You might also like
- ENT For 4th YearDocument14 pagesENT For 4th YearabhishekNo ratings yet
- Nose MCQs Points RIDA NAQVI-1Document3 pagesNose MCQs Points RIDA NAQVI-1hamzaw213No ratings yet
- Cancer-Converted For PrintDocument18 pagesCancer-Converted For PrintTayyab RazaNo ratings yet
- Accurate assessment and prognosis of early nasopharyngeal carcinomaDocument15 pagesAccurate assessment and prognosis of early nasopharyngeal carcinomaWael ShamyNo ratings yet
- 2017 AprilDocument20 pages2017 AprilkiranNo ratings yet
- Nasopharyngeal Carcinoma Diagnosis and Treatment QuestionsDocument15 pagesNasopharyngeal Carcinoma Diagnosis and Treatment QuestionsAli QuwarahNo ratings yet
- ENT Batch 2022 Annual Paper-1Document9 pagesENT Batch 2022 Annual Paper-1mudassirahmedNo ratings yet
- Revision Note - 1 - ENT NuggetsDocument4 pagesRevision Note - 1 - ENT NuggetsNicNo ratings yet
- MCQ in Orl CourseDocument46 pagesMCQ in Orl CoursesulnaikNo ratings yet
- Soal Unas UGMDocument8 pagesSoal Unas UGMMonik AlamandaNo ratings yet
- Surgery One Liners Imp MciDocument41 pagesSurgery One Liners Imp Mciadi100% (2)
- Retropharyngeal Space Anatomy and InfectionsDocument18 pagesRetropharyngeal Space Anatomy and InfectionsShraavya ShivanandaNo ratings yet
- OMFS Question Bank-1Document55 pagesOMFS Question Bank-1Ahmed SalehNo ratings yet
- Ent PointsDocument9 pagesEnt PointsSaiNo ratings yet
- Ent Bcqs 3Document18 pagesEnt Bcqs 3Ghazi Uddin Ahmed0% (1)
- Davinci Medical AcademyDocument9 pagesDavinci Medical AcademyskNo ratings yet
- Ent SDocument5 pagesEnt S76zw5n4pppNo ratings yet
- NOSE MCQs Points Rida Naqvi-1Document2 pagesNOSE MCQs Points Rida Naqvi-1saifsaffa2No ratings yet
- ENT Reviewer PDFDocument11 pagesENT Reviewer PDFMelissa Joy DollagaNo ratings yet
- Microorganisms and diseasesDocument46 pagesMicroorganisms and diseasesRajanNo ratings yet
- Diseases of the External Nose: Classification, Diagnosis and TreatmentDocument90 pagesDiseases of the External Nose: Classification, Diagnosis and TreatmentKamal Saud100% (2)
- 3-Pharynx. Diseases of HypopharynxDocument34 pages3-Pharynx. Diseases of HypopharynxislamNo ratings yet
- Ent MBBS NotesDocument23 pagesEnt MBBS NotesDr.Riashat azimNo ratings yet
- Nasopharyngeal Carcinoma (NPC) Anatomical ConsiderationsDocument5 pagesNasopharyngeal Carcinoma (NPC) Anatomical ConsiderationsAmy KochNo ratings yet
- Medicine June 2009: Fcps Part1 Q BankDocument14 pagesMedicine June 2009: Fcps Part1 Q Bankqudsia_niaziNo ratings yet
- MCQs on Anatomy of Oral Cavity & PharynxDocument88 pagesMCQs on Anatomy of Oral Cavity & Pharynxsidsudp75% (4)
- Board Revision2014 2Document8 pagesBoard Revision2014 2Adham Sharaf AldeenNo ratings yet
- April RQ CompleteDocument99 pagesApril RQ Completeravi guptaNo ratings yet
- 12 Congenital Lesions of Larynx and Evaluation of StridorDocument77 pages12 Congenital Lesions of Larynx and Evaluation of StridorAbhishek ShahNo ratings yet
- Nasal GranulomasDocument127 pagesNasal GranulomasKamal SaudNo ratings yet
- Upper Respiratory Tract DiseasesDocument34 pagesUpper Respiratory Tract DiseasesSounds of MindNo ratings yet
- Nose Sinus CA Slides 040519Document40 pagesNose Sinus CA Slides 040519AchmadPrihadiantoNo ratings yet
- Ent Mcqs 3Document8 pagesEnt Mcqs 3Uzair KhanNo ratings yet
- ENT Paper 2Document13 pagesENT Paper 2John M. Hemsworth100% (1)
- Juvenile Nasopharyngial AngiofibromaDocument8 pagesJuvenile Nasopharyngial AngiofibromaDr-Firas Nayf Al-ThawabiaNo ratings yet
- Acute Laryngotracheobronchitis (ALTB): Symptoms, Causes and TreatmentDocument53 pagesAcute Laryngotracheobronchitis (ALTB): Symptoms, Causes and TreatmentIhsan HanifNo ratings yet
- Anatomy of the Pharynx and LarynxDocument33 pagesAnatomy of the Pharynx and LarynxFuad AwelNo ratings yet
- Presented By:-Dr. Saqib Majeed Salik Resident Maxillofacial Supervised By: - Dr. Suad A Ahmad Consultant Maxillofacial King Abdullah Hospital BishaDocument53 pagesPresented By:-Dr. Saqib Majeed Salik Resident Maxillofacial Supervised By: - Dr. Suad A Ahmad Consultant Maxillofacial King Abdullah Hospital BishaSaqib Majeed SalikNo ratings yet
- MRCS PART-1 QUESTIONSDocument4 pagesMRCS PART-1 QUESTIONSSalma Esam KambalNo ratings yet
- Larynx MCQSDocument114 pagesLarynx MCQSsidsudp100% (2)
- FRCR 2a March 2010 PapersDocument12 pagesFRCR 2a March 2010 PapersAjay Agarwal100% (2)
- 7 Neck Space InfectionsDocument99 pages7 Neck Space InfectionsAbhishek ShahNo ratings yet
- MCQ Final 1980Document19 pagesMCQ Final 1980JohnSonNo ratings yet
- Orbit Eyelids and Lacrimal SystemDocument6 pagesOrbit Eyelids and Lacrimal SystemZaher Al ObeydNo ratings yet
- Pharynx Lecture 2Document4 pagesPharynx Lecture 2Amy KochNo ratings yet
- India Black Fungus COVID-19 MucormycosisDocument37 pagesIndia Black Fungus COVID-19 MucormycosisSK MOMTAZUL KARIMNo ratings yet
- Skin graft storage timeDocument19 pagesSkin graft storage timeJohnSonNo ratings yet
- Respiratory Medicine Case ReportsDocument3 pagesRespiratory Medicine Case ReportsPororo KewrenNo ratings yet
- Faculty of Medicine Medical Education-Damietta University: Level 1 Semester IIDocument34 pagesFaculty of Medicine Medical Education-Damietta University: Level 1 Semester IISounds of MindNo ratings yet
- Ijoo D 18 00333Document18 pagesIjoo D 18 00333DrKunal KaradeNo ratings yet
- Case Report: A.N Atypical Pathway of Infection in An Adolescent W TH A Deep Neck Space AbscessDocument4 pagesCase Report: A.N Atypical Pathway of Infection in An Adolescent W TH A Deep Neck Space AbscessSisca Rizkia ArifiantiNo ratings yet
- Toacs Fcps Ii: by Maj Atif Najam Mbbs FcpsDocument400 pagesToacs Fcps Ii: by Maj Atif Najam Mbbs FcpsFurqan MirzaNo ratings yet
- ENT Practice MCQs With Key 4th Year MBBSDocument7 pagesENT Practice MCQs With Key 4th Year MBBSPatrick BatemanNo ratings yet
- Chettinad University Previous Year QPs General Surgery CollectionDocument9 pagesChettinad University Previous Year QPs General Surgery CollectionSindhiya DurairajanNo ratings yet
- Ent 25 ExamDocument8 pagesEnt 25 ExamAbd AlsalihiNo ratings yet
- Abses SubmandibularDocument17 pagesAbses Submandibularhoney_hannieNo ratings yet
- Common Facial Vein: Superior Hiatus SemilunarisDocument5 pagesCommon Facial Vein: Superior Hiatus SemilunarissuntiNo ratings yet
- Cutaneous Lymphomas: Unusual Cases 3From EverandCutaneous Lymphomas: Unusual Cases 3Oleg E. AkilovNo ratings yet
- Ear MCQs SummaryDocument6 pagesEar MCQs SummaryÅli Raza ChaudaryNo ratings yet
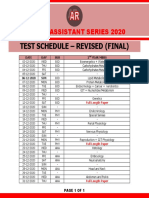
- Test Schedule - Revised (Final) : Medico Assistant Series 2020Document1 pageTest Schedule - Revised (Final) : Medico Assistant Series 2020Åli Raza ChaudaryNo ratings yet
- Pharmacology MCQDocument10 pagesPharmacology MCQNINSIIMA GERALDNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- English 8 in 1 Essays - EditableDocument30 pagesEnglish 8 in 1 Essays - EditableÅli Raza Chaudary100% (1)
- Notsshortquestion12thclassenglish 150211233632 Conversion Gate02Document18 pagesNotsshortquestion12thclassenglish 150211233632 Conversion Gate02aneebaNo ratings yet
- NFPA 97 - 2003 Standard Glossary of Terms Relating To Chimneys, Vents, and Heat-Producing AppliancesDocument34 pagesNFPA 97 - 2003 Standard Glossary of Terms Relating To Chimneys, Vents, and Heat-Producing Appliancesonepunchman yaoNo ratings yet
- Rear Derailleur: Important Notice Names of PartsDocument1 pageRear Derailleur: Important Notice Names of PartsRyan MulyanaNo ratings yet
- School and CentreDocument24 pagesSchool and CentreThrilling PrinceNo ratings yet
- Finasteride 5mg PDFDocument18 pagesFinasteride 5mg PDFddandan_2No ratings yet
- WordsDocument11 pagesWordsAref HoseyniNo ratings yet
- Handling Silica in Cooling WaterDocument17 pagesHandling Silica in Cooling WaterLekhamani YadavNo ratings yet
- Sorogon Medical Mission Group Hospital Operation RecordDocument3 pagesSorogon Medical Mission Group Hospital Operation RecordRoden BerdinNo ratings yet
- APC Symmetra PX-2Document8 pagesAPC Symmetra PX-2drastir_777No ratings yet
- FORM HSE MATRIX TRAINING (Contoh)Document1 pageFORM HSE MATRIX TRAINING (Contoh)Hifni GhazaliNo ratings yet
- Conplast SP430Document2 pagesConplast SP430Tori Small100% (1)
- Bonanza A36 ChecklistDocument10 pagesBonanza A36 Checklistalbucur100% (4)
- The QuestionnaireDocument3 pagesThe QuestionnaireMaximo C. Nayanga Jr.No ratings yet
- The Federal Environmental Protection Authority: May 2004 Addis Ababa EthiopiaDocument44 pagesThe Federal Environmental Protection Authority: May 2004 Addis Ababa Ethiopiayared0% (1)
- 4140DE Data SheetDocument1 page4140DE Data SheetNabeel AmeerNo ratings yet
- Non-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaDocument11 pagesNon-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaPatrícia Felix ÁvilaNo ratings yet
- SpaceX ProposalDocument6 pagesSpaceX ProposalTexas WatchdogNo ratings yet
- Argumentative EssayDocument5 pagesArgumentative Essayapi-538443988No ratings yet
- 3 - 2017 - Superia X 5 StarDocument26 pages3 - 2017 - Superia X 5 Starsomnath serviceNo ratings yet
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)
- 0210 Pop Labels BSDocument1 page0210 Pop Labels BSThe London Free PressNo ratings yet
- Volcanic Eruption Types and ProcessDocument18 pagesVolcanic Eruption Types and ProcessRosemarie Joy TanioNo ratings yet
- Detox 101Document31 pagesDetox 101Botoşanu Diana-LarisaNo ratings yet
- Cambridge O Level: English Language 1123/22Document4 pagesCambridge O Level: English Language 1123/22Shania SeneviratneNo ratings yet
- TDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0Document5 pagesTDI - Full Cave Diver Course: TDI Instructor Manual Part 2 - Diver Standards Date: 12/31/2009 Revision: 10.0BraulioNo ratings yet
- 4 Dec - Elis Vs ElisDocument6 pages4 Dec - Elis Vs ElisRichard TenorioNo ratings yet
- WORKPLACE INSPECTION TECHNIQUES IiaDocument34 pagesWORKPLACE INSPECTION TECHNIQUES IiatewodrosNo ratings yet
- A Study To Assess The Knowledge of Antenatal Mothers Regarding Selected Minor Disorders Affecting PregnancyDocument4 pagesA Study To Assess The Knowledge of Antenatal Mothers Regarding Selected Minor Disorders Affecting PregnancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Strange ICA Stones of PeruDocument31 pagesThe Strange ICA Stones of PeruRoman Aleshkevich100% (1)
- Understanding Immunomodulatory DrugsDocument4 pagesUnderstanding Immunomodulatory DrugsMark Russel Sean LealNo ratings yet
- Payroll Accounting 2015 1st Edition Landin Test Bank 1Document106 pagesPayroll Accounting 2015 1st Edition Landin Test Bank 1dorothy100% (47)