You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Master Rotation Plan - Final-F B. SC NursingDocument10 pagesMaster Rotation Plan - Final-F B. SC NursingRumela ChakrabortyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Observational Report ON: Cardiac Catheterization LaboratoryDocument12 pagesObservational Report ON: Cardiac Catheterization LaboratoryRumela Chakraborty100% (2)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Arterial Blood Gas (Abg) Analysis: Submitted ToDocument5 pagesArterial Blood Gas (Abg) Analysis: Submitted ToRumela ChakrabortyNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 2 FinalDisaster Nursing 1707Document17 pages2 FinalDisaster Nursing 1707Rumela ChakrabortyNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 3 Final Lymphoma and MyelomaDocument16 pages3 Final Lymphoma and MyelomaRumela Chakraborty100% (1)
- NHP Jugal KishoreDocument1,015 pagesNHP Jugal KishoreStefiSundaranNo ratings yet
- UPHC Guideliens - UpdatedDocument34 pagesUPHC Guideliens - Updatedradhe sharmaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- NLC Updated Images For FMG Dec 2021 FinalDocument481 pagesNLC Updated Images For FMG Dec 2021 Finalshivangi khatriNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- IqraDocument71 pagesIqraShenaya singhNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- SPM HAQs 1ST EdDocument46 pagesSPM HAQs 1ST Edranjanavnish142No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Health Programme (Ayurveda Library - Dr. Vivek Tiwari) 2Document24 pagesHealth Programme (Ayurveda Library - Dr. Vivek Tiwari) 2NinnnNo ratings yet
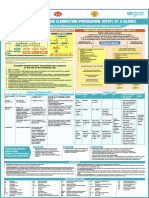
- NTEP at A Glance - Comprehensive Clinical Management Protocol For TBDocument1 pageNTEP at A Glance - Comprehensive Clinical Management Protocol For TBNael NajeebNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Uttarkhand & JK Adv Online (Agra)Document8 pagesUttarkhand & JK Adv Online (Agra)sipuns827No ratings yet
- Job Responsibilities of Health Workers (Male & Female)Document9 pagesJob Responsibilities of Health Workers (Male & Female)Kailash NagarNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Primary Health Centre Organization and FunctionsDocument9 pagesPrimary Health Centre Organization and FunctionsKailash NagarNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- RNTCPDocument46 pagesRNTCPdarshitkotadiya2553No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Tuberculosis (Part 2) : DR Ruchi Dua Associate Professor (MD, DNB) Department of Pulmonary Medicine Aiims RishikeshDocument36 pagesTuberculosis (Part 2) : DR Ruchi Dua Associate Professor (MD, DNB) Department of Pulmonary Medicine Aiims RishikeshMohammed HammedNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- ASHA Incentive Master Claim Form Draft ENGLISH PDFDocument8 pagesASHA Incentive Master Claim Form Draft ENGLISH PDFPushpa GopiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Annexure III.h: Total Male Female TS/TG Male Female TS/TGDocument9 pagesAnnexure III.h: Total Male Female TS/TG Male Female TS/TGTanishk MahereNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Krishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectDocument38 pagesKrishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectchahatpuriNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Operation Dr. Satya Sundar Mohapatra, MBA Health Care Services, Contact: 9437184147Document3 pagesOperation Dr. Satya Sundar Mohapatra, MBA Health Care Services, Contact: 9437184147SatyaMohapatraNo ratings yet
- Textbook of Community Medicine PreventivDocument27 pagesTextbook of Community Medicine Preventivtasneem faizaNo ratings yet
- 1001987548link of Advt With Inductus WebsiteDocument9 pages1001987548link of Advt With Inductus WebsiteJuhi NeogiNo ratings yet
- TB Management Final1Document23 pagesTB Management Final1Aanchal JainNo ratings yet
- Problems On EpidemiologyDocument146 pagesProblems On EpidemiologyAnnie HadassahNo ratings yet
- 28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarDocument29 pages28.04.2021 NTEP - RNTCP Dr. Tanuja PattankarTanuja PattankarNo ratings yet
- Tuberculosis DrugsDocument136 pagesTuberculosis DrugsSyed Gulshan NaqviNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Chapter 5 - National Health Programme PDFDocument26 pagesChapter 5 - National Health Programme PDFPratik LengureNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Himachal Pradesh Current Affairs 2020 by AffairsCloudDocument37 pagesHimachal Pradesh Current Affairs 2020 by AffairsCloudMohit ChoudharyNo ratings yet
- Hospital Manual - CRHSPDocument146 pagesHospital Manual - CRHSPsumeshsomanNo ratings yet
- M&E FrameworkDocument64 pagesM&E FrameworklauraNo ratings yet
- Tuberculosis Isolates From Delhi Using Genotype Mtbdrplus AssayDocument7 pagesTuberculosis Isolates From Delhi Using Genotype Mtbdrplus AssayrehanaNo ratings yet
- 692 693 PDFDocument2 pages692 693 PDFSaumilNo ratings yet
- Ni-Kshay Informant DBTDocument29 pagesNi-Kshay Informant DBTUtkarshaTiwariNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)