You might also like
- Journal Homepage: - : Manuscript HistoryDocument13 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Fragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisDocument16 pagesFragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisTarib TrifaNo ratings yet
- Effectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisDocument8 pagesEffectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisCentral Asian StudiesNo ratings yet
- Ambiguity and Hindering Self MGTDocument8 pagesAmbiguity and Hindering Self MGTdawitNo ratings yet
- Assessment of Knowledge Level On Osteoporosis Among A Private University Students in MalaysiaDocument5 pagesAssessment of Knowledge Level On Osteoporosis Among A Private University Students in MalaysiaHizkia IndriNo ratings yet
- 2020 A Contemporary View of The Definition and Diagnosis of Osteoporosis in Children and AdolescentsDocument10 pages2020 A Contemporary View of The Definition and Diagnosis of Osteoporosis in Children and AdolescentsRaisa SugoroNo ratings yet
- Nagai 2020 Nutrition Status and Functional ProDocument7 pagesNagai 2020 Nutrition Status and Functional ProMiguel de Caso VillarroelNo ratings yet
- OsteoporosisDocument18 pagesOsteoporosisErica ValladaresNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- Assessment of Knowledge of Osteoarthritis Among Elderly PatientsDocument7 pagesAssessment of Knowledge of Osteoarthritis Among Elderly PatientsMostafa ShabanNo ratings yet
- A Descriptive Study To Assess The Level of Knowledge On Preventive Measures of Osteoarthritis Among Old Age People at Urban AreaDocument4 pagesA Descriptive Study To Assess The Level of Knowledge On Preventive Measures of Osteoarthritis Among Old Age People at Urban AreaEditor IJTSRDNo ratings yet
- Assessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportDocument14 pagesAssessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportKhủngLongSiêuNguyHiểmNo ratings yet
- Remote Management of OsteoporosisDocument9 pagesRemote Management of OsteoporosispremamoyNo ratings yet
- F. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. MazzagliaDocument6 pagesF. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. Mazzagliafirdha afghaniNo ratings yet
- Prevalence of Knee Osteoarthritis, Its.61Document7 pagesPrevalence of Knee Osteoarthritis, Its.61Hadley AuliaNo ratings yet
- Prevalence and Consequence of Customized Ocular Prosthesis in Last 15 Years at Dhaka City, Bangladesh: A Retrospective StudyDocument6 pagesPrevalence and Consequence of Customized Ocular Prosthesis in Last 15 Years at Dhaka City, Bangladesh: A Retrospective Studymohammaddu49No ratings yet
- E-1-Osteoporosis and Periodontitis 2016Document14 pagesE-1-Osteoporosis and Periodontitis 2016Yessid Baltazar Arango100% (1)
- OsteoporosisDocument6 pagesOsteoporosisGheavita Chandra DewiNo ratings yet
- Osteoporosis Prevention, Diagnosis, and Therapy: Consensus ConferenceDocument11 pagesOsteoporosis Prevention, Diagnosis, and Therapy: Consensus ConferenceCorin Boice TelloNo ratings yet
- 12 PDFDocument9 pages12 PDFSuresh BabuNo ratings yet
- Prediction of Hip and Hand Fractures in Older Persons With or Without A Diagnosis of PeriodontitisDocument5 pagesPrediction of Hip and Hand Fractures in Older Persons With or Without A Diagnosis of PeriodontitismarishaNo ratings yet
- Orthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderDocument8 pagesOrthopaedic Surgery - 2019 - Qu - Bone Turnover Markers and Bone Mineral Density To Predict Osteoporotic Fractures in OlderAlfred AlfredNo ratings yet
- Neck Pain: Global Epidemiology, Trends and Risk Factors: Review Open AccessDocument13 pagesNeck Pain: Global Epidemiology, Trends and Risk Factors: Review Open Accessalya adhanaNo ratings yet
- Vertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenDocument11 pagesVertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenAdhiatma DotNo ratings yet
- A Hierarchical Opportunistic Screening Model For Osteoporosis Using Machine Learning Applied To Clinical Data and CT ImagesDocument15 pagesA Hierarchical Opportunistic Screening Model For Osteoporosis Using Machine Learning Applied To Clinical Data and CT Imagesviju001No ratings yet
- King ShannonDocument9 pagesKing Shannonarifin hidayatNo ratings yet
- 2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadDocument6 pages2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadRodrigoMarinNo ratings yet
- Osteoporosis Research Paper PDFDocument6 pagesOsteoporosis Research Paper PDFhbzqwpulg100% (3)
