You might also like
- Argumentative Research EssayDocument6 pagesArgumentative Research EssayMeagan SpeckNo ratings yet
- Colon Cancer Care PlanDocument4 pagesColon Cancer Care PlanTony Festa100% (3)
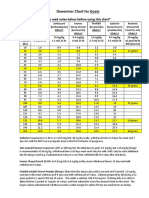
- Dewormer Chart GoatsDocument2 pagesDewormer Chart GoatsAbu Bakr AtikuNo ratings yet
- Space Planning Guide For Community Health Care Facilities (2014-12-22) PDFDocument45 pagesSpace Planning Guide For Community Health Care Facilities (2014-12-22) PDFJuan José Sepúlveda MolinaNo ratings yet
- Effects of Massage and Acupressure On Relieving.10Document9 pagesEffects of Massage and Acupressure On Relieving.10Riska amaliaNo ratings yet
- Effects of Massage and Acupressure OnDocument9 pagesEffects of Massage and Acupressure OnSyahlu DamayantiiNo ratings yet
- Pain Science in Practice - What Is Pain Neuroscience Part 2Document3 pagesPain Science in Practice - What Is Pain Neuroscience Part 2MathildeNo ratings yet
- Jurnal International 2Document11 pagesJurnal International 2FitriiNo ratings yet
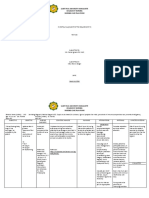
- Saint Paul University Dumaguete College of Nursing Nursing Care Plan FormDocument10 pagesSaint Paul University Dumaguete College of Nursing Nursing Care Plan FormMary Rose Silva GargarNo ratings yet
- Therapeutic Touch: Influence On Vital Signs of NewbornsDocument5 pagesTherapeutic Touch: Influence On Vital Signs of NewbornsYossi ArabNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- 2015 - Effects of Deep Pressure Stimulation On Physiological Arousal VAYU VEST With STRESSOR MORON TESTDocument5 pages2015 - Effects of Deep Pressure Stimulation On Physiological Arousal VAYU VEST With STRESSOR MORON TESTM Izzur MaulaNo ratings yet
- Anaklgesia Intraop PosopDocument10 pagesAnaklgesia Intraop PosopChurrunchaNo ratings yet
- Effect of Effleurage Techniques To Inten 82ec4d7d PDFDocument7 pagesEffect of Effleurage Techniques To Inten 82ec4d7d PDFeka istiyaniNo ratings yet
- Effect of Lavender Oil Massage On Pain Perception During First Stage of Labour Among Primi ParturientsDocument9 pagesEffect of Lavender Oil Massage On Pain Perception During First Stage of Labour Among Primi ParturientsIJAR JOURNALNo ratings yet
- TL 4Document4 pagesTL 4ĐôngNo ratings yet
- Efek Hipnosis Dalam Mengurangi Nyeri Pasca OperasiDocument13 pagesEfek Hipnosis Dalam Mengurangi Nyeri Pasca OperasiRisa PrimeNo ratings yet
- 2009 Fischer Chronic Pain in Ayurveda Medicine and Neuroscience An Integrative Medical ApproachDocument1 page2009 Fischer Chronic Pain in Ayurveda Medicine and Neuroscience An Integrative Medical Approachnermal93No ratings yet
- Kinesio Taping Does Not Provide Additional Bene Ts in Patients With Chronic Low Back Pain Who Receive Exercise and Manual Therapy A Randomized Controlled TrialDocument8 pagesKinesio Taping Does Not Provide Additional Bene Ts in Patients With Chronic Low Back Pain Who Receive Exercise and Manual Therapy A Randomized Controlled TrialMichele GonçalvesNo ratings yet
- Jurnal IntranatalDocument2 pagesJurnal Intranataledy wibowoseptiNo ratings yet
- The Effect of GB21 Acupressure On PainDocument5 pagesThe Effect of GB21 Acupressure On PainSiti AisahNo ratings yet
- 13 Movement and Massage Therapy Reduce Fibromyalgia PainDocument4 pages13 Movement and Massage Therapy Reduce Fibromyalgia PainARCHON SCARNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Assessment Diagnosis Planning Intervention Rationale EvaluationJoselyn M. LachicaNo ratings yet
- 104-107 Reeja Mariam PDFDocument4 pages104-107 Reeja Mariam PDFMoh. Arif Sahrani Hi. HarunNo ratings yet
- KT Trial Added JOSPT2016Document8 pagesKT Trial Added JOSPT2016Ju ChangNo ratings yet
- 3 Effleurage LuarDocument6 pages3 Effleurage LuarYeni terryNo ratings yet
