You might also like
- Family Health Assessment FormDocument3 pagesFamily Health Assessment FormMitchTalledo100% (2)
- Family Assessment GuideDocument5 pagesFamily Assessment GuideAngelica Jane GomezNo ratings yet
- Virginia School Entrance Health FormDocument4 pagesVirginia School Entrance Health Formapi-245886452No ratings yet
- People's participation in health care through community organizingDocument1 pagePeople's participation in health care through community organizingRickNo ratings yet
- Identifying Community Health ProblemsDocument4 pagesIdentifying Community Health ProblemsEmvie Loyd Pagunsan-ItableNo ratings yet
- Community HealthDocument52 pagesCommunity Healthshangsyndrome100% (2)
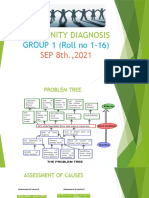
- COMMUNITY DIAGNOSIS Group 1Document11 pagesCOMMUNITY DIAGNOSIS Group 1Sumit GavitNo ratings yet
- Family Health Assessment FormDocument8 pagesFamily Health Assessment FormKevin Llorente50% (2)
- BMJ Case Reports Standard Template 1Document9 pagesBMJ Case Reports Standard Template 1Anisa Dwi FathinasariNo ratings yet
- FOH-25 Tuberculosis Screening (M.25)Document1 pageFOH-25 Tuberculosis Screening (M.25)Maria CabañasNo ratings yet
- Family Assessment Guide: Family Member'S ChartDocument6 pagesFamily Assessment Guide: Family Member'S ChartJULIANNE BAYHONNo ratings yet
- CHN CHP 7Document5 pagesCHN CHP 7Charmaine Rose Inandan Triviño100% (2)
- CHN CHP 5Document4 pagesCHN CHP 5Charmaine Rose Inandan Triviño0% (1)
- Imci-Integrated Management of Childhood Illness - 1992 - 2 Pilot Areas AreDocument18 pagesImci-Integrated Management of Childhood Illness - 1992 - 2 Pilot Areas Arej0nna_02No ratings yet
- Community Health Nursing Review NotesDocument12 pagesCommunity Health Nursing Review NotesISICLE GTNo ratings yet
- Study Questions 2Document10 pagesStudy Questions 2CGNo ratings yet
- Letter of Instruction 949Document6 pagesLetter of Instruction 949Wynna SegundoNo ratings yet
- NCM 109 - Finals CompilationDocument54 pagesNCM 109 - Finals CompilationMaria KawilanNo ratings yet
- Midterms in CHNDocument8 pagesMidterms in CHNcharmaineNo ratings yet
- Fundamentals of Community Health NursingDocument8 pagesFundamentals of Community Health NursingAziil LiizaNo ratings yet
- Nur 192 CHN Lec Session 1 23Document70 pagesNur 192 CHN Lec Session 1 23James Eugene CaasiNo ratings yet
- Comprefinal RleDocument11 pagesComprefinal RleHEIDE BASING-ANo ratings yet
- Essential Primary Health Care ExplainedDocument11 pagesEssential Primary Health Care ExplainedHet rodNo ratings yet
- ECOMAP Community Health Nursing CHNDocument1 pageECOMAP Community Health Nursing CHNmNo ratings yet
- Developing The Family Nursing Care PlanDocument11 pagesDeveloping The Family Nursing Care PlanGenn Medrano GirayNo ratings yet
- Copar DocumentationDocument57 pagesCopar DocumentationEdison Olad Dangkeo, RN,RMNo ratings yet
- Transforming lives through sustainable developmentDocument48 pagesTransforming lives through sustainable developmentbekbekk cabahugNo ratings yet
- CHN Quiz 1Document4 pagesCHN Quiz 1Jam PipikanNo ratings yet
- National nutrition and immunization programsDocument12 pagesNational nutrition and immunization programsTine SabaulanNo ratings yet
- P 2Document7 pagesP 2Aijem RyanNo ratings yet
- Assessing Community Health ProblemsDocument5 pagesAssessing Community Health ProblemsMARC JOSHUA SARANILLONo ratings yet
- Typology of Family Nursing ProblemDocument9 pagesTypology of Family Nursing ProblemJohn Patrick Leal QuinesNo ratings yet
- Family Health Nursing CHN (Start Midterm)Document4 pagesFamily Health Nursing CHN (Start Midterm)Aiza OronceNo ratings yet
- Nutri Lab P1p2rbe Exam 2 2Document16 pagesNutri Lab P1p2rbe Exam 2 2SandyNo ratings yet
- HES 032 - SAS 1 - Merged-1Document1 pageHES 032 - SAS 1 - Merged-1bangtanswifue -No ratings yet
