You might also like
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- Nursing Responsibilities in The Care of Casts Traction FixatorsDocument20 pagesNursing Responsibilities in The Care of Casts Traction FixatorsBasmah A. AdompingNo ratings yet
- EMERGENCY CARE FOR BEGINNERS: Essential First Aid Techniques and Tips (2024)From EverandEMERGENCY CARE FOR BEGINNERS: Essential First Aid Techniques and Tips (2024)No ratings yet
- CT CastCareDocument2 pagesCT CastCareLaira CañeteNo ratings yet
- After Mastectomy: Healing Physically and EmotionallyFrom EverandAfter Mastectomy: Healing Physically and EmotionallyRating: 3 out of 5 stars3/5 (1)
- Nursing Care PlansDocument3 pagesNursing Care PlansBeyotchsangreMesswithurownlifeNo ratings yet
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.From EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.No ratings yet
- Procedure-Lumber PunctureDocument11 pagesProcedure-Lumber Puncturemohamad dildarNo ratings yet
- First Aid & Emergency Companions: First Aid & Emergencies at SeaFrom EverandFirst Aid & Emergency Companions: First Aid & Emergencies at SeaNo ratings yet
- HESI ReviewerDocument10 pagesHESI ReviewerAnonymous XhAUv9lp8100% (2)
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointFrom EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointNo ratings yet
- Nursing Review Bullet For Funda (-Credits To OWNER-)Document4 pagesNursing Review Bullet For Funda (-Credits To OWNER-)Camille Honeyleith Lanuza FernandoNo ratings yet
- Reflexology: 22 Amazing Techniques to Successfully Relax Your Hands & FeetFrom EverandReflexology: 22 Amazing Techniques to Successfully Relax Your Hands & FeetRating: 4 out of 5 stars4/5 (1)
- Applying A CastDocument13 pagesApplying A CastHampson MalekanoNo ratings yet
- Preop & Postop Nursing InterventionsDocument8 pagesPreop & Postop Nursing InterventionsLizethNo ratings yet
- Wa0000.Document34 pagesWa0000.Abdelrahman AbdouNo ratings yet
- Lumbar Puncture (Lumbar Tap)Document21 pagesLumbar Puncture (Lumbar Tap)Paul Gabriel CasquejoNo ratings yet
- RestraintsDocument16 pagesRestraintsSowjanyaNo ratings yet
- Nursing Outcome, Nursing Interventions, and Patient Teaching For Inguinal HerniaDocument4 pagesNursing Outcome, Nursing Interventions, and Patient Teaching For Inguinal HerniaPrincesz Zharah CansicioNo ratings yet
- Bullets FundamentalsDocument45 pagesBullets Fundamentalsj UNo ratings yet
- Nursing Care Plan For Angina Pectoris NCPDocument2 pagesNursing Care Plan For Angina Pectoris NCPderic73% (15)
- Log Rolling A PatientDocument27 pagesLog Rolling A PatientIrish Jane Gallo100% (1)
- Maternal and ChildDocument4 pagesMaternal and ChildNestor CajesNo ratings yet
- Prepared By: Jayvie B. Gacutan, RN Nat'l 10 Placer July 2011 NLEDocument30 pagesPrepared By: Jayvie B. Gacutan, RN Nat'l 10 Placer July 2011 NLEOmie TumanguilNo ratings yet
- Intra Muscular Injection in ChildrenDocument9 pagesIntra Muscular Injection in ChildrenssNo ratings yet
- Nursing Care Plan For Inguinal HerniaDocument5 pagesNursing Care Plan For Inguinal HerniaIv'z Tandoc67% (6)
- Fundamentals of Nursing BulletsDocument14 pagesFundamentals of Nursing BulletsFRIA DEMAISIPNo ratings yet
- Translate Bantal PemanasDocument4 pagesTranslate Bantal Pemanasdrmawan_gama_tektoNo ratings yet
- Fundamental of NursingDocument6 pagesFundamental of NursingHenesis NioganNo ratings yet
- Traction Application Nursing ManagementDocument17 pagesTraction Application Nursing ManagementLatrell GelacioNo ratings yet
