You might also like
- Outline Perioperative NursingDocument8 pagesOutline Perioperative NursingMM VNo ratings yet
- Pharma - SkinDocument8 pagesPharma - Skinreference books100% (1)
- Surgical Instruments GuideDocument70 pagesSurgical Instruments Guidewokorow100% (1)
- Fmge Dec 2019: QuestionsDocument16 pagesFmge Dec 2019: QuestionsSUBHADIPNo ratings yet
- Virginia Satir - Conjoint Family Therapy-Science and Behavior Books (1983)Document310 pagesVirginia Satir - Conjoint Family Therapy-Science and Behavior Books (1983)Klinik Psikologi RSBSNo ratings yet
- Otic and Ophthalmic Agents Guide for Community Pharmacy InternsDocument46 pagesOtic and Ophthalmic Agents Guide for Community Pharmacy InternsAlyssa Leonor NabutasNo ratings yet
- Drug Used in Orthopedic ConditionsDocument105 pagesDrug Used in Orthopedic ConditionsnavenNo ratings yet
- Bites, Stings, and Marine InjuriesDocument61 pagesBites, Stings, and Marine InjuriesmadeNo ratings yet
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlNo ratings yet
- Tooth Eruption & Shedding MechanismsDocument18 pagesTooth Eruption & Shedding MechanismsAnamika PandeyNo ratings yet
- Asepsi S: SurgicalDocument47 pagesAsepsi S: Surgicalspongebob27No ratings yet
- Linear Arrangements of DR InstrumentsDocument42 pagesLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- Or Rle 1-1Document23 pagesOr Rle 1-1Jan Federick Bantay100% (1)
- Fracture FinalDocument92 pagesFracture FinalBea SalgadoNo ratings yet
- Health History Documentation Form ChristinaDocument6 pagesHealth History Documentation Form Christinaapi-545542584No ratings yet
- NCM 109 Skills ChecklistDocument8 pagesNCM 109 Skills ChecklistReygine CariñoNo ratings yet
- Fracture: Edfran Jed A. Serino MSN 303Document34 pagesFracture: Edfran Jed A. Serino MSN 303Edfran Jed SerinoNo ratings yet
- Manual or ProceduresDocument26 pagesManual or ProceduresChristine Joy MolinaNo ratings yet
- Test Bank For Psychiatric Mental Health Nursing 1st Edition by PotterDocument38 pagesTest Bank For Psychiatric Mental Health Nursing 1st Edition by Potterlionelhuynhg7cNo ratings yet
- 986 Assessment of New Born NursingDocument91 pages986 Assessment of New Born NursingkrishnaNo ratings yet
- WalkerDocument18 pagesWalkerNini JendeukieNo ratings yet
- Pressuread Ulcer Prevention Master ClassDocument52 pagesPressuread Ulcer Prevention Master ClassMuhd FaiziNo ratings yet
- Annex 4 Donning Removing of Personal Protective Equipments (PPEs)Document2 pagesAnnex 4 Donning Removing of Personal Protective Equipments (PPEs)Khausalya RaniNo ratings yet
- Surgical InfectionsDocument2 pagesSurgical Infectionsjc_sibal13100% (1)
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNo ratings yet
- Final Health AssessmentDocument7 pagesFinal Health Assessmentapi-546355462No ratings yet
- Wound Documentation Tips PDFDocument2 pagesWound Documentation Tips PDFWinnie LiNo ratings yet
- 6 Alterations On Tissue Perfusion Poleno Serrano TajalaDocument18 pages6 Alterations On Tissue Perfusion Poleno Serrano TajalaSophia A. GoNo ratings yet
- Anesthesia Awareness PreventionDocument13 pagesAnesthesia Awareness PreventionsanaNo ratings yet
- Report Topic:: National Botanical Garden of Bangladesh and Bangladesh National ZooDocument7 pagesReport Topic:: National Botanical Garden of Bangladesh and Bangladesh National ZooBishal SahaNo ratings yet
- Infective Endocarditis 4TH (Compatibility Mode)Document14 pagesInfective Endocarditis 4TH (Compatibility Mode)Mohammed Al-KebsiNo ratings yet
- Learning Objectives: Nursing Skills & Concepts P1of5Document5 pagesLearning Objectives: Nursing Skills & Concepts P1of5rizza_servandoNo ratings yet
