatic System in Covid-19Central Asian StudiesNo ratings yet
- Antibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center StudyDocument5 pagesAntibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center Studyاحمد عرفاتNo ratings yet
- The Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudyDocument10 pagesThe Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudygiovannaNo ratings yet
- Academic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredDocument14 pagesAcademic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredOnilis RiveraNo ratings yet
- An Embedded Earring Backing in The Tragus: Otoscopic ClinicDocument3 pagesAn Embedded Earring Backing in The Tragus: Otoscopic Clinicxoleoni97No ratings yet
- An Embedded Earring Backing in The Tragus: Otoscopic ClinicDocument3 pagesAn Embedded Earring Backing in The Tragus: Otoscopic Clinicxoleoni97No ratings yet
- Systematic Review and Meta-Analysis On The Value of Chest CT in The Diagnosis of Coronavirus Disease (COVID-19) : Sol ScientiaeDocument9 pagesSystematic Review and Meta-Analysis On The Value of Chest CT in The Diagnosis of Coronavirus Disease (COVID-19) : Sol Scientiaexoleoni97No ratings yet
- Kode ICD 10 THTDocument10 pagesKode ICD 10 THTAnung Setiawan0% (1)
- Systematic Review and Meta-Analysis On The Value of Chest CT in The Diagnosis of Coronavirus Disease (COVID-19) : Sol ScientiaeDocument9 pagesSystematic Review and Meta-Analysis On The Value of Chest CT in The Diagnosis of Coronavirus Disease (COVID-19) : Sol Scientiaexoleoni97No ratings yet
- Embedded Earrings Case ReportDocument2 pagesEmbedded Earrings Case Reportxoleoni97No ratings yet
- Scientific Paper CompilationDocument149 pagesScientific Paper Compilationxoleoni97No ratings yet
- An Embedded Earring Backing in The Tragus: Otoscopic ClinicDocument3 pagesAn Embedded Earring Backing in The Tragus: Otoscopic Clinicxoleoni97No ratings yet
- Christian 2014Document12 pagesChristian 2014xoleoni97No ratings yet
- Jurnal SkripsiDocument29 pagesJurnal SkripsiVivin Novitasari Ptr ZNNo ratings yet
- Content Outline PharmacotherapyDocument8 pagesContent Outline PharmacotherapyDina OncyNo ratings yet
- Vitamin D HandoutDocument2 pagesVitamin D Handoutapi-239305061No ratings yet
- Dysphagia: (Difficulty Swallowing)Document17 pagesDysphagia: (Difficulty Swallowing)radian nasutionNo ratings yet
- NCP For Pain - Rheumatoid ArthritisDocument5 pagesNCP For Pain - Rheumatoid Arthritisveorjan100% (1)
- Radial Artery Access For Peripheral Endovascular ProceduresDocument6 pagesRadial Artery Access For Peripheral Endovascular Proceduresvam buddhaNo ratings yet
- A Case of Sheehan's Syndrome: A Rare But Life - Threatening ComplicationDocument2 pagesA Case of Sheehan's Syndrome: A Rare But Life - Threatening ComplicationEditor IJTSRDNo ratings yet
- Tibia Shaft Fracture TreatmentDocument26 pagesTibia Shaft Fracture Treatmentgalih widodoNo ratings yet
- Drug Study ParacetamolDocument2 pagesDrug Study ParacetamolDannah BulliandayNo ratings yet
- SEPSIS OUTCOMESDocument6 pagesSEPSIS OUTCOMESIgnacio PNo ratings yet
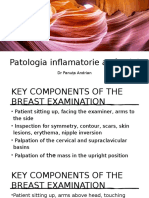
- Patologia Inflamatorie A Sânului: DR Panuța AndrianDocument31 pagesPatologia Inflamatorie A Sânului: DR Panuța AndrianPanuta AndrianNo ratings yet
- Pediatric Surgery Departement Statistics Alexandria EgyptDocument30 pagesPediatric Surgery Departement Statistics Alexandria Egypthayssam rashwanNo ratings yet
- Amber Coffey, M.S, R.T. (R) (T) (CT) (Arrt)Document2 pagesAmber Coffey, M.S, R.T. (R) (T) (CT) (Arrt)Amber CoffeyNo ratings yet
- Article WJPR 1504171685 PDFDocument7 pagesArticle WJPR 1504171685 PDFVenura TennakoonNo ratings yet
- Typhoid PerforationDocument3 pagesTyphoid PerforationSaryia JavedNo ratings yet
- Microneedling & Nanopore PresentationDocument58 pagesMicroneedling & Nanopore PresentationkatherineNo ratings yet
- 2003 - Most Commony Used DrugsDocument376 pages2003 - Most Commony Used DrugsasdNo ratings yet
- Factors Modifying Drug EffectsDocument47 pagesFactors Modifying Drug EffectsRiddhi Jain100% (1)
- Pharmacology of Disopyramide: Yosephine A. H. 020100058Document20 pagesPharmacology of Disopyramide: Yosephine A. H. 020100058zulfantri1983No ratings yet
- Abm-11-A Group 3 Term PaperDocument32 pagesAbm-11-A Group 3 Term PaperSalamah Senior SaipodenNo ratings yet
- Iavt05s1p1 PDFDocument6 pagesIavt05s1p1 PDFVashistmohan A.P.No ratings yet