You might also like
- Technical ReportDocument184 pagesTechnical Reportomen2ng88% (17)
- Emotional Reflexology: A Practical Guide - Jenny TalkingtonDocument4 pagesEmotional Reflexology: A Practical Guide - Jenny TalkingtonhegerahyNo ratings yet
- Liugong 938l Wheel Loader Parts ManualDocument20 pagesLiugong 938l Wheel Loader Parts Manualviolet100% (56)
- Pathophysiology and Management of Psoriasis Diseas1Document28 pagesPathophysiology and Management of Psoriasis Diseas1Priyanka YadavNo ratings yet
- Monthly HSE report summaryDocument5 pagesMonthly HSE report summaryNiraNo ratings yet
- Effort-Reward Imbalance and Burnout Among Nurses of Community General Hospital in San Pablo CityDocument11 pagesEffort-Reward Imbalance and Burnout Among Nurses of Community General Hospital in San Pablo CityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- TX of StriaeDocument13 pagesTX of StriaeadeNo ratings yet
- EMOTIONS AND MENTAL HEALTH - Module 8Document7 pagesEMOTIONS AND MENTAL HEALTH - Module 8Marilou HernandezNo ratings yet
- Cure Kidney Stone With Homoeopathy - by K.S. GopiDocument46 pagesCure Kidney Stone With Homoeopathy - by K.S. GopiHomeNo ratings yet
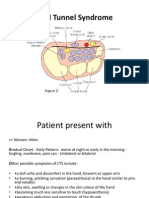
- Carpal Tunnel Syndrome Power Point PresentationDocument6 pagesCarpal Tunnel Syndrome Power Point Presentationapi-237061134No ratings yet
- Chart of Tapping PointsDocument2 pagesChart of Tapping PointsMario L M RamosNo ratings yet
- Roesch Et Al. 2018. Inflammation in Cystic Fibrosis - An UpdateDocument21 pagesRoesch Et Al. 2018. Inflammation in Cystic Fibrosis - An UpdategulararezendeNo ratings yet
- IL 17 in DiseaseDocument11 pagesIL 17 in DiseaseMaruhum NurNo ratings yet
- Skin Immune Response To S. ScabieiDocument4 pagesSkin Immune Response To S. ScabieiAhmad SyaukatNo ratings yet
- Dual Role of Th17 Cells in Crohn's Disease: Jacek Karczewski, Maciej Mazur, Marek KarczewskiDocument4 pagesDual Role of Th17 Cells in Crohn's Disease: Jacek Karczewski, Maciej Mazur, Marek KarczewskitiaraNo ratings yet
- Soluble Immunological Markers of Disease Activity in TuberculosisDocument2 pagesSoluble Immunological Markers of Disease Activity in TuberculosisMartin Lorenzo Miguel BaquilodNo ratings yet
- Immunotherapy For Sepsis - A New Approach Against An Ancient FoeDocument3 pagesImmunotherapy For Sepsis - A New Approach Against An Ancient FoeHendy SetiawanNo ratings yet
- Potential of IL-17A Antagonist as Keratinocyte Control Therapy for PsoriasisDocument21 pagesPotential of IL-17A Antagonist as Keratinocyte Control Therapy for PsoriasisXirpantNo ratings yet
- Inmunopatogenesis Del LupusDocument13 pagesInmunopatogenesis Del LupusPdfzNo ratings yet
- IL-17's Role in Asthma Pathogenesis and Potential TherapyDocument12 pagesIL-17's Role in Asthma Pathogenesis and Potential TherapyMobin Ur Rehman KhanNo ratings yet
- HHS Public Access: Discovery of The IL-23/IL-17 Signaling Pathway and The Treatment of PsoriasisDocument20 pagesHHS Public Access: Discovery of The IL-23/IL-17 Signaling Pathway and The Treatment of PsoriasisDianaNo ratings yet
- Chest: Recent Advances in Chest MedicineDocument10 pagesChest: Recent Advances in Chest MedicinegustavopsoNo ratings yet
- Cytokine: Jaymie Baliwag, Drew H. Barnes, Andrew JohnstonDocument9 pagesCytokine: Jaymie Baliwag, Drew H. Barnes, Andrew Johnstonnts1020No ratings yet
- Perspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsDocument5 pagesPerspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsIván DiazNo ratings yet