- Bantal Untuk PemanasanDocument4 pagesBantal Untuk Pemanasandrmawan_gama_tektoNo ratings yet
- Fundamentals of Nursing BULLETSDocument7 pagesFundamentals of Nursing BULLETSNiña Marie Lim QuitanNo ratings yet
- TXTDocument356 pagesTXTJec AmracNo ratings yet
- Limb AmputationDocument4 pagesLimb Amputationxllxxcxm -No ratings yet
- External Fixation: Nursing Best Practice GuidelinesDocument25 pagesExternal Fixation: Nursing Best Practice GuidelinesDoneva Lyn MedinaNo ratings yet
- AB Critical Thinking ExercisesDocument4 pagesAB Critical Thinking ExercisesAhmad BaolayyanNo ratings yet
- Musculoskeletal Care ModalitiesDocument53 pagesMusculoskeletal Care ModalitiesJona Kristin EnclunaNo ratings yet
- Level of Student - B.SC (N) Ii Yrs Traction: Presented byDocument7 pagesLevel of Student - B.SC (N) Ii Yrs Traction: Presented bydhanasundariNo ratings yet
- BMS ChecklistsDocument16 pagesBMS ChecklistsMahmoud AbouelsoudNo ratings yet
- Care of Patients With Traction TractionDocument5 pagesCare of Patients With Traction TractionMOHAMMAD JABBER M. PAUDACJRNo ratings yet
- Assessing Patients and Managing Acute SituationDocument27 pagesAssessing Patients and Managing Acute SituationCHONANo ratings yet
- AmputationDocument26 pagesAmputationmaglangitjoannamarie1920No ratings yet
- NAME: - SKILLS NO: - BSN: - DateDocument5 pagesNAME: - SKILLS NO: - BSN: - DateJenny AjocNo ratings yet
- Neuroo 170210095341 PDFDocument162 pagesNeuroo 170210095341 PDFmalathiNo ratings yet
- Course Task - Cast CareDocument3 pagesCourse Task - Cast CareJhaji Mei Margarete CasiNo ratings yet
- ODocument37 pagesOyaraNo ratings yet
- NursingprocedureDocument8 pagesNursingprocedureJANELLE GIFT SENARLONo ratings yet
- 2011 Medical Surgical Hesi RemediationDocument69 pages2011 Medical Surgical Hesi RemediationTheMench67% (3)
- Nursing Bullets Ni AcepotDocument48 pagesNursing Bullets Ni AcepotAce MereriaNo ratings yet
- Fundamentals of Nursing Bullets (Nle & Nclex)Document32 pagesFundamentals of Nursing Bullets (Nle & Nclex)ulcNo ratings yet
- Random Nle FactsDocument31 pagesRandom Nle FactsChristianAnthonyRaagasNo ratings yet
- Fundamentals of NursingDocument12 pagesFundamentals of Nursingneleh grayNo ratings yet
- Fundamentals of Nursing BulletsDocument32 pagesFundamentals of Nursing BulletsCatherine G. BorrasNo ratings yet
- Different of Position For Medical ExaminationDocument19 pagesDifferent of Position For Medical ExaminationQueeny Anne Apil100% (1)
- Arellano University - Funda Reviewer - 1Document11 pagesArellano University - Funda Reviewer - 1tinea nigraNo ratings yet
- Rle 1Document7 pagesRle 1kvvalencia2128valNo ratings yet
- Arellano University - Funda Reviewer - 1Document11 pagesArellano University - Funda Reviewer - 1jcarysuitosNo ratings yet
- Week 5 Prelab Homework - AnswersDocument6 pagesWeek 5 Prelab Homework - AnswerswilliamsdevanelNo ratings yet
- CNA Body Mechanics Bed Making Comfort CareDocument32 pagesCNA Body Mechanics Bed Making Comfort CareFaith VaughnNo ratings yet
- Nursing Bullets 1Document81 pagesNursing Bullets 1Tsuyoshi BangNo ratings yet
- CKD Presentation GroupDocument49 pagesCKD Presentation GroupAhmad BaolayyanNo ratings yet
- E Learning SamifinalDocument22 pagesE Learning SamifinalAhmad BaolayyanNo ratings yet
- E-Learning Midterm BSN-IV 1Document18 pagesE-Learning Midterm BSN-IV 1Ahmad BaolayyanNo ratings yet
