You might also like
- Sensibilizacion Central 2020 JosptDocument8 pagesSensibilizacion Central 2020 JosptVictor Andrés Olivares IbarraNo ratings yet
- Lee 2019Document11 pagesLee 2019RashidkpvldNo ratings yet
- 1472 6882 2 9 PDFDocument8 pages1472 6882 2 9 PDFThiago NunesNo ratings yet
- Mojap 05 00232Document9 pagesMojap 05 00232Fasha Since AndampuryNo ratings yet
- Spinal Reflex Therapy & Spinal Reflex Analysis: Evidence BasedDocument2 pagesSpinal Reflex Therapy & Spinal Reflex Analysis: Evidence BasedMonikaNo ratings yet
- Low Back Neck Pain Paper JBMTDocument8 pagesLow Back Neck Pain Paper JBMTMariusz IdzikowskiNo ratings yet
- Neural Mobilization: The Impossible: RichardDocument3 pagesNeural Mobilization: The Impossible: Richardsonali soumyashreeNo ratings yet
- Pelatihan Dry Needle 2022-CourseDocument115 pagesPelatihan Dry Needle 2022-CoursebonangNo ratings yet
- Spinal Injury Nursing Care PlanDocument2 pagesSpinal Injury Nursing Care PlanPatricia OrtegaNo ratings yet
- Pelosin 2013Document10 pagesPelosin 2013QuocNo ratings yet
- Edizioni InternazionaliDocument1 pageEdizioni InternazionaliJefferson EvairNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleLUIZANo ratings yet
- Magnetic Compare To EsDocument4 pagesMagnetic Compare To EsNakarit SangsirinawinNo ratings yet
- A Review of Non-Invasive Sensory FeedbackDocument25 pagesA Review of Non-Invasive Sensory Feedbackrazankhalife4No ratings yet
- Recent Advancement in The Field of Physiotherapy: February 2013Document6 pagesRecent Advancement in The Field of Physiotherapy: February 2013R HariNo ratings yet
- EEG Analysis During Active and Assisted Repetitive Movements Evidence For Differences in Neural EngagementDocument11 pagesEEG Analysis During Active and Assisted Repetitive Movements Evidence For Differences in Neural EngagementWarnithaNo ratings yet
- The Associated Factors and Clinical Features Of.10Document7 pagesThe Associated Factors and Clinical Features Of.10Vinay VivekNo ratings yet
- Spinal Manipulative Therapy and Somatosensory ActivationDocument21 pagesSpinal Manipulative Therapy and Somatosensory ActivationAlan KipperNo ratings yet
- Pelatihan Dry NeedleDocument101 pagesPelatihan Dry NeedleAri SudarsonoNo ratings yet
- 2055668319827466Document23 pages2055668319827466MOVEMENT SCHOOLNo ratings yet
- Effectiveness of Repetitive Magnetic Stimulation IDocument4 pagesEffectiveness of Repetitive Magnetic Stimulation I29kgcfgqw4No ratings yet
- Rsi Presentation HandoutDocument2 pagesRsi Presentation Handoutapi-518621879No ratings yet
- MERKLE - The Interaction Between Pain and Movement PDFDocument15 pagesMERKLE - The Interaction Between Pain and Movement PDFAna PaulaNo ratings yet
- IJHSRUN CaseReportDocument5 pagesIJHSRUN CaseReportIndah YulantariNo ratings yet
- Musculoskeletal EMF TreatmentDocument16 pagesMusculoskeletal EMF Treatmentdrmarwayaseen85No ratings yet
- Kristjansson 2009Document14 pagesKristjansson 2009AdosotoNo ratings yet
- Paper Positional Release Technique SF MWDocument17 pagesPaper Positional Release Technique SF MWkamNo ratings yet
- Different Exercise Endurance ModalitiesDocument14 pagesDifferent Exercise Endurance ModalitiesGabriel CostaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Vas 1Document10 pagesVas 1Abdul Latiful KhabirNo ratings yet
- Home Rehabilitation System For The Upper ExtremityDocument4 pagesHome Rehabilitation System For The Upper ExtremityAnh HuyNo ratings yet