- Mamiek Dwi Putro Departemen / SMF Ilmu Bedah FK Unair / RSU DR Soetomo SurabayaDocument38 pagesMamiek Dwi Putro Departemen / SMF Ilmu Bedah FK Unair / RSU DR Soetomo SurabayamasmblinkNo ratings yet
- Postoperative Nursing CareDocument2 pagesPostoperative Nursing CareYeana AlonNo ratings yet
- Orthopedic Problem and ManagementDocument42 pagesOrthopedic Problem and Managementjosephabram051590No ratings yet
- RLE FAMILY REVIEWDocument22 pagesRLE FAMILY REVIEWEniamrahs DnalonNo ratings yet
- Angelica M.docx LFD 18Document2 pagesAngelica M.docx LFD 18Angelica Malacay RevilNo ratings yet
- Medical Ethics in The Operating RoomDocument63 pagesMedical Ethics in The Operating Roomibheng50% (2)
- Movie AwakeDocument7 pagesMovie AwakemefacostaNo ratings yet
- Musculoskeletal System Musculoskeletal System: A. SkeletonDocument23 pagesMusculoskeletal System Musculoskeletal System: A. SkeletonTina TalmadgeNo ratings yet
- Nursing KardexDocument3 pagesNursing KardexLouie Siazon VasquezNo ratings yet
- Nursing Ethics GuideDocument56 pagesNursing Ethics GuideRahmad WijayaNo ratings yet
- Skills Check ListDocument4 pagesSkills Check Listapi-301335830No ratings yet
- Aseptic Technique: Technical Skills Core CurriculumDocument44 pagesAseptic Technique: Technical Skills Core CurriculumAbby GailNo ratings yet
- Perioperative Nursing Care OverviewDocument88 pagesPerioperative Nursing Care Overviewdaljit chahalNo ratings yet
- Perioperative Nursing Module 1Document169 pagesPerioperative Nursing Module 1fleur harrisonNo ratings yet
- Chapter 23 Admitting and Discharging PatientsDocument34 pagesChapter 23 Admitting and Discharging PatientsCarl Dominique De GuzmanNo ratings yet
- In The Name of Allah, The Most Beneficent and MercifulDocument35 pagesIn The Name of Allah, The Most Beneficent and MercifulAhmedMenshawyNo ratings yet
- Sports Injuries and First 2014-1-1-1Document19 pagesSports Injuries and First 2014-1-1-1Twiligh MONo ratings yet
- IncisionDocument6 pagesIncisionMrTwice Templeros0% (1)
- Exam NCM-Lec DemoDocument8 pagesExam NCM-Lec DemoNina OaipNo ratings yet
- Emergency and Disaster NursingDocument8 pagesEmergency and Disaster NursingMiah SubingsubingNo ratings yet
- CWTS Group 5 - Learning Exercises 1 & 2Document4 pagesCWTS Group 5 - Learning Exercises 1 & 2Marjie VistaNo ratings yet
- Activity 1: Full Name: Subject: Evidence Based Nursing General QuestionDocument1 pageActivity 1: Full Name: Subject: Evidence Based Nursing General QuestionYessamin Paith RoderosNo ratings yet
- Family Nursing Care Plan for a Diabetic ClientDocument12 pagesFamily Nursing Care Plan for a Diabetic ClientChristi MilanNo ratings yet
- Pre-Lecture I. You Are The Provider: Chapter 4: Lifting and Moving PatientsDocument9 pagesPre-Lecture I. You Are The Provider: Chapter 4: Lifting and Moving PatientsJasonJejametNo ratings yet
- Operating Room Personnels and Their Functions: Classification of OR TeamDocument3 pagesOperating Room Personnels and Their Functions: Classification of OR TeamRona PieNo ratings yet
- Wound Closure Methods: Sutures vs TapesDocument5 pagesWound Closure Methods: Sutures vs TapesINSANE LEO GAMINGNo ratings yet
- Im BasketballDocument56 pagesIm BasketballCj SernaNo ratings yet
- Pace Partnership Wound Care ProtocolDocument5 pagesPace Partnership Wound Care ProtocolAmmar AlnajjarNo ratings yet
- Dressings and DrainsDocument118 pagesDressings and DrainsBhanu PraseedhaNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Hysterectomy Types and Procedures ExplainedDocument18 pagesHysterectomy Types and Procedures ExplainedMa. Louise Lovely RosalesNo ratings yet
- Questions and Rationale 2Document152 pagesQuestions and Rationale 2Ma. Louise Lovely RosalesNo ratings yet
- RespirationDocument5 pagesRespirationMa. Louise Lovely RosalesNo ratings yet
