You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Magnetism 02Document10 pagesMagnetism 02Niharika DeNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 0 - 07 - B - 0056 - Diagnostics Made Easy-03042014-NG-webDocument64 pages0 - 07 - B - 0056 - Diagnostics Made Easy-03042014-NG-webtongaiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ssgstartersguide OneDocument18 pagesSsgstartersguide OneLuis RibeiroNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 0625 Nos SK 5 PDFDocument3 pages0625 Nos SK 5 PDFyuke kristinaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Electromagnet 8.1Document14 pagesElectromagnet 8.1Christopher AuNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Biomagnetic Bracelet Biolife IndiaDocument61 pagesBiomagnetic Bracelet Biolife Indiasagarkumar11No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Simulation of Induction HeatingDocument64 pagesSimulation of Induction HeatingaungkyawmyoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
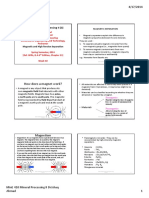
- How Does A Magnet Work?: Mine 410 Mineral Processing IiDocument12 pagesHow Does A Magnet Work?: Mine 410 Mineral Processing Iiabd ullahNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Curie Temp KanthalDocument3 pagesCurie Temp KanthalMoamen MohamedNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Lab EM2 (Answers)Document2 pagesLab EM2 (Answers)Mohamed Zolthan Sacko57% (7)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Class Test - Physics - Magnetism and MatterDocument3 pagesClass Test - Physics - Magnetism and MattermrudulmittalNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Q'uo Transcripts 2009 - LL ResearchDocument327 pagesThe Q'uo Transcripts 2009 - LL ResearchSúperManny100% (1)
- Chapter No. 01: Magnetic CircuitsDocument53 pagesChapter No. 01: Magnetic CircuitsUmar SheikhNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Spooky2 Optimising Remote TreatmentsDocument6 pagesSpooky2 Optimising Remote TreatmentstestnationNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Historical Evolution of Motor TechnologyDocument8 pagesHistorical Evolution of Motor TechnologyddadaraNo ratings yet
- 6.2 MixtureDocument11 pages6.2 MixtureLEE JIA XUAN MoeNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- ICSE+10+Electromagnetism+-+Part+1+ +One+Shot +AKRDocument75 pagesICSE+10+Electromagnetism+-+Part+1+ +One+Shot +AKRCOW GUPTA100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Performance of A Low-Density Hypersonic Magneto-Aerodynamic FacilityDocument21 pagesPerformance of A Low-Density Hypersonic Magneto-Aerodynamic FacilityReshad NawoorNo ratings yet
- E401Document5 pagesE401Mai XiaoNo ratings yet
- Magnets and Magnetic FieldsDocument4 pagesMagnets and Magnetic FieldsCameronNo ratings yet
- Models and Strategies For Teaching: HMEF5123Document32 pagesModels and Strategies For Teaching: HMEF5123Norihan Kamal100% (1)
- Grade 12 Physics Investigatory ProjectDocument3 pagesGrade 12 Physics Investigatory ProjectAziyaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Boy and A MotorDocument69 pagesA Boy and A MotorJShearer100% (3)
- AS5000-MS-20-150 Spec v0 1Document7 pagesAS5000-MS-20-150 Spec v0 1Victor ConstantinNo ratings yet
- Break It Apart Technical ReportDocument9 pagesBreak It Apart Technical Reportapi-347850579No ratings yet
- Chapter 5Document13 pagesChapter 5aregawi weleabezgiNo ratings yet
- CT SaturationDocument21 pagesCT Saturationteha73No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Atomic Energy Education Society Multiple Choice Questions Test ACADEMIC YEAR 2018-19Document15 pagesAtomic Energy Education Society Multiple Choice Questions Test ACADEMIC YEAR 2018-19Vishal JalanNo ratings yet
- Full MFLDocument25 pagesFull MFLNikhil MohanNo ratings yet
- 2 The Laws of Universe and Life PROTEGIDODocument72 pages2 The Laws of Universe and Life PROTEGIDOMedesan FlorinNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)