- DR Tarek Amin Professor of Public Health Cairo UniversityDocument39 pagesDR Tarek Amin Professor of Public Health Cairo UniversityasdfNo ratings yet
- Bone Reports: A A B C C B CDocument9 pagesBone Reports: A A B C C B Caeroforce20No ratings yet
- Fall in AdultDocument14 pagesFall in AdultSandi IrvantaNo ratings yet
- Relationship Between Osteoporosis and Periodontal Disease: Review of The LiteratureDocument9 pagesRelationship Between Osteoporosis and Periodontal Disease: Review of The Literatureaakanksha bhardwajNo ratings yet
- Surgical Oncology: SciencedirectDocument8 pagesSurgical Oncology: SciencedirectMIGUEL MORENONo ratings yet
- UK Clinical Guideline For The Prevention and Treatment of OsteoporosisDocument46 pagesUK Clinical Guideline For The Prevention and Treatment of OsteoporosisHninNo ratings yet
- Archives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisDocument13 pagesArchives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisBHUENDOCRINE SRNo ratings yet
- Association of Developmental Coordination Disorder and 2022 Research in DeveDocument19 pagesAssociation of Developmental Coordination Disorder and 2022 Research in DeveGeorgiana BunghiuzNo ratings yet
- Fractura de CaderaDocument9 pagesFractura de CaderaWendy Lorely Téllez HernándezNo ratings yet
- Jurnal MuskuloDocument8 pagesJurnal MuskuloarvinelaNo ratings yet
- Prevalence and Associated Risk Factors of Osteoporosis Among Elderly Patients in Al-Ahsa Region, Saudi Arabia: A Cross-Sectional StudyDocument8 pagesPrevalence and Associated Risk Factors of Osteoporosis Among Elderly Patients in Al-Ahsa Region, Saudi Arabia: A Cross-Sectional StudyIJAR JOURNALNo ratings yet
- Screening For Osteoporosis - UpToDateDocument22 pagesScreening For Osteoporosis - UpToDatesindy suarezNo ratings yet
- Public Health Nut8Document17 pagesPublic Health Nut8Fiki FerindraNo ratings yet
- CGJ 18 29 PDFDocument6 pagesCGJ 18 29 PDFZenithaMeidaNo ratings yet
- Jurnal Muskuloskeletal: Related PapersDocument16 pagesJurnal Muskuloskeletal: Related PapersYashi AkbarNo ratings yet
- DOH Guideline For The Screening of OsteoporosisDocument11 pagesDOH Guideline For The Screening of OsteoporosisBasil al-hashaikehNo ratings yet
- 1471 2474 14 271 1Document8 pages1471 2474 14 271 1Bernamai CalamNo ratings yet
- Geriatria y OrtopediaDocument28 pagesGeriatria y OrtopediaHector VallejosNo ratings yet
- Perceptions of Stigma Associated With Chronic Knee Pain Voices of Selected Women in Thailand and MalaysiaDocument17 pagesPerceptions of Stigma Associated With Chronic Knee Pain Voices of Selected Women in Thailand and Malaysiakmoujahid185No ratings yet
- An Update On Osteoporosis Research: Effect of Calcium Plus Vitamin D SupplementationDocument9 pagesAn Update On Osteoporosis Research: Effect of Calcium Plus Vitamin D SupplementationTowhid HasanNo ratings yet
- 2022 Article 2985Document8 pages2022 Article 2985Ioana Andreea SinNo ratings yet
- Ijerph 19 02999 With CoverDocument10 pagesIjerph 19 02999 With CoverJADIT YASIRA MENDOZA HERNANDEZNo ratings yet
- Prevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyDocument9 pagesPrevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyTanvirNo ratings yet
- Management of Severe OsteoporosisDocument16 pagesManagement of Severe OsteoporosisZendy Nicole Cano SaavedraNo ratings yet
- 11 Dai 2023Document12 pages11 Dai 2023SRINIVASAN NARASIMHANNo ratings yet
- 1 s2.0 S1013905222001420 MainDocument7 pages1 s2.0 S1013905222001420 MainSuper LonelyNo ratings yet
- v07p0681 PDFDocument6 pagesv07p0681 PDFAzizaNo ratings yet
- New National Osteoporosis Guidance - Implications For GeriatriciansDocument6 pagesNew National Osteoporosis Guidance - Implications For GeriatriciansJENNY LILIANA ALARCON FERNANDEZNo ratings yet
- The Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsDocument13 pagesThe Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsJevon JavierNo ratings yet
- A Perspective On Osteoarthritis Research in Singapore: ReviewDocument9 pagesA Perspective On Osteoarthritis Research in Singapore: ReviewRhinaNo ratings yet
- A Study of The Relationship Between Osteoporosis With Demographic Characteristics and Some Other Factors by Using Bone DensitometryDocument13 pagesA Study of The Relationship Between Osteoporosis With Demographic Characteristics and Some Other Factors by Using Bone Densitometrysnakemamba00No ratings yet
- The Osteoporotic Syndrome: Detection, Prevention, and TreatmentFrom EverandThe Osteoporotic Syndrome: Detection, Prevention, and TreatmentNo ratings yet
- Panduan Penatalaksanaan Hemofilia PDFDocument55 pagesPanduan Penatalaksanaan Hemofilia PDFrahman090789100% (2)
- PICK1 Deficiency Exacerbates Sepsis-Associated AcuDocument12 pagesPICK1 Deficiency Exacerbates Sepsis-Associated AcuDeddy ZulkarnaenNo ratings yet
- Pathophysiology and Treatment of Osteoporosis: Challenges For Clinical Practice in Older PeopleDocument15 pagesPathophysiology and Treatment of Osteoporosis: Challenges For Clinical Practice in Older PeopleDeddy ZulkarnaenNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleDeddy ZulkarnaenNo ratings yet
- PICK1 Deficiency Exacerbates Sepsis-Associated AcuDocument12 pagesPICK1 Deficiency Exacerbates Sepsis-Associated AcuDeddy ZulkarnaenNo ratings yet
- Thousand Suns Starships - Chapter 3 Cheat SheetDocument16 pagesThousand Suns Starships - Chapter 3 Cheat SheetRogue GamesNo ratings yet
- Skills Development PlanDocument1 pageSkills Development PlanJES MARIES MENDEZNo ratings yet
- Generative NLP Robert Dilts PDFDocument11 pagesGenerative NLP Robert Dilts PDFCristina LorinczNo ratings yet
- CTS Company Profile Rev0Document11 pagesCTS Company Profile Rev0khalesnabilNo ratings yet
- Saidin PSC - SHO UTMSPACE - 13.01.22 Module Slide 6s - LDocument43 pagesSaidin PSC - SHO UTMSPACE - 13.01.22 Module Slide 6s - LAmer IkhwanNo ratings yet
- New Section: Jeff Is Quite Tall. Karl Is The Same Height As JeffDocument6 pagesNew Section: Jeff Is Quite Tall. Karl Is The Same Height As JeffIbrahim MahmoudNo ratings yet
- BYRGMv 3Document30 pagesBYRGMv 3tajsisNo ratings yet
- (IMP) Ancient Indian JurisprudenceDocument28 pages(IMP) Ancient Indian JurisprudenceSuraj AgarwalNo ratings yet
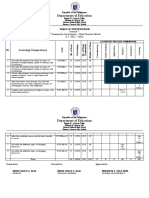
- Department of Education: Learning CompetencyDocument2 pagesDepartment of Education: Learning CompetencyShaira May Tangonan CaragNo ratings yet
- Prac Res Q2 Module 8Document12 pagesPrac Res Q2 Module 8Benicel Lane De VeraNo ratings yet
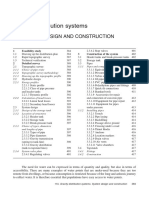
- Gravity Distribution Systems: A System Design and ConstructionDocument40 pagesGravity Distribution Systems: A System Design and ConstructionTooma DavidNo ratings yet
- CRE Chapter 5 (Solutions)Document8 pagesCRE Chapter 5 (Solutions)Bella HannaNo ratings yet
- NDX DolsonDocument67 pagesNDX DolsonMahanta BorahNo ratings yet
- Original PDF Biological Psychology 1st Edition by Kelly G Lambert PDFDocument41 pagesOriginal PDF Biological Psychology 1st Edition by Kelly G Lambert PDFclarence.barcia711100% (35)
- IHS Markit Seed Market Analysis and Data InfographicDocument1 pageIHS Markit Seed Market Analysis and Data Infographictripurari pandeyNo ratings yet
- Afa 7&8Document11 pagesAfa 7&8APMNo ratings yet
- PCS-9613S X DataSheet en Overseas General X R1.10Document57 pagesPCS-9613S X DataSheet en Overseas General X R1.10parveen115No ratings yet
- DIRECTION: Read Each Question Carefully. Encircle The Letter That Corresponds To The Letter of Your AnswerDocument2 pagesDIRECTION: Read Each Question Carefully. Encircle The Letter That Corresponds To The Letter of Your AnswerMea-Ann OscianasNo ratings yet
- Reducing Streetism: A Neglected Cause of Social Anxiety and Delinquency in Adama CityDocument25 pagesReducing Streetism: A Neglected Cause of Social Anxiety and Delinquency in Adama CityKorie ArsieNo ratings yet
- Đề Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Document8 pagesĐề Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Chi Vũ LinhNo ratings yet
- Mai 4.9 Discrete DistributionsDocument16 pagesMai 4.9 Discrete DistributionsAvatNo ratings yet
- I Learned Chapter 8-The Power of GuidanceDocument1 pageI Learned Chapter 8-The Power of Guidanceapi-295870335No ratings yet
- Intro To Bifurcation TheoryDocument47 pagesIntro To Bifurcation TheoryJohn StarrettNo ratings yet
- P, PI and PID ControlDocument3 pagesP, PI and PID ControlsivaNo ratings yet
- Mendelian & Modern Genetics: General Biology 2Document51 pagesMendelian & Modern Genetics: General Biology 2sannsannNo ratings yet
- SP Q4 Week 2 HandoutDocument10 pagesSP Q4 Week 2 HandoutLenard BelanoNo ratings yet
- Spouse Visa AttorneyDocument2 pagesSpouse Visa AttorneyShaheen SadiqueNo ratings yet
- OG19 RC 新题解析Document14 pagesOG19 RC 新题解析Chi JianNo ratings yet
- 302 Decision Science Question - PaperDocument3 pages302 Decision Science Question - Paperajay taleNo ratings yet
- Breathwork Fundamentals GuidebookDocument148 pagesBreathwork Fundamentals GuidebookJuliana RennerNo ratings yet