- HematologyDocument4 pagesHematologyMa. Louise Lovely RosalesNo ratings yet
- Communicable DiseaseDocument18 pagesCommunicable DiseaseMa. Louise Lovely RosalesNo ratings yet
- RespirationDocument5 pagesRespirationMa. Louise Lovely RosalesNo ratings yet
- HematologyDocument4 pagesHematologyMa. Louise Lovely RosalesNo ratings yet
- Prueba 2Document188 pagesPrueba 2David LiNo ratings yet
- Logic Models To Enhance Program PerformanceDocument32 pagesLogic Models To Enhance Program PerformanceCitra ManikNo ratings yet
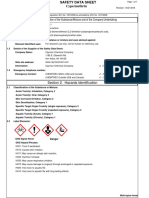
- Material Safety Data Sheet Cypermethrin PDFDocument7 pagesMaterial Safety Data Sheet Cypermethrin PDFSaid Muchsin AlkaffNo ratings yet
- MDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Document13 pagesMDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Clarabelle Mae Dela RosaNo ratings yet
- Proklenz One - MSDSDocument2 pagesProklenz One - MSDSneoNo ratings yet
- Early Metabolic Programming - 1 - InfantNutrition - B.Koletzko PDFDocument10 pagesEarly Metabolic Programming - 1 - InfantNutrition - B.Koletzko PDFAnnie RealNo ratings yet
- Poverty: The Worst Form of ViolenceDocument19 pagesPoverty: The Worst Form of Violencesraboni ahamedNo ratings yet
- Week10 Eth LMDocument8 pagesWeek10 Eth LMRenievave Torculas100% (2)
- LifeextensionDocument84 pagesLifeextensionhermestriNo ratings yet
- Star Extra Protect BrochureDocument5 pagesStar Extra Protect BrochurebhuviNo ratings yet
- OmniTurn Manual g3Document210 pagesOmniTurn Manual g3CESAR MTZNo ratings yet
- BULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14Document6 pagesBULLDOZER - C52JSA-037 - Dozer Clearing of Existing Tracks in Jebel - 18-Mar-14hechame TamerhouletNo ratings yet
- SDS-Dolphin Screen WashDocument10 pagesSDS-Dolphin Screen WashLiz CNo ratings yet
- Teachers Perception of Factors Affecting School DropoutsDocument53 pagesTeachers Perception of Factors Affecting School DropoutsIchipi-ifukor Patrick Chukuyenum100% (1)
- Plastic Surgery ConferenceDocument1 pagePlastic Surgery Conferenceretno widyastutiNo ratings yet
- Tulajabahvani StotrDocument2 pagesTulajabahvani StotrHema DhaneNo ratings yet
- CounterclaimsDocument3 pagesCounterclaimsRuthie PatootieNo ratings yet
- Portfolio Midpoint FeedbackDocument4 pagesPortfolio Midpoint Feedbackapi-587439953No ratings yet
- Code of Ethics-American Counseling AssociationDocument51 pagesCode of Ethics-American Counseling AssociationJohn Carlo PerezNo ratings yet
- Weekly Home Learning Plan For Grade 7 MAPEH 7 Quarter IVDocument10 pagesWeekly Home Learning Plan For Grade 7 MAPEH 7 Quarter IVMiguilaMaldita GamasNo ratings yet
- 1.the Winners Cup PWSDocument4 pages1.the Winners Cup PWSarunimafunnygirl12No ratings yet
- Mapeh 10 Curriculum MapDocument9 pagesMapeh 10 Curriculum MapJoshua LamzonNo ratings yet
- Chapter 6. Operation: Before Operation, Prepare The Ventilator As Instructed inDocument18 pagesChapter 6. Operation: Before Operation, Prepare The Ventilator As Instructed indeboraNo ratings yet
- NAME: Sarah Mae R. Areglado Section: G12 Humss Silang SUBJECT: Understanding Culture, Society and PoliticsDocument6 pagesNAME: Sarah Mae R. Areglado Section: G12 Humss Silang SUBJECT: Understanding Culture, Society and PoliticsEsmen Areglado0% (1)
- Issue Brief NPNRSDocument1 pageIssue Brief NPNRSKristin Villaseñor-MercadoNo ratings yet
- OSHC Guide: Support When Studying AbroadDocument12 pagesOSHC Guide: Support When Studying AbroadIgnacio CorreaNo ratings yet
- Ronald R. Martel Celebrated As A Professional of The Year For 2022 by Strathmore's Who's Who Worldwide PublicationDocument4 pagesRonald R. Martel Celebrated As A Professional of The Year For 2022 by Strathmore's Who's Who Worldwide PublicationPR.comNo ratings yet