You might also like
- Chapter 26 - Introduction To The Urinary System (Also Table 27.4)Document7 pagesChapter 26 - Introduction To The Urinary System (Also Table 27.4)tomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 28 - The Reproductive SystemDocument7 pagesChapter 28 - The Reproductive Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 25 - Introduction To MetabolismDocument5 pagesChapter 25 - Introduction To Metabolismtomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 29 - Development and Inheritance: ST ND RD STDocument5 pagesChapter 29 - Development and Inheritance: ST ND RD STtomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 24 - Introduction To The Digestive SystemDocument7 pagesChapter 24 - Introduction To The Digestive Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 10 - An Introduction To Muscle TissueDocument7 pagesChapter 10 - An Introduction To Muscle Tissuetomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 17 - An Introduction To The Special Senses: Taste HairsDocument4 pagesChapter 17 - An Introduction To The Special Senses: Taste Hairstomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 14 - An Introduction To The Brain and Cranial NervesDocument5 pagesChapter 14 - An Introduction To The Brain and Cranial Nervestomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 20 - Introduction To The Cardiovascular System: Away From To BetweenDocument6 pagesChapter 20 - Introduction To The Cardiovascular System: Away From To Betweentomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 19 - BloodDocument5 pagesChapter 19 - Bloodtomorrow.today.yesterday .yesterdayNo ratings yet
- 511-525chapter 6-8 (5) The Spinal Cord, Spinal Nerves, and Spinal ReflexesDocument4 pages511-525chapter 6-8 (5) The Spinal Cord, Spinal Nerves, and Spinal Reflexestomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 2 - Chemistry: Ionization, DissociationDocument4 pagesChapter 2 - Chemistry: Ionization, Dissociationtomorrow.today.yesterday .yesterdayNo ratings yet
- 420-510chapter 1 (4) Types of TissuesDocument6 pages420-510chapter 1 (4) Types of Tissuestomorrow.today.yesterday .yesterdayNo ratings yet
- 420-510chapter 1 (5) Introduction To The Integumentary SystemDocument6 pages420-510chapter 1 (5) Introduction To The Integumentary Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- 511-525chapter 6-8 (2) An Introduction To ArticulationsDocument3 pages511-525chapter 6-8 (2) An Introduction To Articulationstomorrow.today.yesterday .yesterdayNo ratings yet
- 420-510chapter 1 (3) An Introduction To CellsDocument6 pages420-510chapter 1 (3) An Introduction To Cellstomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 15 - Neural Integration I: Sensory Pathways and Somatic Nervous SystemDocument4 pagesChapter 15 - Neural Integration I: Sensory Pathways and Somatic Nervous Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 12 - An Introduction To The Nervous System: Peripheral Nerves)Document7 pagesChapter 12 - An Introduction To The Nervous System: Peripheral Nerves)tomorrow.today.yesterday .yesterdayNo ratings yet
- 511-525chapter 6-8 (1) An Introduction To The Skeletal SystemDocument6 pages511-525chapter 6-8 (1) An Introduction To The Skeletal Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- 420-510chapter 1 (1) Introduction To Anatomy and PhysiologyDocument3 pages420-510chapter 1 (1) Introduction To Anatomy and Physiologytomorrow.today.yesterday .yesterdayNo ratings yet
- 147Document2 pages147tomorrow.today.yesterday .yesterdayNo ratings yet
