You might also like
- Andrews' Diseases of The Skin 1e 2018Document578 pagesAndrews' Diseases of The Skin 1e 2018Ivanildo100% (1)
- Anatomy - Head and Neck Table of NervesDocument11 pagesAnatomy - Head and Neck Table of NervesIke Ononiwu100% (3)
- Identify The Boundaries of The Infratemporal FossaDocument7 pagesIdentify The Boundaries of The Infratemporal FossaHARSHDESAI56929640No ratings yet
- Hypothyroid SymptomsDocument19 pagesHypothyroid Symptomsfatima110100% (2)
- Bipolar DisordersDocument63 pagesBipolar DisorderselvinegunawanNo ratings yet
- Clinical Collection 2017 2018Document1,602 pagesClinical Collection 2017 2018Laura GranadosNo ratings yet
- Differential Diagnosis in Dermatology Fourth Edition: Richard Ashton, Barbara Leppard and Hywel CooperDocument30 pagesDifferential Diagnosis in Dermatology Fourth Edition: Richard Ashton, Barbara Leppard and Hywel CooperAussie Aulia100% (1)
- Pharynx: Upper Part: Widest - 3.5 CM, Non-Collapsible Middle Part: Narrow Lower End: Narrowest Part of GITDocument5 pagesPharynx: Upper Part: Widest - 3.5 CM, Non-Collapsible Middle Part: Narrow Lower End: Narrowest Part of GITdrpnnreddyNo ratings yet
- Dr. Khalid - S Explanation of 1700 MCQ1Document683 pagesDr. Khalid - S Explanation of 1700 MCQ1heba100% (1)
- PHYSICAL FITNESS and Self Testing ActivitiesDocument13 pagesPHYSICAL FITNESS and Self Testing ActivitiesSydney VersozaNo ratings yet
- The Patient History An Evidence-Based Approach To Differential DiagnosisDocument4 pagesThe Patient History An Evidence-Based Approach To Differential DiagnosisISAYK13% (8)
- MRCPCH 1aDocument21 pagesMRCPCH 1aLoai El100% (1)
- English 2nd Year NotesDocument18 pagesEnglish 2nd Year NotesMuhammad Irfan Khan100% (4)
- Lower LimbsDocument21 pagesLower Limbsauckey171717No ratings yet
- 8 Pharynx Larynx and Nasal CavityDocument13 pages8 Pharynx Larynx and Nasal CavityAmbg GhalyNo ratings yet
- Nose PDFDocument6 pagesNose PDFNiranjanPandeyNo ratings yet
- NotesDocument5 pagesNotesGrantNo ratings yet
- La Faringe. SNM Del Nervio Glosofaríngeo. Plexo FaríngeoDocument24 pagesLa Faringe. SNM Del Nervio Glosofaríngeo. Plexo FaríngeocristinaNo ratings yet
- Cockroach - Endgame Handwritten and SupernotesDocument27 pagesCockroach - Endgame Handwritten and Supernotesmansilamba1006No ratings yet
- Visual Pathway LesionDocument9 pagesVisual Pathway LesionMsd KishorNo ratings yet
- Anatomy AssignmentDocument6 pagesAnatomy AssignmentAyush GuptaNo ratings yet
- Bimbingan 7Document4 pagesBimbingan 7sean 102018039No ratings yet
- Lung FeaturesDocument1 pageLung FeaturesAmrinder MaanNo ratings yet
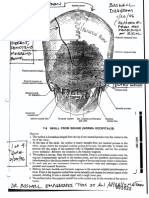
- 7-9 Skull From Behind (Norma Occipitalis)Document4 pages7-9 Skull From Behind (Norma Occipitalis)Zohaib Ur RahmanNo ratings yet
- Embryo 1805Document12 pagesEmbryo 1805NANDINI RATTANNo ratings yet
- Parfitt:) : TryacheaDocument15 pagesParfitt:) : TryacheaJaisri MNo ratings yet
- Parfitt:) : TryacheaDocument15 pagesParfitt:) : TryacheaDhinesh KumarNo ratings yet
- FinalsDocument1 pageFinalsnaljaber1501No ratings yet
- Lower Limb by DR Ashwini SirDocument13 pagesLower Limb by DR Ashwini Sirvani1234guptaNo ratings yet
- Gross AnatomyDocument4 pagesGross AnatomyMacho Inglish ManNo ratings yet
- EarthwormDocument24 pagesEarthworm10306anshkumarNo ratings yet
- Respiratory HistologyDocument2 pagesRespiratory Histologyemptech3No ratings yet
- 10 Respiratory System 2Document120 pages10 Respiratory System 2rosalyn gaboniNo ratings yet
- Biology 3Document1 pageBiology 3KacperCoghenNo ratings yet
- EmbryologyDocument1 pageEmbryologyprasannaipad324No ratings yet
- Basics of Biology: Professor Vishal Trivedi Department of Biosciences and Bioengineering, IIT Guwahati, Assam, IndiaDocument32 pagesBasics of Biology: Professor Vishal Trivedi Department of Biosciences and Bioengineering, IIT Guwahati, Assam, IndiaAKKARSHANA P BIOTECH-2018 BATCHNo ratings yet
- Cardiopulmo NotesDocument8 pagesCardiopulmo NotessegotierjudiNo ratings yet
- Humerus (Bone and Attachments) Flow ChartDocument4 pagesHumerus (Bone and Attachments) Flow ChartLove GuruNo ratings yet
- Anat102a Notes FinalsDocument12 pagesAnat102a Notes FinalsJianne PulidoNo ratings yet
- Module # Respi TransDocument4 pagesModule # Respi TransLara VanessNo ratings yet
- Praktikum HistologiDocument20 pagesPraktikum Histologidanial habriNo ratings yet
- Anatomy 2Document1 pageAnatomy 2Casey Rae YanoNo ratings yet
- Untitled NotebookDocument10 pagesUntitled NotebookprinceNo ratings yet
- Digestive SystemDocument2 pagesDigestive SystemRANGSINEE SUWANNASUKNo ratings yet
- Entomology: Harsh HemananiDocument17 pagesEntomology: Harsh HemananiThe DeofelNo ratings yet
- Infratemporalfossa PpsDocument7 pagesInfratemporalfossa PpsНемосјановић ЋудмилаNo ratings yet
- การบ้าน Flap Coverage Lower LegsDocument4 pagesการบ้าน Flap Coverage Lower Legsภควัต วังทะพันธ์No ratings yet
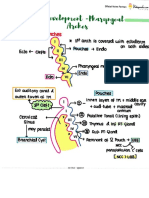
- Pharyngeal ArchesDocument2 pagesPharyngeal Archesspeedy.catNo ratings yet
- Anatomi HidungDocument28 pagesAnatomi HidungferyantoachmadNo ratings yet
- Cranial NervesDocument1 pageCranial NervesFluffy_iceNo ratings yet
- FrogDocument65 pagesFrognarayan sahNo ratings yet
- Crustacea (Rakovi) : Insecta MyriapodaDocument37 pagesCrustacea (Rakovi) : Insecta MyriapodadjokalotricNo ratings yet
- ATLSDocument29 pagesATLSmasriemarshalyNo ratings yet
- SF1-Lecture-01 - Body Fluids and Circulation - NotesDocument7 pagesSF1-Lecture-01 - Body Fluids and Circulation - Notesdisha shuklaNo ratings yet
- Pineal Choroid Plexus Habenular Dural: Physiologic CalcificationDocument6 pagesPineal Choroid Plexus Habenular Dural: Physiologic CalcificationLpsuedjNo ratings yet
- Infra Temporal FossaDocument7 pagesInfra Temporal FossaНемосјановић ЋудмилаNo ratings yet
- ANPH Wk13 - Pulmonary SystemDocument12 pagesANPH Wk13 - Pulmonary SystemSin I GangNo ratings yet
- Excretory Products and Their EliminaationDocument51 pagesExcretory Products and Their Eliminaationmaitreyivm21No ratings yet
- Species Tab.Document13 pagesSpecies Tab.Kobee BacolodNo ratings yet
- True Oral CavityDocument3 pagesTrue Oral CavityHanneke Du PlessisNo ratings yet
- Anatomy Lower Limb by DR AzamDocument19 pagesAnatomy Lower Limb by DR AzamroulprayashNo ratings yet
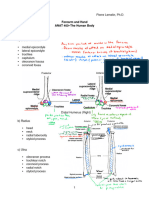
- Forearm and HandDocument8 pagesForearm and Handteam.tell.0qNo ratings yet
- Quiz ReviewerDocument8 pagesQuiz ReviewerCai PascualNo ratings yet
- Gram Negative Bacilli - RespiratoryDocument4 pagesGram Negative Bacilli - RespiratoryrefuapalackyNo ratings yet
- Anatomy Final RevesionDocument2 pagesAnatomy Final Revesiondhuhamed2022No ratings yet
