You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Nutritional Support in Critically Ill PatientDocument42 pagesNutritional Support in Critically Ill PatientPema Dolma Tamang100% (1)
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Advances in Surgical NutritionDocument42 pagesAdvances in Surgical NutritionpratoshNo ratings yet
- Ketogenic Diet "Yes & No" Guide For BeginnersFrom EverandKetogenic Diet "Yes & No" Guide For BeginnersRating: 3 out of 5 stars3/5 (1)
- Total Parenteral NutritionDocument9 pagesTotal Parenteral NutritionUday Kumar100% (1)
- Fix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsFrom EverandFix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsNo ratings yet
- Final Case Study PresentationDocument31 pagesFinal Case Study Presentationapi-546555350No ratings yet
- Nutrition Support Surgical PatientsDocument35 pagesNutrition Support Surgical PatientsFuad Aman AbjNo ratings yet
- Surgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DDocument33 pagesSurgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DLilibeth Tenorio De Leon100% (1)
- NZR TPN PrabuDocument56 pagesNZR TPN PrabuikesesariaNo ratings yet
- NutritionDocument22 pagesNutritionMira ManoharanNo ratings yet
- IV-B Total Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) / Mechanical VentilatorDocument23 pagesIV-B Total Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) / Mechanical VentilatorRio DanteNo ratings yet
- Enteral Nutrition: Agus PrastowoDocument49 pagesEnteral Nutrition: Agus Prastowokartika sariNo ratings yet
- Chapter 15 - EN and PNDocument38 pagesChapter 15 - EN and PNAmani KayedNo ratings yet
- Lecture 2 - TPNDocument54 pagesLecture 2 - TPNDian zaini PutraNo ratings yet
- For The Surgical Patient: Kelly Sparks LDN, RDDocument47 pagesFor The Surgical Patient: Kelly Sparks LDN, RDManikandaprabhu sivaNo ratings yet
- Parenteral NutritionDocument49 pagesParenteral NutritionPeace Andong PerochoNo ratings yet
- Nuciție Parențială TotalăDocument3 pagesNuciție Parențială TotalăAurelia AlexandraNo ratings yet
- RTD Otsuka Parenteral NutritionDocument39 pagesRTD Otsuka Parenteral NutritionMuhammad IqbalNo ratings yet
- Nutrition: - . - and The Surgical PatientDocument39 pagesNutrition: - . - and The Surgical PatientJan Cyrill YuNo ratings yet
- Nutrition in IcuDocument31 pagesNutrition in IcuShni khan100% (4)
- Surgical Nutrition, Lecture NoteDocument65 pagesSurgical Nutrition, Lecture Notea12345644321No ratings yet
- Nutrition Support in The Hospital Patient: David Armstrong November 2, 2005Document40 pagesNutrition Support in The Hospital Patient: David Armstrong November 2, 2005Larasati HasaptiasNo ratings yet
- Nutrition Support: Sean P Harbison MDDocument42 pagesNutrition Support: Sean P Harbison MDsgod34No ratings yet
- TPN 1 UpdatedDocument13 pagesTPN 1 Updatedathijasafraan1997No ratings yet
- Total Parenteral Nutrition Guideline-4 - 2Document38 pagesTotal Parenteral Nutrition Guideline-4 - 2FirnandaNo ratings yet
- Assignment On TPNDocument14 pagesAssignment On TPNBhawna Joshi100% (8)
- NHS guidelines prevent refeeding syndromeDocument5 pagesNHS guidelines prevent refeeding syndromePejman AhmadiNo ratings yet
- Enteral NutritionDocument73 pagesEnteral NutritionYosep SutandarNo ratings yet
- TPN ClassDocument32 pagesTPN Classgamal attamNo ratings yet