- Sepsis and The Systemic Inflammatory Response SyndromeDocument9 pagesSepsis and The Systemic Inflammatory Response SyndromeHandi Tri EffendiNo ratings yet
- IL-13 alters hypoxia genes, upregulates CD73Document7 pagesIL-13 alters hypoxia genes, upregulates CD73Syed Muaz KhalilNo ratings yet
- Atopic Dermatitis .Document7 pagesAtopic Dermatitis .nyuwwchocolavaNo ratings yet
- Jurnal DafiqDocument5 pagesJurnal DafiqDafiq Mihal F YusufNo ratings yet
- Tarea s3 Org EspDocument8 pagesTarea s3 Org EspEduardo EscobarNo ratings yet
- Review One Year in Review 2017: Systemic Lupus ErythematosusDocument11 pagesReview One Year in Review 2017: Systemic Lupus ErythematosusAmany RadwanNo ratings yet
- Autoimmunity in Atopic Dermatitis: Biomarker or Simply Epiphenomenon?Document8 pagesAutoimmunity in Atopic Dermatitis: Biomarker or Simply Epiphenomenon?Miguel RomeroNo ratings yet
- Autoinflammatory DiseasesDocument14 pagesAutoinflammatory DiseasesmedlordNo ratings yet
- Interleukin 12 and Th1 RespoDocument3 pagesInterleukin 12 and Th1 Respou77No ratings yet
- Autoimun LupusDocument10 pagesAutoimun Lupusrachmad_iriantoNo ratings yet
- Differential Expression in Lupus-Associated IL-10 Promoter Single-Nucleotide Polymorphisms Is Mediated by Poly (ADP-ribose) Polymerase-1Document13 pagesDifferential Expression in Lupus-Associated IL-10 Promoter Single-Nucleotide Polymorphisms Is Mediated by Poly (ADP-ribose) Polymerase-1samannosheenNo ratings yet
- IL-17 and TBDocument10 pagesIL-17 and TBchhatraNo ratings yet
- Tofacitinib For The Treatment of Rheumatoid Arthritis: Drug ProfileDocument13 pagesTofacitinib For The Treatment of Rheumatoid Arthritis: Drug ProfileAnggraeni PermatasariNo ratings yet
- Etiopathogenesis of PsoriasisDocument62 pagesEtiopathogenesis of PsoriasisGagan SinghNo ratings yet
- Immuno Final AbstractDocument1 pageImmuno Final AbstractLeema PriyadarshiniNo ratings yet
- Programmed Cell Death Ligand PD-L1 Contributes To The Regulation of CD4 T Effector and Regulatory T Cells in Cutaneous LeishmaniasisDocument12 pagesProgrammed Cell Death Ligand PD-L1 Contributes To The Regulation of CD4 T Effector and Regulatory T Cells in Cutaneous Leishmaniasisra bseNo ratings yet
- 2020-Autoimmunity and Organ Damage in SLEDocument24 pages2020-Autoimmunity and Organ Damage in SLECinantya Meyta SariNo ratings yet
- Atypical Cellular Disorders: Kenneth L. Mcclain, Yasodha Natkunam, and Steven H. SwerdlowDocument14 pagesAtypical Cellular Disorders: Kenneth L. Mcclain, Yasodha Natkunam, and Steven H. SwerdlowhemendreNo ratings yet
- Pathophysiology of Immune Thrombocytopenic Purpura: A Bird's-Eye ViewDocument13 pagesPathophysiology of Immune Thrombocytopenic Purpura: A Bird's-Eye ViewMa Christine TorralbaNo ratings yet
- Bullous Pemphigoid: Etiology, Pathogenesis, and Inducing Factors: Facts and ControversiesDocument9 pagesBullous Pemphigoid: Etiology, Pathogenesis, and Inducing Factors: Facts and ControversiesRiefka Ananda ZulfaNo ratings yet
- Patho Case 1Document12 pagesPatho Case 1Venz Timothy Wesley LandichoNo ratings yet
- Pulmonary, Sleep, and Critical Care Updates: Update in Tuberculosis and Nontuberculous Mycobacterial Disease 2010Document6 pagesPulmonary, Sleep, and Critical Care Updates: Update in Tuberculosis and Nontuberculous Mycobacterial Disease 2010Joseph Sipiran ReyesNo ratings yet
- Células Productoras de IL 17 e IL 17 en Protección Frente A PatologíaDocument17 pagesCélulas Productoras de IL 17 e IL 17 en Protección Frente A PatologíaJacqueline Flores MNo ratings yet