- Fneur 14 1104817Document6 pagesFneur 14 1104817geowalker7092No ratings yet
- Pain Exposure Physical Therapy (PEPT) in Complex Regional Pain Syndrome Type 1: A Systematic ReviewDocument8 pagesPain Exposure Physical Therapy (PEPT) in Complex Regional Pain Syndrome Type 1: A Systematic ReviewSabrina JonesNo ratings yet
- What Is Palpation Osteo BrochureDocument3 pagesWhat Is Palpation Osteo Brochureapi-614224428No ratings yet
- Spinal Electroacupuncture PDFDocument7 pagesSpinal Electroacupuncture PDFAngela Pagliuso100% (2)
- 2015 Nociception, Pain, Negative Moods, and Behavior SelectionDocument18 pages2015 Nociception, Pain, Negative Moods, and Behavior SelectionCristian OyarzoNo ratings yet
- Joint Mobilization EnhancesDocument12 pagesJoint Mobilization EnhancesDavid BrunoNo ratings yet
- Psychology of Sport & Exercise: Full Length ArticleDocument9 pagesPsychology of Sport & Exercise: Full Length ArticleShyamali Kaushalya FernandoNo ratings yet
- The Modulation of Neural Insular Activity by A BraDocument12 pagesThe Modulation of Neural Insular Activity by A BraCletto ArrighiNo ratings yet
- The Role of Physical Exercise and Rehabilitative Implications in The Process of Nerve Repair in Peripheral Neuropathies A Systematic ReviewDocument29 pagesThe Role of Physical Exercise and Rehabilitative Implications in The Process of Nerve Repair in Peripheral Neuropathies A Systematic ReviewMirko GrausoNo ratings yet
- Effect of The Neuromuscular Taping (NMT) Towards Flexibility Muscle Functions at The Lower Back and HamstringsDocument3 pagesEffect of The Neuromuscular Taping (NMT) Towards Flexibility Muscle Functions at The Lower Back and HamstringsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal KedokteranDocument6 pagesJurnal KedokteranFatimatus Zahroh IchsanNo ratings yet
- Mens and TensDocument4 pagesMens and TensRiri NandaNo ratings yet
- Eenm No Idoso Crítico - 2022Document9 pagesEenm No Idoso Crítico - 2022Edgard SantosNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- Muscle Motor Point Identification Is Essential For Optimizing Neuromuscular Electrical Stimulation UseDocument6 pagesMuscle Motor Point Identification Is Essential For Optimizing Neuromuscular Electrical Stimulation UsestefanoNo ratings yet
- Dry Needling (Workshop Fisiofit 2016)Document119 pagesDry Needling (Workshop Fisiofit 2016)Laode Iski IsmailNo ratings yet
- 1.repetitive Peripheral Magnetic Stimulation As Pain Management Solution in Musculoskeletal and Neurological DisordersDocument5 pages1.repetitive Peripheral Magnetic Stimulation As Pain Management Solution in Musculoskeletal and Neurological Disordersf.mariajdbNo ratings yet
- Pas Chos 2013Document6 pagesPas Chos 2013Hari25885No ratings yet
- All For Nov 14 Presentation FinalDocument13 pagesAll For Nov 14 Presentation FinalKristine JamilleNo ratings yet
- Mobilization and Stimulation of Neuromuscular Tissue (MaSoNT)From EverandMobilization and Stimulation of Neuromuscular Tissue (MaSoNT)No ratings yet
- Modulation of Exteroceptive Electromyographic Responses in Defensive Peripersonal SpaceDocument14 pagesModulation of Exteroceptive Electromyographic Responses in Defensive Peripersonal SpaceGogy MarkNo ratings yet
- Chalchat Et Al. 2022Document15 pagesChalchat Et Al. 2022Fábio LanferdiniNo ratings yet
- The Anatomy and Physiology of Pain: Basic ScienceDocument5 pagesThe Anatomy and Physiology of Pain: Basic ScienceAsti DwiningsihNo ratings yet