- University of Luzon College of Business Administration Perez Blvd. Dagupan City, PangasinanDocument9 pagesUniversity of Luzon College of Business Administration Perez Blvd. Dagupan City, PangasinanAhmad BaolayyanNo ratings yet
- Learning Activities: Click To Edit Master Title StyleDocument12 pagesLearning Activities: Click To Edit Master Title StyleAhmad BaolayyanNo ratings yet
- Group3 Title Final WorkDocument114 pagesGroup3 Title Final WorkAhmad BaolayyanNo ratings yet
- NCLEX Critical Thinking Student Workbook 2021Document20 pagesNCLEX Critical Thinking Student Workbook 2021Ahmad BaolayyanNo ratings yet
- Ahmed CASE SCENARIO ExamDocument7 pagesAhmed CASE SCENARIO ExamAhmad BaolayyanNo ratings yet
- Dec14 (Reflection PaperDocument2 pagesDec14 (Reflection PaperAhmad BaolayyanNo ratings yet
- Ahmed Ba Elaian Bsn-Iv: 1. What Emergent Management Should The Nurse Anticipate For The Patient?Document2 pagesAhmed Ba Elaian Bsn-Iv: 1. What Emergent Management Should The Nurse Anticipate For The Patient?Ahmad BaolayyanNo ratings yet
- Confirmation of Cover: Benefits Limits (Plan E)Document2 pagesConfirmation of Cover: Benefits Limits (Plan E)Ahmad BaolayyanNo ratings yet
- 1960 1970sDocument3 pages1960 1970sAhmad BaolayyanNo ratings yet
- Of The Compensatory, Progressive, and Irreversible Stages of ShockDocument4 pagesOf The Compensatory, Progressive, and Irreversible Stages of ShockAhmad BaolayyanNo ratings yet
- Ahmed IntercultureDocument2 pagesAhmed IntercultureAhmad BaolayyanNo ratings yet
- Sample Academic Reading Matching HeadingsDocument3 pagesSample Academic Reading Matching HeadingsNaila sifaNo ratings yet
- Ahmed IntercultureDocument2 pagesAhmed IntercultureAhmad BaolayyanNo ratings yet
- Generic Name Indication (S) Action Adverse Reaction (S) Interaction (S) Contraindication (S) Patient Teaching (S) Nursing Implication (S)Document1 pageGeneric Name Indication (S) Action Adverse Reaction (S) Interaction (S) Contraindication (S) Patient Teaching (S) Nursing Implication (S)Ahmad BaolayyanNo ratings yet
- Respiratory System NewDocument74 pagesRespiratory System NewAhmad BaolayyanNo ratings yet
- Health Statistics and EpidemiologyDocument44 pagesHealth Statistics and EpidemiologyAhmad BaolayyanNo ratings yet
- 1993s (The Cochrane Collaboration Is Established. Magnet Recognition Program Makes First Awards)Document3 pages1993s (The Cochrane Collaboration Is Established. Magnet Recognition Program Makes First Awards)Ahmad BaolayyanNo ratings yet
- Format For Process RecordingDocument3 pagesFormat For Process RecordingAhmad BaolayyanNo ratings yet
- Generic Name Indication (S) Action Adverse Reaction (S) Interaction (S) Contraindication (S) Patient Teaching (S) Nursing Implication (S)Document1 pageGeneric Name Indication (S) Action Adverse Reaction (S) Interaction (S) Contraindication (S) Patient Teaching (S) Nursing Implication (S)Ahmad BaolayyanNo ratings yet
- Respiratory System NewDocument74 pagesRespiratory System NewAhmad BaolayyanNo ratings yet
- Case Study, Chapter 41, Management of Patients With Musculoskeletal DisordersDocument3 pagesCase Study, Chapter 41, Management of Patients With Musculoskeletal DisordersAhmad BaolayyanNo ratings yet
- Common Surgical Instruments ModuleDocument5 pagesCommon Surgical Instruments ModuleAlokKumarNo ratings yet
- Case Study, Chapter 42, Management of Patients With Musculoskeletal TraumaDocument2 pagesCase Study, Chapter 42, Management of Patients With Musculoskeletal TraumaAhmad BaolayyanNo ratings yet