- Review Article: Systemic Lupus Erythematosus: Recent Concepts in Genomics, Pathogenetic Mechanisms, and TherapiesDocument9 pagesReview Article: Systemic Lupus Erythematosus: Recent Concepts in Genomics, Pathogenetic Mechanisms, and TherapiesDarfirizan SeprikaNo ratings yet
- PD-1 Modulating Effector Memory T Cells Response in Tuberculosis PleurisyDocument15 pagesPD-1 Modulating Effector Memory T Cells Response in Tuberculosis PleurisyHendris CitraNo ratings yet
- The Role of Inflammatory Mediators in The Pathogenesis of Nasal Polyposis: Literature ReviewDocument5 pagesThe Role of Inflammatory Mediators in The Pathogenesis of Nasal Polyposis: Literature ReviewLena Wahyu SetianingsihNo ratings yet
- Psoriasis pathophysiology current conceptsofpathogenesisDocument7 pagesPsoriasis pathophysiology current conceptsofpathogenesisAnnaNo ratings yet
- Citocinas e AsmaDocument14 pagesCitocinas e AsmaFabiula AbreuNo ratings yet
- 2009 Citokine CXCRDocument8 pages2009 Citokine CXCRDamiana MargineanuNo ratings yet
- 2b PDFDocument4 pages2b PDFAndrea Il MiodoNo ratings yet
- SITOKINDocument15 pagesSITOKINarifNo ratings yet
- JDM - Amezcua-Guerra Et Al 2017Document8 pagesJDM - Amezcua-Guerra Et Al 2017Ricardo Colín MartínezNo ratings yet
- Col I Ut 0000095 - 01Document11 pagesCol I Ut 0000095 - 01Aguirre VivianaNo ratings yet
- 1989 - Cookson Et Al. - Linkage Between Immunoglobulin E Responses Underlying Asthma and Rhinitis and Chromosome 11qDocument4 pages1989 - Cookson Et Al. - Linkage Between Immunoglobulin E Responses Underlying Asthma and Rhinitis and Chromosome 11qpond_1993No ratings yet
- Lupus FisiopatoDocument9 pagesLupus FisiopatoFernando Re TaNo ratings yet
- First French-Argentine Immunology Congress, 2010 Abstracts Held On Buenos Aires, Argentina, 2nd-5th November, 2010Document105 pagesFirst French-Argentine Immunology Congress, 2010 Abstracts Held On Buenos Aires, Argentina, 2nd-5th November, 2010International Medical PublisherNo ratings yet
- Cheng Et Al 2006 - Act - Il-17rDocument5 pagesCheng Et Al 2006 - Act - Il-17rNilabh RanjanNo ratings yet
- Jurnal BPHDocument15 pagesJurnal BPHdewasayogaNo ratings yet
- 9Document11 pages9Nejc KovačNo ratings yet
- Growth Performance of Acropora Formosa in Natural Reefs and Coral Nurseries For Reef RestorationDocument11 pagesGrowth Performance of Acropora Formosa in Natural Reefs and Coral Nurseries For Reef RestorationIsmailNo ratings yet
- Penggunaan D-Optimal Mixture Design Untuk OptimasiDocument8 pagesPenggunaan D-Optimal Mixture Design Untuk OptimasiIsmailNo ratings yet
- Todentj 14 113Document7 pagesTodentj 14 113Eti ApriyantiNo ratings yet
- 1 PBDocument8 pages1 PBIsmailNo ratings yet
- Kons PG7114-25702-1-PBDocument9 pagesKons PG7114-25702-1-PBNavisa HaifaNo ratings yet
- Melioidosis - MapDocument1 pageMelioidosis - MapIsmailNo ratings yet
- DRP LeptospirosisDocument6 pagesDRP LeptospirosisIsmailNo ratings yet
- EUCAST V - 9.0 - Breakpoint - Tables PDFDocument100 pagesEUCAST V - 9.0 - Breakpoint - Tables PDFRicardo Ariel GianeciniNo ratings yet
- Melioidosis DiagnositicsDocument9 pagesMelioidosis Diagnositicsmansoor ahmedNo ratings yet
- Art Antioxidant Potency of Water Kefir PDFDocument4 pagesArt Antioxidant Potency of Water Kefir PDFGabrielNo ratings yet
- Departamental CardioDocument9 pagesDepartamental CardioIsaac GuerreroNo ratings yet
- Pengolahan Limbah Cair Industri Farmasi Formulasi PDFDocument11 pagesPengolahan Limbah Cair Industri Farmasi Formulasi PDFHenni Pus VeraNo ratings yet