- NCP-Acute Postpartum Perineal PainDocument2 pagesNCP-Acute Postpartum Perineal PainFrenzylane Diane CoralNo ratings yet
- Active Scars Lewitt 2004 PDFDocument4 pagesActive Scars Lewitt 2004 PDFpfi_jenNo ratings yet
- Adjuvant Treatments Associated With Botulinum Toxin Injection For Managing Spasticity: An Overview of The LiteratureDocument6 pagesAdjuvant Treatments Associated With Botulinum Toxin Injection For Managing Spasticity: An Overview of The LiteratureManuela Gómez GutiérrezNo ratings yet
- Neuromuscular Taping For The Upper LimbDocument4 pagesNeuromuscular Taping For The Upper LimbFayza RihastaraNo ratings yet
- Introduction To Neuro Rehabilitation and Restorative Neurology (Article) Author Milan R DimitrijevicDocument3 pagesIntroduction To Neuro Rehabilitation and Restorative Neurology (Article) Author Milan R DimitrijevicPredrag NikolicNo ratings yet
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodFrom EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaNo ratings yet
- Materi PIR - Dr. Imam Subadi, SP - KFR-K Cellular Adaption in Exercise Movement and Exercise in Pain ManagementDocument29 pagesMateri PIR - Dr. Imam Subadi, SP - KFR-K Cellular Adaption in Exercise Movement and Exercise in Pain ManagementGhea Putri HendrianiNo ratings yet
- Great Challenges Towards Sports Injury Prevention & Rehabilitation - Prof. Dr. Dr. Angela B. M. Tulaar, SP - KFR (K)Document23 pagesGreat Challenges Towards Sports Injury Prevention & Rehabilitation - Prof. Dr. Dr. Angela B. M. Tulaar, SP - KFR (K)Ghea Putri HendrianiNo ratings yet
- Eur J Heart Fail-2013-Tang-eurjhf-hft082Document9 pagesEur J Heart Fail-2013-Tang-eurjhf-hft082Ghea Putri HendrianiNo ratings yet
- Updated Rehabilitation Management of Lower Extremity Injuries - Dr. Dr. Damayanti Tinduh, SP - KFR (K)Document35 pagesUpdated Rehabilitation Management of Lower Extremity Injuries - Dr. Dr. Damayanti Tinduh, SP - KFR (K)Ghea Putri HendrianiNo ratings yet
- Alat Gigi Ekatalog MeiDocument3 pagesAlat Gigi Ekatalog MeiGhea Putri HendrianiNo ratings yet
- Mater PIR - Dr. Siti Chandra W., SP - KFR-K High Intensity Laser For Post COVID RehabilitationDocument20 pagesMater PIR - Dr. Siti Chandra W., SP - KFR-K High Intensity Laser For Post COVID RehabilitationGhea Putri HendrianiNo ratings yet
- 2015 PDCI Core Kit 3b PERKENI Standards of Medical CareDocument62 pages2015 PDCI Core Kit 3b PERKENI Standards of Medical CareGhea Putri HendrianiNo ratings yet
- Risk Factors For Lower Extremity Injury A Review of The Literature - Dr. Zayadi Zainudin, SP - KFRDocument41 pagesRisk Factors For Lower Extremity Injury A Review of The Literature - Dr. Zayadi Zainudin, SP - KFRGhea Putri HendrianiNo ratings yet
- Materi PIR - Prof. Dr. Dr. Hening Laswati, SP - KFR-K - The Evidence and Molecular Mechanism of Pulmonary FunctionDocument15 pagesMateri PIR - Prof. Dr. Dr. Hening Laswati, SP - KFR-K - The Evidence and Molecular Mechanism of Pulmonary FunctionGhea Putri HendrianiNo ratings yet
- Materi PIR - DR - Dr. Meisy Andriana, SP - KFR-K The Mechanism of Plasticity and Regeneration in The Brain and Spinal CordDocument25 pagesMateri PIR - DR - Dr. Meisy Andriana, SP - KFR-K The Mechanism of Plasticity and Regeneration in The Brain and Spinal CordGhea Putri HendrianiNo ratings yet
- PDF 5. Neuroanatomy-MinDocument6 pagesPDF 5. Neuroanatomy-MinGhea Putri HendrianiNo ratings yet