- Respiratory System With HighlightsDocument90 pagesRespiratory System With HighlightsReinand Joseff ServanoNo ratings yet
- C-5 Digestive System II PDFDocument33 pagesC-5 Digestive System II PDFHarsh PatelNo ratings yet
- Plant FDocument5 pagesPlant Fny neNo ratings yet
- AnatomyDocument26 pagesAnatomyAvinashNo ratings yet
- Screenshot 2020-01-12 at 8.27.45 PMDocument1 pageScreenshot 2020-01-12 at 8.27.45 PMIntisar AL SenaniNo ratings yet
- Heartfailurelecture 140122113443 Phpapp02Document80 pagesHeartfailurelecture 140122113443 Phpapp02Ngoc-Suong LeNo ratings yet
- Clinical Case 03-2019 by SlidesgoDocument42 pagesClinical Case 03-2019 by SlidesgoMark Daniel RuizNo ratings yet
- Clinical Correlation p2Document2 pagesClinical Correlation p2Intisar AL SenaniNo ratings yet
- Carpal TunnelDocument7 pagesCarpal TunnelIntisar AL SenaniNo ratings yet
- Clinical Correlation p2Document2 pagesClinical Correlation p2Intisar AL SenaniNo ratings yet
- Carpal TunnelDocument7 pagesCarpal TunnelIntisar AL SenaniNo ratings yet
- ALT (Alanine Aminotransferase) Test - Purpose, Procedure, and Results PDFDocument5 pagesALT (Alanine Aminotransferase) Test - Purpose, Procedure, and Results PDFMARIUS BACIUNo ratings yet
- Cristian Zanartu, MD Joins New York Cancer & Blood SpecialistsDocument3 pagesCristian Zanartu, MD Joins New York Cancer & Blood SpecialistsPR.comNo ratings yet
- Dermatitis Atopica Niños - Ingles PDFDocument10 pagesDermatitis Atopica Niños - Ingles PDFESTEPHANY PAMELA GAMBINI ACOSTANo ratings yet
- Acute On Chronic Liver FailureDocument7 pagesAcute On Chronic Liver FailureDendyNo ratings yet
- Oral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeDocument7 pagesOral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeSnowNo ratings yet
- EscitalopramDocument1 pageEscitalopramRicky Ramos Jr.No ratings yet
- Rinitis AlergyDocument24 pagesRinitis AlergyroatfatchuriNo ratings yet
- 2 Abdomen Checklist 1Document3 pages2 Abdomen Checklist 1Angela DancelNo ratings yet
- Mofettes - English PresentationDocument1 pageMofettes - English Presentationhotel montanaNo ratings yet
- Oxford English For Careers - Medicine1 .Unit 2Document5 pagesOxford English For Careers - Medicine1 .Unit 2Linda JamburiaNo ratings yet
- Ricardo Padilla Perez v. Secretary of Health & Human Services, 985 F.2d 552, 1st Cir. (1993)Document10 pagesRicardo Padilla Perez v. Secretary of Health & Human Services, 985 F.2d 552, 1st Cir. (1993)Scribd Government DocsNo ratings yet
- PericarditisDocument3 pagesPericarditisKhalid Mahmud Arifin0% (1)
- Ncma 219 Finals CompleteDocument70 pagesNcma 219 Finals CompleteKENSEY MOORE EBROLENo ratings yet
- Cryptosporidiosis in Ruminants: Update and Current Therapeutic ApproachesDocument8 pagesCryptosporidiosis in Ruminants: Update and Current Therapeutic ApproachesDrivailaNo ratings yet
- Thesis Statement Examples Alzheimers DiseaseDocument6 pagesThesis Statement Examples Alzheimers DiseaseJulie Davis100% (2)
- Benefits From OkraDocument1 pageBenefits From OkranasirfahimNo ratings yet
- HL - PH - 001Document2 pagesHL - PH - 001stepuptoblockNo ratings yet
- Summary History of Nursing - Ersa Salia 19020Document2 pagesSummary History of Nursing - Ersa Salia 19020Ersa SaliaNo ratings yet
- Annisya Handini 1Document15 pagesAnnisya Handini 1Hafidh Alyza RNo ratings yet
- BacteriologyDocument14 pagesBacteriologysilcmtgNo ratings yet