- Chapter 21 - Blood VesselsDocument6 pagesChapter 21 - Blood Vesselstomorrow.today.yesterday .yesterdayNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
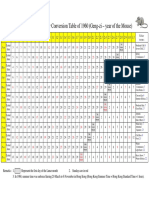
- Gregorian-Lunar Calendar Conversion Table of 1960 (Geng-Zi - Year of The Mouse)Document1 pageGregorian-Lunar Calendar Conversion Table of 1960 (Geng-Zi - Year of The Mouse)Anomali SahamNo ratings yet
- Micromine TutorialDocument5 pagesMicromine TutorialFerdinand Siahaan100% (1)
- Gulfpub Wo 201805Document81 pagesGulfpub Wo 201805Patricia.PNo ratings yet
- Study of Noise Mapping at Moolchand Road Phargang New DelhiDocument10 pagesStudy of Noise Mapping at Moolchand Road Phargang New DelhiEditor IJTSRDNo ratings yet
- Jazz - Installing LED DRLsDocument16 pagesJazz - Installing LED DRLsKrishnaNo ratings yet
- UBO - Lecture 07 - Implementing and Managing Organisational ChangeDocument0 pagesUBO - Lecture 07 - Implementing and Managing Organisational ChangeShahNooraniITNo ratings yet
- 67 9268Document34 pages67 9268Salvador ReyesNo ratings yet
- 1973 Essays On The Sources For Chinese History CanberraDocument392 pages1973 Essays On The Sources For Chinese History CanberraChanna LiNo ratings yet
- LPP - Problem Number 2Document9 pagesLPP - Problem Number 2CT SunilkumarNo ratings yet
- Reading in MCJ 216Document4 pagesReading in MCJ 216Shela Lapeña EscalonaNo ratings yet
- Think Feel DoDocument3 pagesThink Feel DoHardik MehtaNo ratings yet
- Ap Reg W# 5-Scaffold For Transfer TemplateDocument2 pagesAp Reg W# 5-Scaffold For Transfer TemplateJunafel Boiser Garcia100% (2)
- GE Elec 7 UNIT-3 NoDocument22 pagesGE Elec 7 UNIT-3 NoLyleNo ratings yet
- Memo For Completed RubricDocument3 pagesMemo For Completed Rubricnisev2003No ratings yet
- Adobe Scan 23-Feb-2024Document4 pagesAdobe Scan 23-Feb-2024muzwalimub4104No ratings yet
- Report Palazzetto Croci SpreadsDocument73 pagesReport Palazzetto Croci SpreadsUntaru EduardNo ratings yet
- Support of Roof and Side in Belowground Coal MinesDocument5 pagesSupport of Roof and Side in Belowground Coal MinesNavdeep MandalNo ratings yet
- Networking With OrganizationsDocument23 pagesNetworking With OrganizationsClaudette Lui Cabanos- Mercado-ReyesNo ratings yet
- Tadano450xl PDFDocument12 pagesTadano450xl PDFmunawar0% (1)
- 1 Raven's™ Standard Progressive Matrices Plus (SPM Plus) - PSI OnlineDocument1 page1 Raven's™ Standard Progressive Matrices Plus (SPM Plus) - PSI OnlineVINEET GAIROLANo ratings yet
- Sensory Play Activities Kids Will LoveDocument5 pagesSensory Play Activities Kids Will LoveGoh KokMingNo ratings yet
- Practical Econometrics Data Collection Analysis and Application 1st Edition Hilmer Test BankDocument27 pagesPractical Econometrics Data Collection Analysis and Application 1st Edition Hilmer Test Bankdavidhallwopkseimgc100% (28)
- Holiday Assignment (Dussehra Vacation) - 2022-23Document3 pagesHoliday Assignment (Dussehra Vacation) - 2022-23yogeshNo ratings yet
- The Status of The Translation ProfessionDocument172 pagesThe Status of The Translation ProfessionVeaceslav MusteataNo ratings yet
- Physics Cheat SheetDocument8 pagesPhysics Cheat SheetJeremiah MoussaNo ratings yet
- Fire and IceDocument11 pagesFire and IcelatishabasilNo ratings yet
- Omran WalidDocument196 pagesOmran WalidDébora AmougouNo ratings yet
- Variables in The EquationDocument3 pagesVariables in The EquationfiharjatinNo ratings yet
- Pursanova IXC ManualDocument16 pagesPursanova IXC ManualHector Serrano MagañaNo ratings yet
- NM Integrative Wellness MRC Public Health Acupuncture JITTDocument40 pagesNM Integrative Wellness MRC Public Health Acupuncture JITTPrince DhillonNo ratings yet