- (Reed Henry) Total Parenteral NutritionDocument42 pages(Reed Henry) Total Parenteral NutritionEveLyn PRadanaNo ratings yet
- Slides Malnutrition FINALDocument50 pagesSlides Malnutrition FINALwa2nagungpNo ratings yet
- Total Parenteral Nutrition Guideline-4 - 2Document38 pagesTotal Parenteral Nutrition Guideline-4 - 2Henry M. BarberenaNo ratings yet
- Case StudyDocument5 pagesCase Studyapi-247850107No ratings yet
- Nutrition in The Surgical PatientDocument35 pagesNutrition in The Surgical PatientUsaid SulaimanNo ratings yet
- Exam 4 NOTESDocument20 pagesExam 4 NOTESDoctorDrapionNo ratings yet
- BMT Total Parenteral NutritionDocument5 pagesBMT Total Parenteral NutritionDuwii CinutNo ratings yet
- Nutrition in ICU PatientsDocument50 pagesNutrition in ICU PatientsNurulain MD AnuarNo ratings yet
- Total Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) - Mechinal VentilatorDocument23 pagesTotal Parenteral Nutrition (TPN) and Central Venous Pressure Line (CVP) - Mechinal VentilatorErika Danalle ArceoNo ratings yet
- Total Parenteral NutritionDocument59 pagesTotal Parenteral NutritionMARIAH ALEXIE GASALNo ratings yet
- Parenteral NutritionDocument6 pagesParenteral NutritionAngela NeriNo ratings yet
- 1.CBE CME Obstructive JaundiceDocument39 pages1.CBE CME Obstructive JaundicedeepikaNo ratings yet
- Nutrition PostoperativeDocument47 pagesNutrition PostoperativeAnonymous 86gki5No ratings yet
- Parenteral NutritionDocument47 pagesParenteral Nutritionalishba100% (2)
- Nutrisi Parenteral - EmaDocument51 pagesNutrisi Parenteral - EmaVu Nguyen NguyenNo ratings yet
- Nutrisi Parenteral - EmaDocument51 pagesNutrisi Parenteral - EmaVu Nguyen NguyenNo ratings yet
- Total Parenteral NutritionDocument41 pagesTotal Parenteral Nutritionrana adnan ejaz100% (3)
- Nutrition in Sick PatientsDocument50 pagesNutrition in Sick PatientsIbnu ZakiNo ratings yet
- Use of The Modified Atkins Diet in Intractable SEIZURESDocument30 pagesUse of The Modified Atkins Diet in Intractable SEIZURESDr-Ajay TripathiNo ratings yet
- Pocket Card Parenteral Nutrition February 2021Document5 pagesPocket Card Parenteral Nutrition February 2021Kouba MarciminiNo ratings yet
- Nutrition in SurgeryDocument29 pagesNutrition in SurgeryAfifah JaafarNo ratings yet
- Nutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)Document58 pagesNutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)SanaSofiyahNo ratings yet
- Enteral Nutrition GuideDocument38 pagesEnteral Nutrition GuideWidi Alya ZhafiraNo ratings yet
- Entral NutritionDocument73 pagesEntral NutritionAmr OthmanNo ratings yet
- Glycemic control in hospitalized patientsDocument31 pagesGlycemic control in hospitalized patientsahmed_g_salihNo ratings yet
- Total Parenteral Nutrition: Feeding IntravenouslyDocument5 pagesTotal Parenteral Nutrition: Feeding IntravenouslyjulieNo ratings yet
- Parental Nutrition TherapyDocument52 pagesParental Nutrition Therapysamarshahab320No ratings yet
- Nutritional TherapyDocument16 pagesNutritional TherapymahanayakakashNo ratings yet
- Nutritional phy-WPS OfficeDocument5 pagesNutritional phy-WPS OfficeAkachukwu ObunikeNo ratings yet
- CS6 Alzheimer's Disease Drug StudyDocument3 pagesCS6 Alzheimer's Disease Drug StudyAudrie Allyson GabalesNo ratings yet
- 3rd Year Nursing MS LEC MIDTERM QUIZESDocument18 pages3rd Year Nursing MS LEC MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- 3F Gabales, Audrie Allyson - Synchronous Class Lec 6 ActivityDocument1 page3F Gabales, Audrie Allyson - Synchronous Class Lec 6 ActivityAudrie Allyson GabalesNo ratings yet
- 3rd Year Nursing RESEARCH MIDTERM QUIZESDocument3 pages3rd Year Nursing RESEARCH MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- 3rd Year Nursing MIDTERM MS QUIZ 5-6 NotesDocument13 pages3rd Year Nursing MIDTERM MS QUIZ 5-6 NotesAudrie Allyson GabalesNo ratings yet
- Surgical Gowning and GlovingDocument36 pagesSurgical Gowning and GlovingAudrie Allyson GabalesNo ratings yet
- Diagnostic Prodecures X Ray Utz CT Scan MriecgeegDocument42 pagesDiagnostic Prodecures X Ray Utz CT Scan MriecgeegAudrie Allyson GabalesNo ratings yet
- Breast Self ExaminationDocument81 pagesBreast Self ExaminationAudrie Allyson Gabales100% (1)
- CS6 Alzheimer DiseaseDocument21 pagesCS6 Alzheimer DiseaseAudrie Allyson GabalesNo ratings yet
- CS7 pt1Document4 pagesCS7 pt1Audrie Allyson GabalesNo ratings yet
- Sensitivity Test Checks To See What Kind ofDocument5 pagesSensitivity Test Checks To See What Kind ofAudrie Allyson GabalesNo ratings yet
- Armada Past and Present Medical HistoryDocument1 pageArmada Past and Present Medical HistoryAudrie Allyson GabalesNo ratings yet
- Drug Study HIVDocument10 pagesDrug Study HIVAudrie Allyson GabalesNo ratings yet
- Cervical - Pap SmearDocument17 pagesCervical - Pap SmearAudrie Allyson GabalesNo ratings yet
- Safe Handling of Hazardous MedicationsDocument54 pagesSafe Handling of Hazardous MedicationsAudrie Allyson GabalesNo ratings yet
- 3F CS7 CRF Gabales, Audrie Allyson H.Document25 pages3F CS7 CRF Gabales, Audrie Allyson H.Audrie Allyson GabalesNo ratings yet
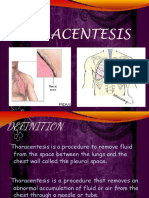
- Thoracentesis - ParacentesisDocument62 pagesThoracentesis - ParacentesisAudrie Allyson GabalesNo ratings yet
- CS10 HIV PathophysiologyDocument2 pagesCS10 HIV PathophysiologyAudrie Allyson GabalesNo ratings yet
- CASE-10-Drug StudyDocument7 pagesCASE-10-Drug StudyAudrie Allyson GabalesNo ratings yet
- Azithromycin Drug Classification, Indications, Side Effects & Nursing ResponsibilitiesDocument17 pagesAzithromycin Drug Classification, Indications, Side Effects & Nursing ResponsibilitiesAudrie Allyson GabalesNo ratings yet
- Aag Drug StudyDocument7 pagesAag Drug StudyAudrie Allyson GabalesNo ratings yet
- Cs8 Intro, ObjDocument1 pageCs8 Intro, ObjAudrie Allyson GabalesNo ratings yet
- RES MIDTERM Master NotesDocument168 pagesRES MIDTERM Master NotesAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer DRUG STUDYDocument12 pagesColorectal Cancer DRUG STUDYAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer Diagnostic LabsDocument1 pageColorectal Cancer Diagnostic LabsAudrie Allyson GabalesNo ratings yet
- CS11 TYPHOID FEVER PathophysiologyDocument1 pageCS11 TYPHOID FEVER PathophysiologyAudrie Allyson GabalesNo ratings yet
- DISCHARGE PLAN & RRL For Colorectal CancerDocument2 pagesDISCHARGE PLAN & RRL For Colorectal CancerAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer Patient DataDocument3 pagesColorectal Cancer Patient DataAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer NCPDocument6 pagesColorectal Cancer NCPAudrie Allyson GabalesNo ratings yet
- Introduction To Qualitative Research MethodsDocument3 pagesIntroduction To Qualitative Research MethodsAudrie Allyson GabalesNo ratings yet
- A Beginners Guide Sap Smart FormsDocument61 pagesA Beginners Guide Sap Smart FormsMuhammad ZeeshanNo ratings yet
- My CV - Rose ChebetDocument5 pagesMy CV - Rose ChebetSammy WatimaNo ratings yet
- Ffective Riting Kills: Training & Discussion OnDocument37 pagesFfective Riting Kills: Training & Discussion OnKasi ReddyNo ratings yet
- S7 - Q2 - Answer KeyDocument11 pagesS7 - Q2 - Answer KeyRaniel LacuarinNo ratings yet
- 6.4 Permutations and CombinationsDocument14 pages6.4 Permutations and CombinationsAns SembiringNo ratings yet
- Secu Gen Hamster Pro 20Document2 pagesSecu Gen Hamster Pro 20Ashish GusainNo ratings yet
- Carbon Emission and Battery Monitoring SystemDocument17 pagesCarbon Emission and Battery Monitoring SystemIJRASETPublicationsNo ratings yet
- Developing Website Information ArchitectureDocument39 pagesDeveloping Website Information ArchitectureBizuNo ratings yet
- Mark Dyczkowski and Trika Journal March 2015 Vol.1.No.1.Document10 pagesMark Dyczkowski and Trika Journal March 2015 Vol.1.No.1.Mark Dyczkoswki and Trika Journal100% (2)
- Chapter (3) Simple Stresses in Machine Parts: Design of Machine Elements I (ME-41031)Document80 pagesChapter (3) Simple Stresses in Machine Parts: Design of Machine Elements I (ME-41031)Dr. Aung Ko LattNo ratings yet
- ErgonomicsDocument15 pagesErgonomicsdtmNo ratings yet
- Economics of Power GenerationDocument32 pagesEconomics of Power GenerationKimberly Jade VillaganasNo ratings yet
- Ceftriaxone R Salmonella Typhi 02Document8 pagesCeftriaxone R Salmonella Typhi 02docsumitraiNo ratings yet
- Binh Dien Fertilizer Joint Stock CompanyDocument11 pagesBinh Dien Fertilizer Joint Stock CompanyHuynh Minh Quan B2014431No ratings yet
- The Secret Science of Shaktipat - Guide To Initiation 13 September 2020Document77 pagesThe Secret Science of Shaktipat - Guide To Initiation 13 September 2020Patrick JenksNo ratings yet
- IruvarDocument5 pagesIruvarKarthikeya KaredlaNo ratings yet
- Avelino Vs Cuenco (Case Digest)Document8 pagesAvelino Vs Cuenco (Case Digest)Christopher Dale WeigelNo ratings yet
- Combining Singing and PsycologyDocument6 pagesCombining Singing and PsycologyAna luciaNo ratings yet
- Pizza Hut Final!Document15 pagesPizza Hut Final!Alisha ParabNo ratings yet
- Petol Ps 460-5G: Technical SheetDocument2 pagesPetol Ps 460-5G: Technical SheetA MahmoodNo ratings yet
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet
- GCS Activity 2003Document33 pagesGCS Activity 2003donnottryNo ratings yet
- Man 400eDocument324 pagesMan 400eLopez Tonny100% (1)
- Data Structures and Algorithms in Java ™: Sixth EditionDocument8 pagesData Structures and Algorithms in Java ™: Sixth EditionIván Bartulin Ortiz0% (1)
- String inverter comparisonDocument4 pagesString inverter comparisonRakesh HateyNo ratings yet
- AAPD Reference Manual - Pediatric Dentistry 2010-2011Document336 pagesAAPD Reference Manual - Pediatric Dentistry 2010-2011Tiara100% (1)
- MsdsDocument6 pagesMsdsGis GeorgeNo ratings yet
- Sop For FatDocument6 pagesSop For Fatahmed ismailNo ratings yet
- Java syntax and data types tutorialDocument3 pagesJava syntax and data types tutorialpeter chan100% (1)
- G.raju Reddy Resume (PDF1) PDFDocument3 pagesG.raju Reddy Resume (PDF1) PDFanon_708469687No ratings yet