- The Effect of Sacral Massage On Labor Pain and Anxiety A Randomized Controlled TrialDocument23 pagesThe Effect of Sacral Massage On Labor Pain and Anxiety A Randomized Controlled TrialAnonymous DDIQ0jIsV9No ratings yet
- Information About ArticleDocument6 pagesInformation About ArticleYeni terryNo ratings yet
- Pain Management During Labor & Second Stage of LaborDocument97 pagesPain Management During Labor & Second Stage of LaborTheMothershipNo ratings yet
- Rose Aromatherapy in OpDocument5 pagesRose Aromatherapy in OpdianNo ratings yet
- Acupuncture in Reproductive MedicineDocument13 pagesAcupuncture in Reproductive MedicineyohanNo ratings yet
- Jospt 2020 0601Document5 pagesJospt 2020 0601Gajen SinghNo ratings yet
- Drug StudyDocument3 pagesDrug StudyFrances Katherine GarciaNo ratings yet
- Bedah Iskandar Japardi53Document8 pagesBedah Iskandar Japardi53Ria Ulfha IndrianyNo ratings yet
- ACCUPRESUREDocument8 pagesACCUPRESUREedita astuti panjaitanNo ratings yet
- Mind and Body ConnectionDocument4 pagesMind and Body ConnectionANANYA AGARWAL 20224305No ratings yet
- 35 Aml ELmetwaly For PublishingDocument13 pages35 Aml ELmetwaly For PublishingDinda Resty L DNo ratings yet
- Effect of Acupressure Therapy Point HT 6 and LI 4 On Post Cesarean Sectio's PainDocument4 pagesEffect of Acupressure Therapy Point HT 6 and LI 4 On Post Cesarean Sectio's PainbelaNo ratings yet
- 2554 10028 1 PB PDFDocument4 pages2554 10028 1 PB PDFbelaNo ratings yet
- Neuraxial Analgesia For Labour 2020 InglesDocument7 pagesNeuraxial Analgesia For Labour 2020 InglesDenis Andres Manzanero MarinNo ratings yet
- Perioperative Pain Management in Colorectal Surgery: Vinay Ratnalikar Catrin Williams Thomas MosesDocument7 pagesPerioperative Pain Management in Colorectal Surgery: Vinay Ratnalikar Catrin Williams Thomas Mosesdian lukman hakimNo ratings yet
- The Effect of Shiatsu Massage On Pain Reduction in Burn PatientsDocument4 pagesThe Effect of Shiatsu Massage On Pain Reduction in Burn Patientskaterine viafaraNo ratings yet
- Jurnal InterDocument11 pagesJurnal InterINDAHNo ratings yet
- Guided Imagery For Post OperationDocument10 pagesGuided Imagery For Post OperationDwi NoviyaniNo ratings yet
- PDF - Published Version BostDocument7 pagesPDF - Published Version Bostmuratigdi96No ratings yet
- 233 Full PDFDocument5 pages233 Full PDFrizk86No ratings yet
- Internasional 1Document6 pagesInternasional 1FitriiNo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- Efficacy of Birth Ball Exercises On Labour Pain ManagementDocument7 pagesEfficacy of Birth Ball Exercises On Labour Pain ManagementWenny Indah Purnama Eka SariNo ratings yet
- Non-Pharmacological Pain Relief Measures During Labor and DeliveryDocument14 pagesNon-Pharmacological Pain Relief Measures During Labor and DeliveryStudent NurseNo ratings yet
- Jurnal Kecemasan Pre OpDocument4 pagesJurnal Kecemasan Pre OpDevi FatmawatiNo ratings yet
- Week 7 Careplan OnlyDocument2 pagesWeek 7 Careplan Onlyapi-381357393No ratings yet
- Patil 2016Document8 pagesPatil 2016Ichwan MalikNo ratings yet
- 1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileDocument6 pages1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileValdemar Caumo JuniorNo ratings yet
- Rizky Asta Pramesti Rini - ID 139Document10 pagesRizky Asta Pramesti Rini - ID 139Rizky KykyNo ratings yet
- TherapyDocument6 pagesTherapynabilaNo ratings yet
- Rafin NCP and Drug StudyDocument7 pagesRafin NCP and Drug StudyCezanne CruzNo ratings yet
- New Labor Treatment OptionsDocument9 pagesNew Labor Treatment OptionsSarone juniorNo ratings yet
- Relieveing PainDocument12 pagesRelieveing PainAgitha PutriNo ratings yet
- PAINDocument35 pagesPAINassumptaNo ratings yet
- Artigo SaúdeDocument4 pagesArtigo SaúdePauloNo ratings yet
- Complejidad Back Pain Peter o SullivanDocument9 pagesComplejidad Back Pain Peter o SullivanAntonio tapiaNo ratings yet
- Preemptive Analgesia in Oral Surgery (Pain Vaccination) - A ReviewDocument27 pagesPreemptive Analgesia in Oral Surgery (Pain Vaccination) - A ReviewAshish DadhaniaNo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- SeizuresDocument1 pageSeizuresRock GoodNo ratings yet
- OT in The ICU Student PresentationDocument37 pagesOT in The ICU Student PresentationMochammad Syarief HidayatNo ratings yet
- Smt. B.N.B Swaminarayan Pharmacy College, Salvav Dr. Kantilal Narkhede BP103TP Pharmaceutics 1 Question BankDocument6 pagesSmt. B.N.B Swaminarayan Pharmacy College, Salvav Dr. Kantilal Narkhede BP103TP Pharmaceutics 1 Question BankAvinash MansukNo ratings yet
- ConfidentialityDocument57 pagesConfidentialityPriya Sharma75% (12)
- Hospital Administration Role in Quality PatientcareDocument41 pagesHospital Administration Role in Quality PatientcareMuhammad Abeesh100% (2)
- Physiotherapy Role and BenefitsDocument2 pagesPhysiotherapy Role and BenefitsGet Better Physiotherapy CentreNo ratings yet
- DepressantsDocument6 pagesDepressantsArvinjohn GacutanNo ratings yet
- Local Government and The Delivery of Immunization Service A Study of Selected Local Governments in Kaduna State, Nigeria.Document246 pagesLocal Government and The Delivery of Immunization Service A Study of Selected Local Governments in Kaduna State, Nigeria.Taiwo ArowoloNo ratings yet
- Managing Geriatric PatientsDocument8 pagesManaging Geriatric PatientsSarah KahilNo ratings yet
- Lesson 5 Pharma Extra LectureDocument2 pagesLesson 5 Pharma Extra Lecturethe someoneNo ratings yet
- The Influence of Contextual Factors On Healthcare Quality Improvement Initiatives: A Realist ReviewDocument22 pagesThe Influence of Contextual Factors On Healthcare Quality Improvement Initiatives: A Realist ReviewArseniojakejr FloresNo ratings yet
- ASTRIDE BasedThreatModelforTelehealthSystemsDocument16 pagesASTRIDE BasedThreatModelforTelehealthSystemsfernando PalloNo ratings yet
- Syllabus For BPKMCH NEPALDocument7 pagesSyllabus For BPKMCH NEPALDeep SharmaNo ratings yet
- DOH Breast Cancer Guidelines FinalDocument123 pagesDOH Breast Cancer Guidelines Finalsupratimbiswas073380No ratings yet
- Test Bank For Foundations and Adult Health Nursing 6th Edition Barbara ChristensenDocument24 pagesTest Bank For Foundations and Adult Health Nursing 6th Edition Barbara Christensenamandabrockxwfandpiyr100% (44)
- Manual HumanaDocument80 pagesManual HumanaGuille GuerraNo ratings yet
- Nursing Care Plan Placenta PreviaDocument2 pagesNursing Care Plan Placenta PreviaLei Ortega100% (3)
- Katz IndexDocument2 pagesKatz IndexnhengjrNo ratings yet
- Big Group A1 General Task 1 Nursing AssessmentDocument15 pagesBig Group A1 General Task 1 Nursing AssessmentCAUSIN, Lance Matthew,No ratings yet
- Improving Performance and Outcomes: Section 7Document4 pagesImproving Performance and Outcomes: Section 7Andrew WongNo ratings yet
- Health Recharge - Single SheeterDocument2 pagesHealth Recharge - Single SheeterRavi JoshiNo ratings yet
- HCA Healthcare/HealthONE Names Ryan Simpson President and CEO of The Medical Center of Aurora and Spalding Rehabilitation HospitalDocument3 pagesHCA Healthcare/HealthONE Names Ryan Simpson President and CEO of The Medical Center of Aurora and Spalding Rehabilitation HospitalPR.comNo ratings yet
- Per Schizo PDFDocument158 pagesPer Schizo PDFNarendraNo ratings yet
- Test Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithDocument17 pagesTest Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithMary Bartolomeo100% (35)
- (START HERE) 7 Day Feminine Transformation WorkbookDocument37 pages(START HERE) 7 Day Feminine Transformation Workbookt6w5g27n4qNo ratings yet
- Referensi Jurnal Berdasarkan Harvard Style, Apa Style, Dan Vancouver StyleDocument9 pagesReferensi Jurnal Berdasarkan Harvard Style, Apa Style, Dan Vancouver StyleWisnu 12No ratings yet