You might also like
- Module 2 CANVAS NOTES HematopoiesisDocument6 pagesModule 2 CANVAS NOTES HematopoiesisMohammad MasacalNo ratings yet
- Hematology Module 2 and 3Document11 pagesHematology Module 2 and 3SEAN MELNOR LOSBAÑESNo ratings yet
- Hematology Trans - Module 3 & 4 - Hematopoiesis and Lineage Specific HematopoiesisDocument6 pagesHematology Trans - Module 3 & 4 - Hematopoiesis and Lineage Specific HematopoiesisFaye Kyla Heart ResuelloNo ratings yet
- Hematology 1 L2 Hematopoiesis LectureDocument4 pagesHematology 1 L2 Hematopoiesis LectureChelze Faith DizonNo ratings yet
- 3 HEMA HematopoiesisDocument9 pages3 HEMA HematopoiesisJohanna Rose Cobacha SalvediaNo ratings yet
- BSC Lecture Notes Semester 1Document7 pagesBSC Lecture Notes Semester 1satasha28No ratings yet
- CL1 HaemopoiesisDocument41 pagesCL1 HaemopoiesisSamuel George100% (1)
- He Ma To PoiesisDocument64 pagesHe Ma To Poiesismatthew deguzman100% (1)
- CLINPATH-01.Hematopoiesis & Morphology of Blood CellsDocument10 pagesCLINPATH-01.Hematopoiesis & Morphology of Blood CellsCharisse Angelica MacedaNo ratings yet
- Week 1 - HEMATOPOIESISDocument8 pagesWeek 1 - HEMATOPOIESISAcel Jone CayotNo ratings yet
- CHAPTER 2 HematopoiesisDocument7 pagesCHAPTER 2 HematopoiesisAMELIA DALE MARQUEZNo ratings yet
- HEMATOPOESISDocument71 pagesHEMATOPOESISHussenNo ratings yet
- Hema TransesDocument25 pagesHema TransesNikoh Anthony EwayanNo ratings yet
- Hematology 1 NotebookDocument29 pagesHematology 1 NotebookNikoh Anthony EwayanNo ratings yet
- HematologyDocument23 pagesHematologyWynlor AbarcaNo ratings yet
- Hematopoiesis (HEMA)Document12 pagesHematopoiesis (HEMA)April Lady Faith P. PaundogNo ratings yet
- 2 HaemopoiesisDocument50 pages2 HaemopoiesisWasana Mendis100% (2)
- LECTURE 2 - HEMATOPOIESIS and ERYTHROPOIESIS - 10 - 17 - 2020Document49 pagesLECTURE 2 - HEMATOPOIESIS and ERYTHROPOIESIS - 10 - 17 - 2020apoorva krishnagiriNo ratings yet
- Hematopoietic DevelopmentDocument6 pagesHematopoietic DevelopmentSea ClestNo ratings yet
- Development of Blood Cells 2019Document31 pagesDevelopment of Blood Cells 2019Muhammad Anas Abbal100% (1)
- AFIP Manual New HaemDocument76 pagesAFIP Manual New HaemDr.A SHAHID SiddiquiNo ratings yet
- Blood Formation LectureDocument24 pagesBlood Formation Lecturehassan aryaniNo ratings yet
- Hematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofDocument12 pagesHematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofRajender ArutlaNo ratings yet
- Exercise 5 HematopoiesisDocument11 pagesExercise 5 HematopoiesisAngela AninangNo ratings yet
- HematopoeisisDocument16 pagesHematopoeisisPauline SalvadorNo ratings yet
- Hematopoiesis PDFDocument10 pagesHematopoiesis PDFJezzah Mae CañeteNo ratings yet
- Lecture 3 (1) HaematopoeisisDocument20 pagesLecture 3 (1) Haematopoeisismaxwell amponsahNo ratings yet
- Stages and Phases of HematopoeisisDocument2 pagesStages and Phases of HematopoeisisDanica Barcebal100% (4)
- Lym, Throm, GranuDocument12 pagesLym, Throm, Granumaxwell amponsahNo ratings yet
- Hematopoiesis ErythropoiesisDocument8 pagesHematopoiesis ErythropoiesisASHLEY ALEXIS GUEVARRANo ratings yet
- Introduction To Haematology and HemopoiesisDocument30 pagesIntroduction To Haematology and HemopoiesisOROKE JOHN EJENo ratings yet
- Hematopoiesis New 161214142246Document29 pagesHematopoiesis New 161214142246Vikram KumarNo ratings yet
- Primary and Secondary Lymphoid Organs - Aditi SinghDocument50 pagesPrimary and Secondary Lymphoid Organs - Aditi SinghEunice PalloganNo ratings yet
- Blood SciencesDocument47 pagesBlood Sciencescaroline vaughanNo ratings yet
- Bone Marrow and Hematopoiesis - 2Document7 pagesBone Marrow and Hematopoiesis - 2Sharan MurugaboopathyNo ratings yet
- Semeiology of Hematopoietic SystemDocument18 pagesSemeiology of Hematopoietic SystemIvanNo ratings yet
- Heamtopoises ReviewerDocument17 pagesHeamtopoises ReviewerClyde BaltazarNo ratings yet
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- Ha Ema To PoiesisDocument38 pagesHa Ema To PoiesisEmma Joel OtaiNo ratings yet
- Haematopoitik System: Prof - Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked - SPPKDocument43 pagesHaematopoitik System: Prof - Dr. Adi Koesoema Aman SPPK (KH) - Dr. Malayana Nasution Mked - SPPKrubyniNo ratings yet
- HematopoiesisDocument5 pagesHematopoiesisFuture TrekingNo ratings yet
- HaematopoiesisDocument4 pagesHaematopoiesisGerardLum100% (1)
- H E M A T O P O I E S I S (Rodaks, Turgeon, and PPT) 11Document4 pagesH E M A T O P O I E S I S (Rodaks, Turgeon, and PPT) 11Kristin SoquilloNo ratings yet
- Haematopoiesis: DR Rosline Hassan Hematology Department School of Medical Sciences Universiti Sains MalaysiaDocument46 pagesHaematopoiesis: DR Rosline Hassan Hematology Department School of Medical Sciences Universiti Sains Malaysialow_sernNo ratings yet
- Hematology 1 NotesDocument40 pagesHematology 1 NotesAyessa SheinleeNo ratings yet
- Erythropoiesis: Presented by DR Etu-Efeotor T. PDocument88 pagesErythropoiesis: Presented by DR Etu-Efeotor T. PPrincewill SeiyefaNo ratings yet
- Hematopoeitic System& Blood, KBK 2015 LDLDocument80 pagesHematopoeitic System& Blood, KBK 2015 LDLgita dwi ananda100% (1)
- Hema Report PDFDocument25 pagesHema Report PDFdaliaNo ratings yet
- Hematopoiesis Reading NotesDocument7 pagesHematopoiesis Reading NotesMemeowwNo ratings yet
- Hematopoeitic System: Alya Amila Fitrie Lokot Donna LubisDocument80 pagesHematopoeitic System: Alya Amila Fitrie Lokot Donna LubisrubyniNo ratings yet
- Normal HematopoesiseDocument35 pagesNormal HematopoesisesaketNo ratings yet
- 2 - Introduction To Hematopoiesis and RBC ProductionDocument71 pages2 - Introduction To Hematopoiesis and RBC ProductionClaire GonoNo ratings yet
- HEMATOLOGYDocument5 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- Dr. Waluyo Rudiyanto, M.KesDocument50 pagesDr. Waluyo Rudiyanto, M.KesAsiatiNo ratings yet
- HEMATOPOIESISDocument65 pagesHEMATOPOIESISDian Artileristiana50% (2)
- Here, Only 1 Few Stages Undergo Subdivision (Sabi Ni Maam)Document6 pagesHere, Only 1 Few Stages Undergo Subdivision (Sabi Ni Maam)Jaenie Grace AliganNo ratings yet
- TRANS PPT TOPIC MegakaryopoeisisDocument5 pagesTRANS PPT TOPIC MegakaryopoeisisPaul LesterNo ratings yet
- ErythropoiesisDocument51 pagesErythropoiesisKevin Leo100% (1)
- HEMA-1 Up To PG 30.-1-31Document31 pagesHEMA-1 Up To PG 30.-1-31Angela ReyesNo ratings yet
- Hema DagdagDocument1 pageHema DagdagAngela ReyesNo ratings yet
- MYCODocument59 pagesMYCOAngela ReyesNo ratings yet
- Tumor Markers: Blood Group AntigenDocument5 pagesTumor Markers: Blood Group AntigenAngela ReyesNo ratings yet
- Hema 2Document35 pagesHema 2Angela ReyesNo ratings yet
- Pedigree Analysis WorksheetDocument3 pagesPedigree Analysis WorksheetAngela ReyesNo ratings yet
- Finals - VirologyDocument14 pagesFinals - VirologyAngela ReyesNo ratings yet
- Ilovepdf MergedDocument31 pagesIlovepdf MergedAngela ReyesNo ratings yet
- Aubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityDocument38 pagesAubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityAngela ReyesNo ratings yet
- Urine Sediment ConstituentsDocument12 pagesUrine Sediment ConstituentsAngela ReyesNo ratings yet
- Blood Bank (2 Week) : Antibody ScreensDocument5 pagesBlood Bank (2 Week) : Antibody ScreensAngela ReyesNo ratings yet
- Ilovepdf MergedDocument56 pagesIlovepdf MergedAngela ReyesNo ratings yet
- 5TH Week Hematocrit DeterminationDocument24 pages5TH Week Hematocrit DeterminationAngela ReyesNo ratings yet
- 1 Hema LecDocument5 pages1 Hema LecAngela ReyesNo ratings yet
- Myco LQDocument37 pagesMyco LQAngela ReyesNo ratings yet
- Coagulation Screening Procedures:: RD THDocument2 pagesCoagulation Screening Procedures:: RD THAngela ReyesNo ratings yet
- Midterms - MycologyDocument17 pagesMidterms - MycologyAngela ReyesNo ratings yet
- Microbiology: T. VaginalisDocument78 pagesMicrobiology: T. VaginalisAngela ReyesNo ratings yet
- Finals - ImmunohematologyDocument20 pagesFinals - ImmunohematologyAngela ReyesNo ratings yet
- Phagocyte System.: Innate/non-Specific Immune SystemDocument6 pagesPhagocyte System.: Innate/non-Specific Immune SystemAngela ReyesNo ratings yet
- 1 Hema LecDocument5 pages1 Hema LecAngela ReyesNo ratings yet
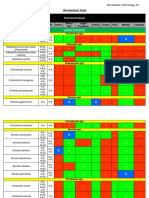
- Biochemical Tests: JAPAY, Princess Agatha Mei R. BS Medical Technology 3ADocument5 pagesBiochemical Tests: JAPAY, Princess Agatha Mei R. BS Medical Technology 3AAngela ReyesNo ratings yet
- Blue. 1 or 2 HoursDocument5 pagesBlue. 1 or 2 HoursAngela ReyesNo ratings yet
- Cclec MidtermsDocument65 pagesCclec MidtermsAngela ReyesNo ratings yet
- Biochem Test 1.2Document9 pagesBiochem Test 1.2Angela ReyesNo ratings yet
- Histopath Lec (Module 2) : Cellular Adaptations, Cellular Injury and Cell DeathDocument5 pagesHistopath Lec (Module 2) : Cellular Adaptations, Cellular Injury and Cell DeathAngela ReyesNo ratings yet
- Histopath Lec (Module 1) : Iintroduction To PathologyDocument17 pagesHistopath Lec (Module 1) : Iintroduction To PathologyAngela ReyesNo ratings yet
- Immuno Sero CompleteDocument33 pagesImmuno Sero CompleteAngela ReyesNo ratings yet
- BLOOD COLLECTION Part 1 Hema LabDocument7 pagesBLOOD COLLECTION Part 1 Hema LabAngela ReyesNo ratings yet
- Histopath Lab (Module 2) : Receiving, Accessioning and Gross Examination of Tissue SamplesDocument5 pagesHistopath Lab (Module 2) : Receiving, Accessioning and Gross Examination of Tissue SamplesAngela ReyesNo ratings yet
- Contemporary Strategic ManagementDocument2 pagesContemporary Strategic ManagementZee Dee100% (1)
- Ultracold Atoms SlidesDocument49 pagesUltracold Atoms SlideslaubbaumNo ratings yet
- Isi Rumen SBG Subtitusi HijauanDocument3 pagesIsi Rumen SBG Subtitusi HijauanBagas ImamsyahNo ratings yet
- Saiva Dharma ShastrasDocument379 pagesSaiva Dharma ShastrasfunnybizNo ratings yet
- Circular ConvolutionDocument3 pagesCircular Convolutionseeksudhanshu1No ratings yet
- Industrial ExperienceDocument30 pagesIndustrial ExperienceThe GridLockNo ratings yet
- World War II D-Day Invasion by SlidesgoDocument55 pagesWorld War II D-Day Invasion by SlidesgoPreston SandsNo ratings yet
- COK - Training PlanDocument22 pagesCOK - Training PlanralphNo ratings yet
- Hockney-Falco Thesis: 1 Setup of The 2001 PublicationDocument6 pagesHockney-Falco Thesis: 1 Setup of The 2001 PublicationKurayami ReijiNo ratings yet
- Research FinalDocument55 pagesResearch Finalkieferdem071908No ratings yet
- CFD Turbina Michell BankiDocument11 pagesCFD Turbina Michell BankiOscar Choque JaqquehuaNo ratings yet
- AIIMS 2015 Solved PaperDocument436 pagesAIIMS 2015 Solved PaperSurya TejaNo ratings yet
- 2Document8 pages2Eduardo Antonio Comaru Gouveia75% (4)
- Coaxial Cable Attenuation ChartDocument6 pagesCoaxial Cable Attenuation ChartNam PhamNo ratings yet
- The Checkmate Patterns Manual: The Ultimate Guide To Winning in ChessDocument30 pagesThe Checkmate Patterns Manual: The Ultimate Guide To Winning in ChessDusen VanNo ratings yet
- ISA InTech Journal - April 2021Document50 pagesISA InTech Journal - April 2021Ike EdmondNo ratings yet
- Culture 2007 2013 Projects Overview 2018-03-18Document133 pagesCulture 2007 2013 Projects Overview 2018-03-18PontesDeboraNo ratings yet
- Detail Design Drawings: OCTOBER., 2017 Date Span Carriage WayDocument26 pagesDetail Design Drawings: OCTOBER., 2017 Date Span Carriage WayManvendra NigamNo ratings yet
- 19 Dark PPT TemplateDocument15 pages19 Dark PPT TemplateKurt W. DelleraNo ratings yet
- Importance of Skill Based Education-2994Document5 pagesImportance of Skill Based Education-2994João Neto0% (1)
- Niveshdaily: From Research DeskDocument53 pagesNiveshdaily: From Research DeskADNo ratings yet
- Bcom (HNRS) Project Final Year University of Calcutta (2018)Document50 pagesBcom (HNRS) Project Final Year University of Calcutta (2018)Balaji100% (1)
- W.C. Hicks Appliances: Client Name SKU Item Name Delivery Price Total DueDocument2 pagesW.C. Hicks Appliances: Client Name SKU Item Name Delivery Price Total DueParth PatelNo ratings yet
- Grammar and Vocabulary TestDocument5 pagesGrammar and Vocabulary TestLeonora ConejosNo ratings yet
- Ultra ConductorsDocument28 pagesUltra ConductorsAnu Kp50% (8)
- Pathogenic Escherichia Coli Associated With DiarrheaDocument7 pagesPathogenic Escherichia Coli Associated With DiarrheaSiti Fatimah RadNo ratings yet
- Gis Data Creation in Bih: Digital Topographic Maps For Bosnia and HerzegovinaDocument9 pagesGis Data Creation in Bih: Digital Topographic Maps For Bosnia and HerzegovinaGrantNo ratings yet
- Mcdaniel Tanilla Civilian Resume Complete v1Document3 pagesMcdaniel Tanilla Civilian Resume Complete v1api-246751844No ratings yet
- Sample REVISION QUESTION BANK. ACCA Paper F5 PERFORMANCE MANAGEMENTDocument43 pagesSample REVISION QUESTION BANK. ACCA Paper F5 PERFORMANCE MANAGEMENTAbayneh Assefa75% (4)
- De Thi Hoc Ki 1 Lop 11 Mon Tieng Anh Co File Nghe Nam 2020Document11 pagesDe Thi Hoc Ki 1 Lop 11 Mon Tieng Anh Co File Nghe Nam 2020HiềnNo ratings yet