You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Icu - SG 2 2Document230 pagesIcu - SG 2 2Charlie AbagonNo ratings yet
- Pertussis: A Reading OnDocument8 pagesPertussis: A Reading OnCharlie AbagonNo ratings yet
- Newborn Assessment: A Reading OnDocument14 pagesNewborn Assessment: A Reading OnCharlie AbagonNo ratings yet
- NCM204 Page 361-471Document43 pagesNCM204 Page 361-471Charlie AbagonNo ratings yet
- Endorsement PDFDocument34 pagesEndorsement PDFCharlie Abagon100% (3)
- Family Planning CHN RotDocument7 pagesFamily Planning CHN RotCharlie AbagonNo ratings yet
- IIII :::: : S EsentDocument22 pagesIIII :::: : S EsentCharlie AbagonNo ratings yet
- Sinabawan G Gulay: Presented By: Group 1 of BSN 2JDocument21 pagesSinabawan G Gulay: Presented By: Group 1 of BSN 2JCharlie AbagonNo ratings yet
- Anti - Viral: Topical Antivirals (HSV)Document2 pagesAnti - Viral: Topical Antivirals (HSV)Charlie AbagonNo ratings yet
- CHN Implementing Family Care PlanDocument2 pagesCHN Implementing Family Care PlanCharlie Abagon100% (1)
- FCT Updated 2Document3 pagesFCT Updated 2Charlie AbagonNo ratings yet
- Chapter 13 - Lymphatic SystemDocument4 pagesChapter 13 - Lymphatic SystemCharlie AbagonNo ratings yet
- Foods, Nutrients Other SubstancesDocument35 pagesFoods, Nutrients Other SubstancesCharlie AbagonNo ratings yet
- Site of The First MassDocument6 pagesSite of The First MassCharlie AbagonNo ratings yet
- Phenol and Phenolics: AlcoholsDocument2 pagesPhenol and Phenolics: AlcoholsCharlie AbagonNo ratings yet
- BEDMAKINGDocument7 pagesBEDMAKINGCharlie AbagonNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PDEA Updates 2015Document100 pagesPDEA Updates 2015Jill Marie Arabia100% (1)
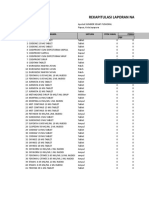
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDocument11 pagesRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFBang23 ManikNo ratings yet
- Philippine LawsDocument1 pagePhilippine LawsWenn Joyrenz ManeclangNo ratings yet
- To Study The Effect of Various Tranquilizers and Sedatives On Motor Co-Ordination by Rotarod Test in Mice PDFDocument2 pagesTo Study The Effect of Various Tranquilizers and Sedatives On Motor Co-Ordination by Rotarod Test in Mice PDFSuman DahalNo ratings yet
- Acute Toxicity Study of Malli Chooranam A Siddha FormulationDocument2 pagesAcute Toxicity Study of Malli Chooranam A Siddha FormulationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- VasopressinDocument3 pagesVasopressinChristian Dave EndinoNo ratings yet
- ColistinDocument2 pagesColistinGwyn RosalesNo ratings yet
- Thymus Vulgaris - TimijanDocument8 pagesThymus Vulgaris - TimijanRok KopinčNo ratings yet
- Hi Alert MedicationsHHHIGHDocument27 pagesHi Alert MedicationsHHHIGHnovitalumintusariNo ratings yet
- Assignment 3 Design Personal Training ProgramDocument3 pagesAssignment 3 Design Personal Training ProgramEjhay TenderoNo ratings yet
- Registered Medicine List 07-04-2014 Sse Frequently UpdatedDocument116 pagesRegistered Medicine List 07-04-2014 Sse Frequently Updatedjema; belihuNo ratings yet
- Ferron Glumin XRDocument22 pagesFerron Glumin XRhilmayuniarNo ratings yet
- TrazodoneDocument20 pagesTrazodoneAjay MehtaNo ratings yet
- Unit-III and IVDocument82 pagesUnit-III and IVJamaicah SinceroNo ratings yet
- Kubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyDocument6 pagesKubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyMikaelaMundell100% (1)
- Worksheet 3: (2 Points) (2 Points)Document2 pagesWorksheet 3: (2 Points) (2 Points)KingxMagic lopezNo ratings yet
- Fluoxetine Hydro ChlorideDocument3 pagesFluoxetine Hydro Chlorideapi-3797941No ratings yet
- Drug StudyDocument2 pagesDrug StudyAlyssa Marie PepitoNo ratings yet
- DS PNSSDocument4 pagesDS PNSSKathryne May JinonNo ratings yet
- Doh Do 0223Document19 pagesDoh Do 0223J Velasco PeraltaNo ratings yet
- Drug Study RifampicinDocument2 pagesDrug Study RifampicinJamil Lorca100% (5)
- Drug Management Cycle: Adryan Fristiohady Program Studi Pendidikan Profesi Apoteker Universitas Halu OleoDocument34 pagesDrug Management Cycle: Adryan Fristiohady Program Studi Pendidikan Profesi Apoteker Universitas Halu OleoLhynda Priarti Latif100% (4)
- Humulin R: Regular U-500 (Concentrated) Insulin Human Injection, Usp (Rdna Origin)Document7 pagesHumulin R: Regular U-500 (Concentrated) Insulin Human Injection, Usp (Rdna Origin)Rebecca BlackburnNo ratings yet
- Unit 2 Notes-1Document15 pagesUnit 2 Notes-1Manuel Christopher MontesclarosNo ratings yet
- Presentation On: Beximco PharmaDocument37 pagesPresentation On: Beximco PharmaToukir Ahmed100% (1)
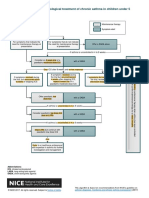
- Algorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5Document1 pageAlgorithm D: Pharmacological Treatment of Chronic Asthma in Children Under 5samNo ratings yet
- No Person Can Dispence Medicnine Other Then Reg PharmacistDocument22 pagesNo Person Can Dispence Medicnine Other Then Reg PharmacistSandeep PandeyNo ratings yet
- Unit I General PharmacologyDocument16 pagesUnit I General PharmacologycuolyNo ratings yet
- Appropriate Use of Laxatives in The Older PersonDocument7 pagesAppropriate Use of Laxatives in The Older PersonStacey WoodsNo ratings yet
- Chapter 6Document39 pagesChapter 6A kNo ratings yet