- Health Statistics and EpidemiologyDocument44 pagesHealth Statistics and EpidemiologyAhmad BaolayyanNo ratings yet
- Viral Hepatitis: Ms. Whelhelmina Montefrio, BSN, R.NDocument49 pagesViral Hepatitis: Ms. Whelhelmina Montefrio, BSN, R.NAhmad BaolayyanNo ratings yet
- University of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsDocument10 pagesUniversity of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsAhmad BaolayyanNo ratings yet
- Psychotherapy DAP NoteDocument2 pagesPsychotherapy DAP NoteMistor Williams100% (1)
- Drug Study Atropine SulfateDocument1 pageDrug Study Atropine Sulfateirhizzp75% (8)
- CHN Prelim QuizDocument5 pagesCHN Prelim QuizVanessa Mae Rara100% (1)
- Pediatrics RemarksDocument62 pagesPediatrics RemarksGÖKSU SAYGILINo ratings yet
- Normal ObDocument31 pagesNormal ObShai EstrellerNo ratings yet
- Immune Responses, and TransplantationDocument7 pagesImmune Responses, and TransplantationJoyzoeyNo ratings yet
- PTS - Soal Bahasa Inggris Kelas IXDocument6 pagesPTS - Soal Bahasa Inggris Kelas IXRini YusmayantiNo ratings yet
- Biostat 2020 62 QDocument270 pagesBiostat 2020 62 Q'محمد علي' محمد لافيNo ratings yet
- ICU AlgorithmsDocument45 pagesICU AlgorithmsHashimIdreesNo ratings yet
- Redefining Wellness: Ultimate Mold GuideDocument11 pagesRedefining Wellness: Ultimate Mold Guidereyshme0% (1)
- Hypertensive Disorders of Pregnancy 33Document36 pagesHypertensive Disorders of Pregnancy 33Asteway MesfinNo ratings yet
- Annex D Health Declaretion FormDocument2 pagesAnnex D Health Declaretion FormMa. Leonora TumamposNo ratings yet
- Epidemiology (Approaches &methods), Disease Causation and ScreeningDocument37 pagesEpidemiology (Approaches &methods), Disease Causation and ScreeningSyed Arifa AndrabiNo ratings yet
- Module 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewDocument10 pagesModule 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewEmily BernatNo ratings yet
- Comorbid Psychopathology in AuDocument12 pagesComorbid Psychopathology in Auiuliabucur92No ratings yet
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 pagesGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000No ratings yet
- Food HygieneDocument31 pagesFood Hygienehemihema100% (1)
- What Are Bacteria - Streptococcus FaecalisDocument3 pagesWhat Are Bacteria - Streptococcus FaecalisAnkan PalNo ratings yet
- Neoplasms - Primary and Secondary Neoplasms of The BrainDocument11 pagesNeoplasms - Primary and Secondary Neoplasms of The BrainHisabu MohammedNo ratings yet
- CME AnaemiaDocument40 pagesCME AnaemiaNini Shuhaida Mat HarunNo ratings yet
- Atelektasis Jurnal RadiologiDocument19 pagesAtelektasis Jurnal RadiologiRachmi MerrinaNo ratings yet
- Sensory Practice TestDocument19 pagesSensory Practice TestJennelyn GinturoNo ratings yet
- What Is Brain CancerDocument3 pagesWhat Is Brain Canceryash vardhanNo ratings yet
- Controversies Practice Changers in Ob-GynDocument57 pagesControversies Practice Changers in Ob-GynVirginia AbalosNo ratings yet
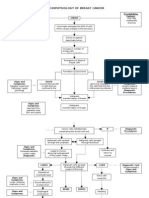
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- PolydactylyDocument16 pagesPolydactylyGupies100% (1)
- TB PosterDocument13 pagesTB Posterthamizhselvi87No ratings yet
- Vesicular and Bullous Dermatosis MCQsDocument59 pagesVesicular and Bullous Dermatosis MCQsDr.Tawheed88% (8)
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.ANo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)