- Materi PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineDocument30 pagesMateri PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineGhea Putri HendrianiNo ratings yet
- Materi PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineDocument30 pagesMateri PIR - Dr. Lydia Arfianti, SP - KFR-K The Strategies in Rehabilitation of Pathologic Fracture of The SpineGhea Putri HendrianiNo ratings yet
- PDF 6. MOTOR CONTROL-minDocument11 pagesPDF 6. MOTOR CONTROL-minGhea Putri HendrianiNo ratings yet
- Vascular Supply To The BrainDocument38 pagesVascular Supply To The BrainGhea Putri HendrianiNo ratings yet
- Materi PIR - Dr. Norhayati Hussein, MD, Physiatrist Potential Rehabiliation Strategies To Enhance Neuroplasticy Regeneration in Movement RecoveryDocument38 pagesMateri PIR - Dr. Norhayati Hussein, MD, Physiatrist Potential Rehabiliation Strategies To Enhance Neuroplasticy Regeneration in Movement RecoveryGhea Putri HendrianiNo ratings yet
- Materi PIR - DR - Dr. Ratna D. Haryadi, SP - KFR-K Pediatric Exercise SMART Goal For Movement and Therapeutic Exercise in Pediatric RehabilitationDocument25 pagesMateri PIR - DR - Dr. Ratna D. Haryadi, SP - KFR-K Pediatric Exercise SMART Goal For Movement and Therapeutic Exercise in Pediatric RehabilitationGhea Putri HendrianiNo ratings yet
- Anatomi Dan Kinesiologi Shoulder Part 2Document38 pagesAnatomi Dan Kinesiologi Shoulder Part 2denishNo ratings yet
- Anatomi Kinesiologi Pergelangan Kaki Dan KakiDocument38 pagesAnatomi Kinesiologi Pergelangan Kaki Dan KakiGhea Putri HendrianiNo ratings yet
- Materi Dr. Ibrahim Agung, SPKFRDocument30 pagesMateri Dr. Ibrahim Agung, SPKFRGhea Putri HendrianiNo ratings yet
- Materi PIR - Dr. S M Mei Wulan, SP - KFR-K Application of Movement - Therapeutic Exercise in Cerebral PalsyDocument26 pagesMateri PIR - Dr. S M Mei Wulan, SP - KFR-K Application of Movement - Therapeutic Exercise in Cerebral PalsyGhea Putri HendrianiNo ratings yet
- Materi PIR - Dr. Lukas W., SP - OT-K Principles - Biomechanics of Spine Fracture HealingDocument21 pagesMateri PIR - Dr. Lukas W., SP - OT-K Principles - Biomechanics of Spine Fracture HealingGhea Putri HendrianiNo ratings yet
- 3.2 Autonomic Nervous SystemDocument31 pages3.2 Autonomic Nervous SystemyunitaNo ratings yet
- PDF 1.1 Shoulder-MinDocument5 pagesPDF 1.1 Shoulder-MinGhea Putri HendrianiNo ratings yet
- Clinical Parthways Pneumonia Rawat Inap Ruang Intensif RS UNRAMDocument5 pagesClinical Parthways Pneumonia Rawat Inap Ruang Intensif RS UNRAMGhea Putri HendrianiNo ratings yet
- Dr. Ilham OsteoporosisDocument39 pagesDr. Ilham OsteoporosisGhea Putri HendrianiNo ratings yet
- Dr. Ilham OsteoporosisDocument39 pagesDr. Ilham OsteoporosisGhea Putri HendrianiNo ratings yet
- Dr. Kobal Low CarbDocument42 pagesDr. Kobal Low CarbGhea Putri HendrianiNo ratings yet
- Interventional Management in Knee OA PDFDocument29 pagesInterventional Management in Knee OA PDFGhea Putri HendrianiNo ratings yet
- Epithelium Surface SpecializationsDocument41 pagesEpithelium Surface SpecializationsMitzel SapaloNo ratings yet
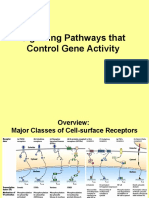
- 16) Signaling Pathways That Control Gene ActivityDocument27 pages16) Signaling Pathways That Control Gene ActivityRNo ratings yet
- Ebook Principles of Tissue Engineering PDF Full Chapter PDFDocument67 pagesEbook Principles of Tissue Engineering PDF Full Chapter PDFbernard.moore610100% (20)