- ZQL1688 - Function Testing SOP - ADocument22 pagesZQL1688 - Function Testing SOP - AAlexandre PatrocinioNo ratings yet
- DPS Nashik Class 12 Science SyllabusDocument18 pagesDPS Nashik Class 12 Science SyllabusSayali Morwal-KumawatNo ratings yet
- Chords ListDocument5 pagesChords ListakshayNo ratings yet
- Detection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian LynxDocument5 pagesDetection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian Lynxsusey madelit apaza mamaniNo ratings yet
- Water Transport Studies in Stone Masonry With Soil Cement MortarDocument10 pagesWater Transport Studies in Stone Masonry With Soil Cement MortarTJPRC PublicationsNo ratings yet
- Chennai Public School: CH 3 Coordinate Geometry Multiple AssessmentDocument3 pagesChennai Public School: CH 3 Coordinate Geometry Multiple Assessment11F10 RUCHITA MAARANNo ratings yet
- Treatment of Acid-Related Disorders - SeminarDocument40 pagesTreatment of Acid-Related Disorders - SeminarZana Mohammed0% (1)
- Subway's Fresh Look: CEO Suzanne Greco Is Taking The Company To A Whole New Level With The Fresh Forward RebrandDocument9 pagesSubway's Fresh Look: CEO Suzanne Greco Is Taking The Company To A Whole New Level With The Fresh Forward RebrandTanvir KhanNo ratings yet
- Aashto Lane Width PDFDocument1 pageAashto Lane Width PDFnywd806033No ratings yet
- 18.national Forestry Act 1984Document92 pages18.national Forestry Act 1984Sudhir A K KumarenNo ratings yet
- SB 10054865 6305Document15 pagesSB 10054865 6305Ralph WamaeNo ratings yet
- Fault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)Document5 pagesFault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)zacarias NiquiceNo ratings yet
- A 1000 Calorie Diet Plan For Weight Loss - DMooseDocument15 pagesA 1000 Calorie Diet Plan For Weight Loss - DMoosekwasnyciakristinaNo ratings yet
- Building Schedule 050721Document6 pagesBuilding Schedule 050721Parth DaxiniNo ratings yet
- (Elsevier) The Influence of Circumferential Weld-Induced Imperfections On The Buckling of Silos ADocument12 pages(Elsevier) The Influence of Circumferential Weld-Induced Imperfections On The Buckling of Silos AMateo PaladinoNo ratings yet
- Mine Pool AtlasDocument172 pagesMine Pool AtlasRishiraj SahooNo ratings yet
- HYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTDocument3 pagesHYBRIFLEX® RRH Hybrid Cable Solution 12 X 24, 6AWG, Low-Inductance, Single-Mode Fiber, DLC Connectors Top and Bottom, 240 FTNoame Pauline SimbajonNo ratings yet
- Deltopectoral Approach to the ShoulderDocument28 pagesDeltopectoral Approach to the ShoulderChrysi TsiouriNo ratings yet
- S6000-Operation-Manual SkyliftDocument50 pagesS6000-Operation-Manual SkyliftSetiawan Tuhu basukiNo ratings yet
- ASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardDocument2 pagesASME B36.10M-2004 Welded and Seamless Wrought Steel Pipe StandardAmit BansalNo ratings yet
- Ch02 World Trade An Overview 1Document32 pagesCh02 World Trade An Overview 1XIKAMNo ratings yet
- Fluosilic Acid MsdsDocument5 pagesFluosilic Acid MsdsVuglaShemmanNo ratings yet
- Storm Water Drainage GuidelinesDocument16 pagesStorm Water Drainage GuidelinesSeeni GovindNo ratings yet
- Fine ArtsDocument12 pagesFine Artsatul prajapatiNo ratings yet
- Toyota Vehicle Glossary TermsDocument31 pagesToyota Vehicle Glossary TermsEdward Ugochukwu AdighibeNo ratings yet
- DR Vatsal Patel AhmedabadDocument30 pagesDR Vatsal Patel AhmedabadSayali PhansekarNo ratings yet
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet