You might also like
- Marquez - Case Study 4Document4 pagesMarquez - Case Study 4Caren MarquezNo ratings yet
- Marquez - Case Study 3Document6 pagesMarquez - Case Study 3Caren MarquezNo ratings yet
- Marquez - Case Study 122Document5 pagesMarquez - Case Study 122Caren MarquezNo ratings yet
- Marquez - Case Study 120Document4 pagesMarquez - Case Study 120Caren Marquez100% (1)
- MCQs in Pediatrics Review of Nelson Textbook of Pediatrics (PDFDrive)Document642 pagesMCQs in Pediatrics Review of Nelson Textbook of Pediatrics (PDFDrive)GrInDoVe9097No ratings yet
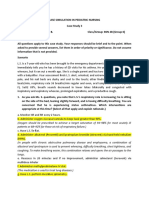
- Case Simulation 3 in Pediatric NursingDocument3 pagesCase Simulation 3 in Pediatric NursingCaren MarquezNo ratings yet
- Head Lice 101 For ParentsDocument2 pagesHead Lice 101 For Parentsapi-269333320No ratings yet
- Nelson 20th MCQDocument593 pagesNelson 20th MCQcharlesy T89% (19)
- Case Simulation in Pediatric Nursing Case Study 2 InstructionsDocument2 pagesCase Simulation in Pediatric Nursing Case Study 2 InstructionsCheska PalomaNo ratings yet
- Head Lice Infestation in Children: Treatment in The School Setting Amanda Hill Georgia Highlands CollegeDocument6 pagesHead Lice Infestation in Children: Treatment in The School Setting Amanda Hill Georgia Highlands CollegeblueyesmileNo ratings yet
- Scabies LiceDocument28 pagesScabies Liceapi-256362380No ratings yet
- Infestation and BitesDocument76 pagesInfestation and Bitesedi büdüNo ratings yet
- RingwormDocument20 pagesRingwormCj LowryNo ratings yet
- Appendix 8 Sample Notification Letters To ParentsDocument12 pagesAppendix 8 Sample Notification Letters To ParentsEdward AkumNo ratings yet
- Case Study IGDocument2 pagesCase Study IGCheha PaikNo ratings yet
- Pediculosis CapitisDocument13 pagesPediculosis CapitisMaria Teresa LazarteNo ratings yet
- MajorDocument16 pagesMajorElla Mharie Muñasque GabijanNo ratings yet
- IntegumentaryDocument1 pageIntegumentaryCoffee CojjeeNo ratings yet
- AAP Head Lice 2017 - HealthyChildren.orgDocument5 pagesAAP Head Lice 2017 - HealthyChildren.orgYan Zhen YuanNo ratings yet
- E1355 Full PDFDocument13 pagesE1355 Full PDFJëññy ÑõvëmbêrNo ratings yet
- A Well Visit With the Focused Dermatological ExamDocument5 pagesA Well Visit With the Focused Dermatological ExamReinhard OmuyaNo ratings yet
- Hair HygieneDocument9 pagesHair HygieneanikyulaikhaNo ratings yet
- AKTDocument10 pagesAKTMohammad RammalNo ratings yet
- Assignment IndividualDocument10 pagesAssignment Individualkartini272597No ratings yet
- Lice and Scabies: Treatment UpdateDocument11 pagesLice and Scabies: Treatment UpdateYar ZepolNo ratings yet
- Efficacy of Paragis Chapter 1Document5 pagesEfficacy of Paragis Chapter 1ellyzaherbolingo0No ratings yet
- Management Pediculosis Capitis: Parasitology Section, Faculty of Medicine, University of LampungDocument6 pagesManagement Pediculosis Capitis: Parasitology Section, Faculty of Medicine, University of LampungDiary JafNo ratings yet
- Download textbook Mcqs In Pediatrics Review Of Nelson Textbook Of Pediatrics 20Th Edition Zuhair M Almusawi ebook all chapter pdfDocument53 pagesDownload textbook Mcqs In Pediatrics Review Of Nelson Textbook Of Pediatrics 20Th Edition Zuhair M Almusawi ebook all chapter pdfsandra.millican277100% (7)
- Pediculosis (Lice Infestation) : Oklahoma State Department of Health 01-2015 ReviewedDocument8 pagesPediculosis (Lice Infestation) : Oklahoma State Department of Health 01-2015 ReviewedAgung PermanajatiNo ratings yet
- Pedikulosis + SkabiesDocument21 pagesPedikulosis + Skabiesjeams manuNo ratings yet
- Lippincott's PEDIATRIC9 ANSWERSDocument5 pagesLippincott's PEDIATRIC9 ANSWERSNursyNurseNo ratings yet
- Head LiceDocument15 pagesHead Licefarmasi_hmNo ratings yet
- Thesis Statement On EczemaDocument7 pagesThesis Statement On Eczemafjgqdmne100% (2)
- PediculosisDocument28 pagesPediculosisLucy PalmaNo ratings yet