- Orthobiologics: J. Tracy Watson, MDDocument130 pagesOrthobiologics: J. Tracy Watson, MDDeep Katyan DeepNo ratings yet
- A Human Placenta-Derived Decellularized Connective Tissue Matrix (CTM) Supports Cellular Functions Involved in Wound Healing ProcessesDocument1 pageA Human Placenta-Derived Decellularized Connective Tissue Matrix (CTM) Supports Cellular Functions Involved in Wound Healing ProcessesbaoNo ratings yet
- Science of Hyaluronic Acid Beyond Filling - Fibroblasts and Their Response To The Extracellular MatrixDocument8 pagesScience of Hyaluronic Acid Beyond Filling - Fibroblasts and Their Response To The Extracellular MatrixAnonymous LnWIBo1GNo ratings yet
- Organisasi Tubuh ManusiaDocument34 pagesOrganisasi Tubuh ManusiaSis WantoNo ratings yet
- Porosity Measurement MethodsDocument18 pagesPorosity Measurement MethodsmahaNo ratings yet
- JCD Platelet-Rich Plasma and Hyaluronic Acid - An Efficient RADDocument8 pagesJCD Platelet-Rich Plasma and Hyaluronic Acid - An Efficient RADyellowbieNo ratings yet
- GP Dorsal Pain Case June 2021Document5 pagesGP Dorsal Pain Case June 2021Lisa NurhasanahNo ratings yet
- Journal of The Mechanical Behavior of Biomedical MaterialsDocument10 pagesJournal of The Mechanical Behavior of Biomedical MaterialsAndres Ricardo Beltran DiazNo ratings yet
- Cartilage & BoneDocument8 pagesCartilage & BoneRehab OmerNo ratings yet
- Anatomy Notes Week3Document18 pagesAnatomy Notes Week3Zainab Ali100% (1)
- Connective TissueDocument24 pagesConnective TissueIssa AvenaNo ratings yet
- Cytiva-Microcarrier Cell CultureDocument160 pagesCytiva-Microcarrier Cell CultureQuynhMai TrinhNo ratings yet
- James Oschman The Living Matrix Connective TissueDocument7 pagesJames Oschman The Living Matrix Connective TissueCarlos Braghini Jr.100% (2)
- Biomechanics of Articular CartilageDocument33 pagesBiomechanics of Articular CartilageLibbyNo ratings yet
- Tissue Renewal and Repair RegenerationDocument13 pagesTissue Renewal and Repair Regenerationمحسن حدوان عليخانNo ratings yet
- Epifix BrochureDocument2 pagesEpifix Brochureapi-235072265100% (2)
- WillemsDocument236 pagesWillemsGábor SumandánNo ratings yet
- Post-Myocardial Infarction Fibrosis. Pathophysiology, Examination, and InterventionDocument31 pagesPost-Myocardial Infarction Fibrosis. Pathophysiology, Examination, and Interventionluis sanchezNo ratings yet
- VI. Cartilage and BoneDocument14 pagesVI. Cartilage and BoneDale TelgenhoffNo ratings yet
- Wounds & Wound HealingDocument47 pagesWounds & Wound HealingDrSarmad100% (3)
- Endothelium in Health and Diseases: Dr. Meghana .P PG in PathologyDocument57 pagesEndothelium in Health and Diseases: Dr. Meghana .P PG in Pathologynnn nnnNo ratings yet
- Dental Pulp - Lecture 3Document16 pagesDental Pulp - Lecture 3Aya AlaliNo ratings yet
- Keloid TreatmentDocument19 pagesKeloid TreatmentAndrew NdewNo ratings yet
- Chapter 19 PDFDocument30 pagesChapter 19 PDFJeanPaule JoumaaNo ratings yet
- Corning Cell Culture Selection GuideDocument52 pagesCorning Cell Culture Selection GuideKimberly DelicaNo ratings yet
- Robbins 7th Ed - Chapter 3 - Tissue Renewal & Repair (2) Flashcards by Heli Sinnpson - BrainscapeDocument12 pagesRobbins 7th Ed - Chapter 3 - Tissue Renewal & Repair (2) Flashcards by Heli Sinnpson - BrainscapeCarlos MaingeNo ratings yet
- Tumori Tesuturi MoiDocument123 pagesTumori Tesuturi MoiOana BarbuNo ratings yet