- Family Nursing Care PlanDocument26 pagesFamily Nursing Care PlanAmira Fatmah QuilapioNo ratings yet
- Quiz 2 Obstetrics Nursing: Untitled SectionDocument11 pagesQuiz 2 Obstetrics Nursing: Untitled SectionBeverly DatuNo ratings yet
- CHILD HEALTH NCLEX QUESTIONSDocument42 pagesCHILD HEALTH NCLEX QUESTIONSEllen AngelNo ratings yet
- MCN II NewbornDocument14 pagesMCN II NewbornJharaNo ratings yet
- Nur 194 Sas 2Document2 pagesNur 194 Sas 2Orange AlvarezNo ratings yet
- Family Nursing ProcessDocument25 pagesFamily Nursing ProcessJAMES ROD MARINDUQUE100% (1)
- OVERVIEW OF CHN CONCEPTSDocument15 pagesOVERVIEW OF CHN CONCEPTSChiz EscubuaNo ratings yet
- Baguio Central University College of Nursing Comprehensive Exam.-ChnDocument9 pagesBaguio Central University College of Nursing Comprehensive Exam.-ChnKristian Karl Bautista Kiw-isNo ratings yet
- Community Health Nursing Roles and ResponsibilitiesDocument7 pagesCommunity Health Nursing Roles and ResponsibilitiesIsabel Bibat DavidNo ratings yet
- SC CHN Imci Post Test 50items Mr. JV GasminDocument4 pagesSC CHN Imci Post Test 50items Mr. JV Gasmincianm1143No ratings yet
- Family Developmental TaskDocument4 pagesFamily Developmental TaskFirenze Fil100% (2)
- Nursing Practice IDocument3 pagesNursing Practice IななみけんとNo ratings yet
- Application of Nursing Standards Is A Must in Community Health Nursing. To Whom of The Following Do These Standards Apply?Document27 pagesApplication of Nursing Standards Is A Must in Community Health Nursing. To Whom of The Following Do These Standards Apply?L1NEDS DNo ratings yet
- Assessing Community Health NeedsDocument8 pagesAssessing Community Health NeedsYeany IddiNo ratings yet
- Chapter 012 PSDocument12 pagesChapter 012 PSJann ericka JaoNo ratings yet
- Nursing Problems TypologyDocument8 pagesNursing Problems TypologyClifford Ogad0% (1)
- Philippine Health Agenda - Dec1 - 1 PDFDocument26 pagesPhilippine Health Agenda - Dec1 - 1 PDFreyalene gallegosNo ratings yet
- CHN Prelim QuizDocument5 pagesCHN Prelim QuizVanessa Mae Rara100% (1)
- Sas 15 MCN Lec 2Document3 pagesSas 15 MCN Lec 2Jhoanna Marie VillaverdeNo ratings yet
- Bermudez, Rosette - CHN-2 Midterm ExamDocument22 pagesBermudez, Rosette - CHN-2 Midterm ExamRosette Mae BermudezNo ratings yet
- Competency Appraisal Imci Set BDocument5 pagesCompetency Appraisal Imci Set BEden Marie FranciscoNo ratings yet
- NUR 193 RLE Student - S GuideDocument59 pagesNUR 193 RLE Student - S GuideAntoinette PeleñaNo ratings yet
- Community Health Nursing Exam 1 - 198 TermsDocument80 pagesCommunity Health Nursing Exam 1 - 198 TermsCharaNo ratings yet
- Family Assessment FormDocument4 pagesFamily Assessment FormJulianne Kyla MercadoNo ratings yet
- Family Health Assessment Form CHN LABDocument6 pagesFamily Health Assessment Form CHN LABAriane SalibioNo ratings yet
- Surigao Education Center Km.2 Surigao City, PhilippinesDocument5 pagesSurigao Education Center Km.2 Surigao City, PhilippinesJoanne Bernadette AguilarNo ratings yet
- CHN AssessmentDocument2 pagesCHN AssessmentJohn SecretNo ratings yet
- Selario Family Health Assessment FormDocument7 pagesSelario Family Health Assessment FormMaria Rosario Pangilinan SagmitNo ratings yet
- Health Education: Trust Is Essential To Initiate Any Formal Teaching, SoDocument1 pageHealth Education: Trust Is Essential To Initiate Any Formal Teaching, SoKlaire DynNo ratings yet
- EMILIO AGUINALDO COLLEGE Health Education AssignmentDocument1 pageEMILIO AGUINALDO COLLEGE Health Education AssignmentKlaire DynNo ratings yet
- Search For History of Bioethics and Write A Reflection Paper (200 Words) Submit in Word FormatDocument2 pagesSearch For History of Bioethics and Write A Reflection Paper (200 Words) Submit in Word FormatKlaire DynNo ratings yet
- Search For History of Bioethics and Write A Reflection Paper (200 Words) Submit in Word FormatDocument2 pagesSearch For History of Bioethics and Write A Reflection Paper (200 Words) Submit in Word FormatKlaire DynNo ratings yet
- Write About Your Stand On The Issue of Abortion. Search For Journals or Articles To Support Your StatementDocument3 pagesWrite About Your Stand On The Issue of Abortion. Search For Journals or Articles To Support Your StatementKlaire DynNo ratings yet
- Postpartum HTPDocument2 pagesPostpartum HTPGershom Perez AcaboNo ratings yet
- Rhea TestDocument3 pagesRhea Testerma090308No ratings yet
- COVID vaccination certificate for Indian teenDocument1 pageCOVID vaccination certificate for Indian teenShubham TiwariNo ratings yet
- Chittaranjan National Cancer Institute: Test ReportDocument1 pageChittaranjan National Cancer Institute: Test ReportscribbNo ratings yet
- Advances in The Diagnosis of Preterm LabourDocument22 pagesAdvances in The Diagnosis of Preterm LabouranggialwieNo ratings yet
- Contraception and Sterilization FinalDocument2 pagesContraception and Sterilization FinalRasheedAladdinNGuiomalaNo ratings yet
- Vaccination 810805065288Document1 pageVaccination 810805065288tinaNo ratings yet
- NP2 Nursing Board Exam November 2008Document16 pagesNP2 Nursing Board Exam November 2008Clarissa GuifayaNo ratings yet
- Course Outline: OCCUPATIONAL SAFETY AND HEALTH Course Is Designed To ImpartDocument5 pagesCourse Outline: OCCUPATIONAL SAFETY AND HEALTH Course Is Designed To ImpartNorzelan Saleh100% (2)
- LPL-PATNA Lab Report for Hepatitis B and C ScreeningDocument6 pagesLPL-PATNA Lab Report for Hepatitis B and C ScreeningRajarshi BhattacharyaNo ratings yet
- Online Assignment 4Document6 pagesOnline Assignment 4Ab Staholic BoiiNo ratings yet
- Abortion Using Misoprostol Pills: Before SmaDocument1 pageAbortion Using Misoprostol Pills: Before SmaAhmad Shah SyedNo ratings yet
- CPG Cap 2010Document12 pagesCPG Cap 2010RenatoCosmeGalvanJuniorNo ratings yet
- Canesten Clotrimazole Vaginal Products: Rescheduling Application ForDocument38 pagesCanesten Clotrimazole Vaginal Products: Rescheduling Application ForneleatucicovshiiNo ratings yet
- Community Health Nursing (Learning Feedback Diary (LFD #30)Document3 pagesCommunity Health Nursing (Learning Feedback Diary (LFD #30)Angelica Malacay RevilNo ratings yet
- National Ten-Year Cancer Control Strategy - 2021-2025 RoadmapDocument76 pagesNational Ten-Year Cancer Control Strategy - 2021-2025 RoadmapWac GunarathnaNo ratings yet
- Gesc 113Document13 pagesGesc 113Lively DoseNo ratings yet
- Cultural Competence or Cultural Humility Moving Beyond The DebateDocument4 pagesCultural Competence or Cultural Humility Moving Beyond The DebateEstela MedinaNo ratings yet
- Polio EradicationDocument9 pagesPolio Eradicationsobia salmanNo ratings yet
- Common Cancers in WomenDocument49 pagesCommon Cancers in WomenNaghib BogereNo ratings yet
- Annex B Checklist of Safe Management MeasuresDocument7 pagesAnnex B Checklist of Safe Management MeasuresJay PoNo ratings yet
- OB Case Study 1Document2 pagesOB Case Study 1SdvNo ratings yet
- Midwives and Nutrition Education During Pregnancy - A Literature RDocument23 pagesMidwives and Nutrition Education During Pregnancy - A Literature RSuredaNo ratings yet
- Global Health Priorities AssignmentDocument3 pagesGlobal Health Priorities Assignmentapi-239807389100% (1)
- American Needle Guard - Dental Needle Guard in NYCDocument4 pagesAmerican Needle Guard - Dental Needle Guard in NYCSyed Sajjad RazaNo ratings yet
- Yaws Eradication ProgrammeDocument82 pagesYaws Eradication ProgrammeAparna Aby50% (2)
- PTA Resolution for Donation to School WashroomDocument2 pagesPTA Resolution for Donation to School WashroomMara Ciela CajalneNo ratings yet