- Child Evolve ExamDocument37 pagesChild Evolve Examfriendofnurse100% (14)
- NCLEX Practice Exam For Pediatric Nursing 1: Start StartDocument9 pagesNCLEX Practice Exam For Pediatric Nursing 1: Start StartLot RositNo ratings yet
- Scabies in Children and Its Outcome With Topical Permethrin and Oral Ivermectin: A Single Center Prospective StudyDocument5 pagesScabies in Children and Its Outcome With Topical Permethrin and Oral Ivermectin: A Single Center Prospective StudyChlo14No ratings yet
- Scabies Treatment in Children: A Narrative ReviewDocument8 pagesScabies Treatment in Children: A Narrative Reviewcut normaya putriNo ratings yet
- Final OutputDocument12 pagesFinal Outputellyzaherbolingo0No ratings yet
- School Nurse Presentation - LiceDocument12 pagesSchool Nurse Presentation - LiceDeonNo ratings yet
- Sas 22Document4 pagesSas 22Sistine Rose LabajoNo ratings yet
- NCLEX Practice Exam For Pediatric Nursing 2 - RNpediaDocument14 pagesNCLEX Practice Exam For Pediatric Nursing 2 - RNpediaLot Rosit100% (1)
- Enhancing The Parental Role in Controlling Pediatric Atopic Dermatitis A Narrative ReviewDocument13 pagesEnhancing The Parental Role in Controlling Pediatric Atopic Dermatitis A Narrative ReviewIJAR JOURNALNo ratings yet
- Chapter IIDocument12 pagesChapter IIellyzaherbolingo0No ratings yet
- Q3 Health 8 Module 5 PDFDocument13 pagesQ3 Health 8 Module 5 PDFkateNo ratings yet
- Child AbuseDocument3 pagesChild AbusevasabakaNo ratings yet
- Quan L. Do Parents Value Drowning Prevention Information at Discharge From The Emergency DepartmentDocument4 pagesQuan L. Do Parents Value Drowning Prevention Information at Discharge From The Emergency DepartmentVictoriaMuroNo ratings yet
- Managing Head Lice in The School Setting: Marjorie Cole, RN, MSNDocument48 pagesManaging Head Lice in The School Setting: Marjorie Cole, RN, MSNSampathSenadeeraNo ratings yet
- Health 6 Module Quarter 1Document30 pagesHealth 6 Module Quarter 1Eph RaimNo ratings yet
- Module 1 - EXPLOREDocument3 pagesModule 1 - EXPLOREJoan BabieraNo ratings yet
- A Semi - Detailed Lesson Plan in Caregiving 12Document2 pagesA Semi - Detailed Lesson Plan in Caregiving 12Jessa Mae JabegueroNo ratings yet
- Practice Test NCLEX-Suddarts: Compiled by ZudotaDocument55 pagesPractice Test NCLEX-Suddarts: Compiled by ZudotaNicholas TagleNo ratings yet
- Case Study 7 8 and 9Document32 pagesCase Study 7 8 and 9Lyca Ledesma JamonNo ratings yet
- Cilios Com Ptirus PubisDocument4 pagesCilios Com Ptirus PubisRafael CedroNo ratings yet
- MCQ NelsonDocument433 pagesMCQ NelsonShashank MisraNo ratings yet
- Literature Review of EczemaDocument6 pagesLiterature Review of Eczemaafmabkbhckmajg100% (1)
- This Article Previously Appeared in General Practice Update 2008Document8 pagesThis Article Previously Appeared in General Practice Update 2008gopscharanNo ratings yet
- Head LiceDocument5 pagesHead Licealan_kadir100% (1)
- Sample Essays For KidsDocument3 pagesSample Essays For Kidsezmt6r5c100% (2)
- Pthirus Pubis em Cilios - CriançaDocument2 pagesPthirus Pubis em Cilios - CriançaRafael CedroNo ratings yet
- Management of Headaches in Children and AdolescentsDocument13 pagesManagement of Headaches in Children and Adolescentsebmanansala0771pamNo ratings yet
- Argument Essay ReflectionDocument5 pagesArgument Essay Reflectionapi-509671089No ratings yet
- Dermatologist's Tips: Baby Skincare - How to Care for your Child's SkinFrom EverandDermatologist's Tips: Baby Skincare - How to Care for your Child's SkinRating: 5 out of 5 stars5/5 (2)
- Medical Emergencies in Early Childhood and School-Age SettingsFrom EverandMedical Emergencies in Early Childhood and School-Age SettingsNo ratings yet
- Nursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryDocument1 pageNursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryCaren MarquezNo ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- Marquez - Case Study 114Document6 pagesMarquez - Case Study 114Caren MarquezNo ratings yet
- Case StudyDocument7 pagesCase StudyCaren MarquezNo ratings yet
- Curriculum CTS Cosmetology NSQFDocument39 pagesCurriculum CTS Cosmetology NSQFPradnya gaikwadNo ratings yet
- Surprising Benefits of Papaya For Skin - Kishmish Organic PDFDocument8 pagesSurprising Benefits of Papaya For Skin - Kishmish Organic PDFSRG_007No ratings yet
- Regional Plastic Surgical Unit, Canniesburn Hospital, Bearsden, GlasgowDocument14 pagesRegional Plastic Surgical Unit, Canniesburn Hospital, Bearsden, Glasgowkoreta123No ratings yet
- International Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingDocument10 pagesInternational Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingAzri RahmadiNo ratings yet
- Wa0002Document7 pagesWa0002kush018kumarNo ratings yet
- Fungal & Parasitic Infestations of The SkinDocument67 pagesFungal & Parasitic Infestations of The SkinGhaith HamdiNo ratings yet
- Screening of Antimicrobial Activity of Varnya Lepa Lotion - A Polyherbal FormulationDocument5 pagesScreening of Antimicrobial Activity of Varnya Lepa Lotion - A Polyherbal FormulationIJAR JOURNALNo ratings yet
- The Physiology of The SkinDocument39 pagesThe Physiology of The SkinElvisNo ratings yet
- Everything Ocu Lop Last I A Make e Up PermanentDocument8 pagesEverything Ocu Lop Last I A Make e Up PermanentDaritza C. MoyanoNo ratings yet
- Pocket Dermatology Sara Hylwa, Elisabeth Hurliman, Jing Liu EtcDocument542 pagesPocket Dermatology Sara Hylwa, Elisabeth Hurliman, Jing Liu EtcMuhammad Ahmad bin makruf syammaku100% (1)
- US NomenclatureDocument7 pagesUS NomenclatureAngelSosaNo ratings yet
- The DoctorDocument6 pagesThe DoctorWritervpaVpaNo ratings yet
- Mergal 174II: Description Mergal Application/ Use HighlightsDocument4 pagesMergal 174II: Description Mergal Application/ Use HighlightsJose Gabriel Luis PencoNo ratings yet
- Cryotherapy AftercareDocument1 pageCryotherapy AftercareLi NguyenNo ratings yet
- 3 - Forensics 02 03 Botka Hair AnalysisDocument23 pages3 - Forensics 02 03 Botka Hair AnalysisFajar FebriantoNo ratings yet
- Acne Scars Nu PDFDocument315 pagesAcne Scars Nu PDFCristina Pop100% (2)
- Glycolic AcidDocument9 pagesGlycolic AcidNadaNo ratings yet
- Procedures and RationaleDocument7 pagesProcedures and RationaleMonmon BagarinaoNo ratings yet
- Young Nails Gel Product Education ManualDocument43 pagesYoung Nails Gel Product Education ManualPaola TNo ratings yet
- Burns: Burn and Its CausesDocument1 pageBurns: Burn and Its CausesRanjan MehrotraNo ratings yet
- Wound Concept - LuciaDocument41 pagesWound Concept - LuciaStevie kanenderNo ratings yet
- Getting Started With Create Cosmetic FormulasDocument25 pagesGetting Started With Create Cosmetic FormulasZEMOURANo ratings yet
- Gentle Black Deep Cleansing Oil KLAIRS SkincarismaDocument1 pageGentle Black Deep Cleansing Oil KLAIRS SkincarismaAkun PremiumNo ratings yet
- Jepretan Layar 2023-08-23 Pada 17.57.35Document51 pagesJepretan Layar 2023-08-23 Pada 17.57.35znwcskfpq8No ratings yet
- Review of Ayurvedic Herbs With K Esharanjana Property in The Management of Caniites (Palitya)Document4 pagesReview of Ayurvedic Herbs With K Esharanjana Property in The Management of Caniites (Palitya)Ujju LabanaNo ratings yet
- Waxing Full Leg (Final)Document5 pagesWaxing Full Leg (Final)Lionel YdeNo ratings yet
- A - Beat The Heat With These Summer Skin Care TipsDocument1 pageA - Beat The Heat With These Summer Skin Care TipsAjinkya A RandiveNo ratings yet
- JM 4411 GA Gelling AgentDocument5 pagesJM 4411 GA Gelling AgentRandy IpNo ratings yet
- Consensus Recommendations For The Use of Hyperdiluted Calcium Hydroxyapatite (Radiesse) As A Face and Body Biostimulatory Agent.Document9 pagesConsensus Recommendations For The Use of Hyperdiluted Calcium Hydroxyapatite (Radiesse) As A Face and Body Biostimulatory Agent.allen.515No ratings yet
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet