Professional Documents
Culture Documents
Netik
Uploaded by
Adil BarutOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Netik
Uploaded by
Adil BarutCopyright:
Available Formats
International Journal of Urology (2020) doi: 10.1111/iju.
14230
Review Article
Peyronie’s disease: Contemporary evaluation and management
Matthew J Ziegelmann,1,2 Petar Bajic1 and Laurence A Levine1
1
Division of Urology, Rush University Medical Center, Chicago, Illinois, and 2Department of Urology, Mayo Clinic, Rochester,
Minnesota, USA
Abbreviations & Acronyms Abstract: Peyronie’s disease is a common yet poorly understood condition
AMS = American Medical characterized by penile pain, curvature, sexual dysfunction and psychological bother.
Systems Peyronie’s disease represents a penile wound healing disorder, and is thought to arise
AUA = American Urological from exuberant scarring in response to penile trauma in genetically predisposed men. In
Association the absence of active treatment, the majority of men experience stable or worsening
CCH = collagenase symptoms, with few reporting spontaneous resolution in penile curvature or other
Clostridium histolyticum deformity. In contrast, penile pain improves or resolves in the majority of men.
CUA = Canadian Urological Treatment options vary based on symptom severity and stability. Several oral therapies
Association are commonly prescribed, although to date there are no strong data to support any oral
ED = erectile dysfunction agents as monotherapy for Peyronie’s disease. Other options including penile traction
EMDA = electromotive drug therapy and intralesional injections result in modest improvements for many patients,
administration particularly when used early after symptom onset. Penile straightening through
ICI = intracavernosal approaches, such as penile plication and plaque incision or partial excision and grafting,
injection represent the most rapid and reliable approach to correct penile curvature once the
IFN = interferon symptoms have stabilized. Side-effects vary based on the type of surgery carried out,
ILI = intralesional injection and include penile shortening, sensation changes and erectile dysfunction in the minority
IPP = inflatable penile of men. In patients with drug refractory erectile dysfunction and Peyronie’s disease,
prosthesis placement of a penile prosthesis will address both issues, and is associated with high
PD = Peyronie’s disease levels of patient satisfaction. The current review provides a practical approach to the
PDE5I = modern evaluation and management of patients presenting with Peyronie’s disease.
phosphodiesterase 5
inhibitor
Key words: collagenase, grafting, penile curvature, plication, Xiaflex.
PDQ = Peyronie’s Disease
Questionnaire
PTT = penile traction Introduction
therapy PD is a wound-healing disorder characterized by penile pain, curvature and sexual dysfunc-
SPL = stretched penile tion. Francois Gigot de la Peyronie first described treatment for “induratio penis plastica” in
length 1743.1,2 However, the condition today known as PD was described as early as the 13th cen-
SWT = shockwave therapy tury.3,4 PD represents abnormal healing in response to trauma within the penile tunica albug-
TAP = tunica albuginea inea.5,6 Despite this, just 20–30% of patients recall preceding trauma, such as mis-thrust
plication during intercourse.6,7 Peyronie’s “plaque” (scar) results from abnormal extracellular matrix
VT = vacuum therapy production through upregulation of myofibroblast activity and tissue inhibitors of matrix met-
alloproteinases, among other mechanisms.8,9 There is a link between personal or family his-
Correspondence: Laurence A tory of PD and Dupuytren’s contractures, suggesting a genetic predisposition.10,11
Levine M.D., Division of PD is broadly differentiated into an acute (“active”) inflammatory phase and a chronic
Urology, Rush University (“stable”) phase. The former is characterized by variable penile pain and progressive penile
Medical Center, 1725 West deformity. The latter is characterized by symptom stability and pain improvement/resolution.
Harrison Street, Suite #352, To date, there are no firmly agreed upon criteria characterizing the transition to chronic PD.
Chicago, IL 60612, USA. Many experts consider PD to be stable when present for at least 12 months with 3–6 months
Email: drlevine@hotmail.com of stability.12 In contrast, severe pain rarely persists beyond the acute phase. Treatment varies
Received 19 September 2019; depending on the disease phase.12
accepted 27 February 2020. PD typically occurs during the fifth to sixth decade of life, but can occur at any age.13
Studies have suggested that PD prevalence might be as high as 9% in the general population,
and higher in patients with diabetes or after radical prostatectomy.14–17 However, Shiraishi
et al. found a much lower prevalence of 0.6% in a Japanese cohort.18 In addition to sexual
dysfunction, PD also has a significant impact on quality of life and psychological well-being
for the man and his partner.19 PD is frequently encountered by urologists in practice, and as a
result of increased awareness and the availability of new treatment options, the number of
men presenting for treatment will likely increase in the coming years. Thus, a general
© 2020 The Japanese Urological Association 1
MJ ZIEGELMANN ET AL.
understanding of its evaluation and treatment is mandatory. in the acute or chronic phase, which has important treatment
Herein, we provide a general overview of PD for the practic- implications. There is controversy regarding whether ED predis-
ing urologist. poses to PD or vice versa. Penile buckling or “hinge” effect,
wherein the penis bends on itself at the area of deformity as a
PD: Initial evaluation and adjunctive result of axial pressure, is also common. This might result from
testing ED, but is also seen with severe penile deformity.
The penis should be palpated along its entire length from
The initial evaluation should include a thorough history and the pubis to the glans, identifying areas of thickening or pla-
physical examination.12 If possible, the patient’s sexual part- que. SPL is typically measured from the pubis to coronal sul-
ner should be involved in the conversation.20 Important ele- cus. If symptoms of hypogonadism are present, an early
ments of the history/examination are summarized in Table 1. morning total testosterone is recommended.25 Fasting serum
PD evokes significant psychological burden, and all patients glucose, hemoglobin A1c, complete blood count and lipid
should be queried about their emotional well-being.19 The panel might be considered to identify underlying ED risk fac-
PDQ was developed and validated to assess psychosocial out- tors.26 In those endorsing penile sensitivity or risk factors for
comes with PD that might not be adequately captured with neuropathy (e.g. diabetes), biothesiometry is a useful adjunct
alternative metrics.21 The PDQ includes questions in three to record baseline sensory deficits.27
specific domains: (i) psychological and physical symptoms; If minimal bother is reported, no further evaluation is nec-
(ii) penile pain; and (iii) symptom bother. This should be essary. In contrast, those desiring active treatment must
considered as part of the initial work-up to quantify symptom undergo curvature assessment with ICI of an erectogenic
bother and subsequently assess treatment effect.22 agent.12 Patient-provided photographs are an alternative, but
ED is also seen in up to half of men with PD.23,24 Symptom are associated with significant inter/intra-observer variabil-
onset, progression and stability determine whether the patient is ity.28,29 Penile duplex Doppler ultrasound might be carried
out to assess vascular hemodynamics and the degree of plaque
calcification, which has important treatment implications.30,31
Table 1 Important elements of the history and physical examination in a
man presenting with PD
PD treatment
History Laboratory testing (as indicated)
• Pain (flaccid or erect) • Prostate-specific antigen
Treatment options depend on the degree of bother, sexual
• Curvature • Complete blood count
function limitations and symptom stability. In patients with
• Indentation • Fasting serum glucose or
minimal bother, observation alone is reasonable. Few studies
• Shortening hemoglobin A1c have evaluated the natural history of untreated PD. Separate
• Penile instability (“buckling”) • Lipid profile studies from Gelbard and Mulhall using starkly different
• ED • Total testosterone methodology found similar rates of symptom improvement
• Symptom duration
(~12–13%), stabilization (40–45%) and progression (42–
and/or stability 48%) with observation alone.23,32 Patients should be moni-
• Psychological bother tored for symptom progression, at which time active treat-
ment might be warranted.
Questionnaires Adjunctive testing (as indicated)
Historically, men in the acute phase were recommended
• PDQ Biothesiometry (subject changes
in penile sensation) observation or oral monotherapy for at least 6–12 months.
• International Index of
Formal curvature assessment† However, during the past several decades, a variety of alter-
Erectile Function
• Erection Hardness Score • Curvature assessment with native treatments have been studied for early PD. Specifi-
• Patient Health Questionnaire-9
goniometer cally, PTT and ILI might halt progression and allow for
• Point of maximum curvature improvement in curvature and length.33,34 Early intervention
Physical examination • Penile torsion might also prevent the need for invasive treatment, such as
Penis: • Indentation or hourglass penile straightening, or facilitate a less invasive approach.
• Penile elasticity
deformity Surgical straightening with plication or grafting should only
• SPL (pubis to corona)
• Hinge effect‡ be carried out once the patient has entered the “chronic”
• Presence of “plaque”
Penile duplex Doppler ultrasound
phase to limit the risk for deformity recurrence.35 A caveat to
(scar) – location, length
• Presence of penile plaque this principle is that patients with ED refractory to oral medi-
(tunical thickening)
cations might undergo penile prosthesis placement during the
Testicles/scrotum: • Cavernosal artery vascular
active phase to stabilize the PD and prevent further deformity
• Inguinal – lymphadenopathy, hernia assessment
a Peak systolic velocity
and shortening. In the following section, we will review the
General cardiovascular evaluation
b End diastolic velocity
various treatment options for PD.
c Resistive index
Non-invasive therapy
†Evaluation of the erect penis after administration of erectogenic medica-
tions (alprostadil, phentolamine, papaverine) or vacuum erection device.
Oral agents
‡Penile instability or “buckling” when axial pressure is applied to the erect There is no strong evidence to date that supports the use of
penis.
oral monotherapy for PD. The AUA and CUA guidelines on
2 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
PD recommend against oral therapy with vitamin E, tamox- and curvature. Further studies are necessary before this treat-
ifen, omega-3-fatty acids, procarbazine and vitamin E/L-car- ment can be considered standard of care.
nitine combination.12,36 Non-steroidal anti-inflammatories are
indicated for penile pain, particularly in the early phase.12
SWT
Data on other agents, such as para-amino-benzoate, L-argi-
nine/citrulline, pentoxifylline and colchicine, are limited by A shockwave is a mechanical disturbance that propagates
suboptimal study methodology.12,36 Despite this, many through a medium and carries energy.53 Several devices are
experts continue to recommend oral therapy because of the available to apply local SWT to the penis, and have been
low cost, minimal side-effects, and potential efficacy sug- hypothesized to cause mechanical disruption leading to scar
gested by in vitro and animal studies.37,38 Recently, there has remodeling and lysis. A meta-analysis found that SWT for
been growing interest in daily PDE5I therapy.39 In vitro and PD improves penile pain and plaque volume, without signifi-
rat model studies have shown that PDE5Is might actually cant impact on curvature.54,55 As a result of significant
decrease PD plaque through alterations in fibroblast activity, methodological flaws, the true impact of SWT on PD remains
decreased collagen deposition and local apoptosis.40,41 unclear, and further research is required. Furthermore, no ran-
Pentoxifylline, another commonly used agent, acts through domized trials examining the efficacy of low-intensity SWT
non-selective phosphodiesterase inhibition, and has been sug- (such as that used to treat ED) have been reported. In the
gested to modify PD scarring through its effects on nitric meantime, both the AUA and CUA support the use of SWT
oxide. Ultimately, multimodal therapy with oral and other for penile pain as a result of PD, but not penile curva-
treatments might yield the best results.42 Our standard proto- ture.12,36
col utilizes a combination of pentoxifylline 400 mg t.i.d.,
L-citrulline 750 mg b.i.d. and tadalafil 5 mg daily (if concur-
Mechanical therapy
rent ED is present).41
Mechanical therapy refers to the application of force to the
penis by external PTT or VT. This induces a process known
Topical therapy
as “mechanotransduction.” Traction was originally used in
Several topical agents have also been investigated. Verapamil the Dupuytren’s contracture population.56 In contrast to the
is a calcium channel blocker commonly used to treat hyper- traditional “bench-to-bedside” paradigm, mechanical therapy
tension, angina pectoris and headaches, which prevents pro- was studied in the clinical realm for PD and only later with
line incorporation into the extracellular matrix protein within basic science studies.57,58
scar tissue.43–45 This causes upregulation of collagenase by PTT might be used as monotherapy or as part of a treat-
fibroblasts.45,46 To date, in vivo studies examining topical ment protocol with oral therapy and ILI. The first published
verapamil have shown variable results. One study randomized report was a 2008 pilot study by our group involving 10
57 men to verapamil, trifluoperazine (a calmodulin blocker) patients who utilized PTT for 2–8 h daily for 6 months.59 All
and magnesium sulfate (weaker calcium channel patients had objective curvature improvement (10–45°) along
blocker).47 The authors reported subjective curvature with improvements in SPL (0.5–2 cm). A subsequent study
improvement in >90% of men, but lacked objective measure- by Gontero et al. reported a mean 1.3-cm SPL increase,
ments.47 Furthermore, Martin et al. found that topical vera- although curvature was not significantly changed (31° pre-
pamil does not aggregate in detectable levels within the treatment and 27° post-treatment).60 A larger, prospective
tunica.48 study of 96 men with acute phase PD compared PTT with no
EMDA utilizes an electrical charge gradient to promote tis- intervention and found a mean 20° decrease in the PTT group
sue penetration, and has been studied as a means to promote at 9 months, compared with objective worsening in the con-
transdermal drug delivery. Our group identified low, but trol group.33 Symptom duration <3 months and starting cur-
detectable, levels of verapamil within the tunica albuginea vature <45° were associated with better outcomes.
after EMDA.49 Di Stasi et al. reported a significant decrease Traction duration appears to play an important role in out-
in penile curvature from 43° to 21° with verapamil + EMDA, comes. Abern et al. found that patients who utilized PTT for
compared with no change in a placebo group.50 In contrast, a ≥3 h daily, in conjunction with intralesional verapamil and
small (n = 42) randomized placebo-controlled trial showed oral L-arginine/pentoxifylline, had mean SPL improvement of
no significant difference in the number of patients who expe- 0.6 cm compared with 0.7-cm loss in those who used PTT
rienced curvature improvement with verapamil + EMDA <3 h.42 A study by Yafi et al. similarly reported that PTT
(65%, mean improvement 9.1°) versus control (58%, mean use >3 h per day was associated with improved SPL for men
improvement 7.6°).51 Because of a lack of supportive data, receiving intralesional interferon.61 In contrast, Ziegelmann
and the relatively burdensome administration protocol, et al. did not find any significant difference in outcomes
experts recommend against verapamil + EMDA.12 based on PTT duration in a cohort of patients who underwent
Another recent study reported outcomes in a small cohort intralesional CCH with or without concurrent PTT.62 Nota-
of patients randomized to topical placebo versus “H-100” gel, bly, just 25% of patients used PTT for the recommended
a novel compound consisting of nicardipine, superoxide >3 h daily, emphasizing the real-world challenges inherent
dismutase and emu oil (purported to enhance tissue penetra- with PTT.
tion).52 The study was underpowered, but patients in the A recent study by Moncada et al. randomized patients with
“H-100” cohort experienced significant improvements in SPL PD (symptom duration ≥1 year and no prior treatment) to
© 2020 The Japanese Urological Association 3
MJ ZIEGELMANN ET AL.
PTT with the Penimaster Pro (MSP Concept, Berlin, Ger- concluded that the evidence to support ILI verapamil is less
many) or no traction for a period of 12 weeks.63 Patients robust when compared with other intralesional agents, such as
were instructed to use the device for 3–8 h daily. A total of IFN and CCH.65 However, due to modest yet favorable
80 patients completed the study protocol and were available results, low cost and lack of severe side-effects, verapamil is
for follow up. The mean curvature improvement was 31° in still utilized by many authorities as first-line therapy, particu-
the PTT cohort. Patients who utilized the device <4 h a day larly in the acute phase or in those with active pain.12
experienced a mean curve improvement of 20° compared
with 38° in those who used PTT >6 h per day. There were
IFN alfa-2b
also significant improvements in SPL.22,63 Limitations include
that only patients who complied with recommended PTT IFN exerts its effects on PD plaque by concentration-depen-
duration were included in the analysis (as-treated), and the dent fibroblast inhibition and decreased collagen production
cohort included only patients with uniplanar curvature >45° (upregulated collagenase activity).72 Wegner et al. first
without indentation deformity who had not undergone prior reported their experience with intralesional IFN in 1995.73 A
therapy. Another study by Ziegelmann et al. evaluated out- subsequent pilot study by Ahuja et al. (n = 20) found that
comes with a new traction system known as the Restorex pain resolved in 90% of patients, with curvature improving in
(Pathright Medical, Plymouth, MN, USA).64 A total of 100 20–90% of patients (mean 65%).74 Later, Hellstrom et al.
patients were randomized to PTT daily for 30–90 min versus carried out a multicenter, single-blind, placebo-controlled
no traction for 3 months. Using an intent-to-treat analysis, the study comparing intralesional IFN (5 million units in 10 cc
authors reported a significant improvement in penile curva- of saline administered every other week; n = 50) with pla-
ture (!11.7° vs +1.3°) and SPL (+1.5 cm vs 0 cm) when cebo (n = 53), finding a mean penile curvature improvement
comparing patients in the treatment arms with controls. More of 13.5° (27%) in the IFN group compared with just 4.4°
than 75% of patients showed an improvement in curvature, (9%) in the placebo group (P < 0.001).75,76 Pain improved in
and nearly 95% had an improvement in SPL. To date, this is 67% of IFN patients compared with 28% of controls. A com-
the most rigorous study on PTT and the first study to show parison of men treated with IFN for dorsal and ventral pla-
improvements with PTT duration <3–8 h daily. Ultimately, ques showed similar outcomes, with >50% having ≥20%
further data are required to determine the long-term sustain- improvement in penile curvature.77 Side-effects with IFN are
ability of these and other published results. With documented mild-to-moderate, and include ecchymosis, pain, sinusitis,
efficacy in both acute and chronic PD, as well as evidence fever, chills and arthralgias.75 These tend to be short-lived
supporting length restoration and girth improvement, traction and adequately managed with anti-inflammatory medications.
therapy should be recommended to virtually all patients with Based on data from two randomized, placebo-controlled tri-
PD. als, intralesional IFN provides modest improvement in penile
curvature and might hasten penile pain improvement.75,76
Intralesional injections
Collagenase Clostridium histolyticum
ILI therapy refers to the process of injecting medication
directly into plaque, representing a less invasive treatment CCH (Xiaflex; Endo Pharmaceuticals, Dublin, Ireland) is the
modality with proven benefits.65 There are also data to sup- newest intralesional agent available, and has gained consider-
port ILI for penile pain and possibly even girth and length able interest since the original phase III study was published
recovery when used in combination with other treatment in 2013.7 CCH breaks down collagen types I/III, which are
modalities.42,66 During the past several decades, a variety of the main components of PD plaque. CCH is also used to treat
ILI agents, including hyaluronic acid, botulinum toxin and Dupuytren’s contractures.78,79 The original clinical applica-
thiocolchicine, have been studied. However, the most com- tion of CCH to PD dates back to 1985, when Gelbard et al.
mon agents used in clinical practice today include verapamil, published a phase I single-arm trial; prior in vitro studies
IFN and CCH (Table 2).65 served as the foundation for this innovative work.80,81 A sub-
sequent phase IIb study randomized patients to CCH versus
placebo with and without provider-applied manual modeling
Verapamil
(bending the flaccid penis in the direction opposite the curva-
In 1994, our group first used intralesional verapamil in a non- ture).82 The authors identified a significant improvement in
randomized dose-escalating study of 14 PD patients.67 Subjec- penile curvature in those who underwent CCH with modeling
tive improvements in narrowing and curvature were reported (mean 17.5° or !32%) compared with those who underwent
in 100% and 43%, respectively. A subsequent study reported placebo and modeling (mean 0.6° or +2.5%; P < 0.001).
outcomes for 140 men, with average curvature improvement Interestingly, there was no significant difference between
of 17° and >80% reporting girth improvement.68 A prospec- CCH and placebo in the patients randomized to the non-mod-
tive series found that >95% of men showed improvement or eling arm, emphasizing the importance of modeling itself.
resolution of penile pain as well.69,70 In contrast, Shirazi et al. Phase III data once again showed a significantly greater
failed to identify a difference in curvature or pain between improvement in curvature for those who underwent CCH
patients undergoing verapamil and saline control.71 Side-ef- (!17° or !34%) compared with placebo (!9° or !18%;
fects are generally mild, and include transient pain (mitigated P < 0.0001), along with greater improvement in the patient
by penile block) and bruising. A recent systematic review bother domain of PDQ.7 The original data from the phase III
4 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
Table 2 Randomized, placebo-controlled trials for intralesional therapy with CCH, IFN and verapamil
Post-treatment Change in penile
Intralesional Baseline penile penile curvature curvature, mean
Study Design agent Patients curvature (degrees) (degrees) (degrees) Follow up
Gelbard Randomized, CCH CCH (n = 401) CCH: 50.1 (SD 14.4) CCH: 33.1 (SD 16.8) CCH: !17.3 52 weeks
et al.7 double-blind, Placebo (n = 211) Placebo: 49.3 (SD 14.0) Placebo: 40.0 (SD 16.2) Placebo: !9.3
placebo-controlled
Hellstrom Randomized, single-blind, IFN IFN (n = 50) IFN: 49.9 (SD 2.4) IFN: 36.4 (SD 2.1) IFN: !13.5 >4 weeks
et al.75 placebo-controlled Placebo (n = 53) Placebo: 50.9 (SD 2.5) Placebo: 46.4 (SD 2.2) Placebo: !4.5
Shirazi Randomized, Verapamil Verapamil (n = 40) Verapamil: 49.7 (SD 9.3) Verapamil: 47.6 (SD 7.3) Verapamil: !2.1 24 weeks
et al.71 placebo-controlled Placebo (n = 40) Placebo: 45.6 (SD 9.7) Placebo: 43.4 (SD 8.9) Placebo: !2.2
Rehman Randomized, Verapamil Verapamil (n = 7) Verapamil: 37.7 (SD 9.3) Verapamil: 29.6 (SD 7.3) Verapamil: !8.1 3 months
et al.157 single-blinded, Placebo (n = 7) Placebo: 33.6 (SD 9.7) Placebo: 31.4 (SD 8.9) Placebo: !2.2
placebo-controlled
studies included patients with dorsal or dorsolateral penile Also, a post-approval study from Tsambarlis et al. found less
curvature of 30–90° in the chronic phase (>12 months since promising results in a cohort of 45 men who underwent CCH
diagnosis with “stable” disease).7 Exclusion criteria included with a mean reduction of curvature of 5.4°.87 In comparison,
isolated hourglass penile deformity, ED, ventral curvature many series reporting results for surgical straightening with
and significant plaque calcification. Subsequent series have plication or grafting techniques have found success rates,
reported improvements ranging from 5° to 26°, with less defined by most authorities as a “functionally” straight penis
stringent inclusion criteria.79 A multicenter retrospective ser- with residual curvature <10–20°, in excess of 90%.35 This is
ies of 918 patients found a mean improvement of 15.3°, with true even in the setting of relatively complex deformities. Not
nearly 70% of patients having >20% curvature improvement. surprisingly, a recent prospective analysis comparing CCH
Attempts to identify those patients most likely to respond to with TAP and partial excision and grafting found superior
CCH have been limited, but data suggest that lack of plaque curvature correction with surgical straightening.88
calcification, greater disease duration and higher baseline Another important consideration is the potential side-ef-
International Index of Erectile Function scores might be asso- fects associated with CCH. Penile ecchymosis and swelling
ciated with better results.30,83 Currently, based on our exten- are seen in up to 80% and 55% of patients treated with CCH,
sive experience with ILI, we recommend CCH for patients respectively. Significant penile hematoma and overt corporal
with mild-to-moderate curvature (<60°) who have an acute rupture are, thankfully, quite rare, with reported incidence
angle of curvature (rather than an extended crescent-type ranging from 0.5–5% and 0.8–1.4%, respectively.75,89
curve) and minimal plaque calcification.84 Although many providers encounter these complications,
The original CCH protocol involved up to four injection there is no consensus on management strategies. Hematomas
cycles.7 Each cycle consists of two injections of 0.58 mg might be managed with observation, local compression and
CCH directly into the PD plaque, with an interval between aspiration if associated with discomfort. Some experts closely
injections of 1–3 days. Patients were instructed to carry out observe patients in the setting of possible CCH-associated
manual modeling daily during the 6-week interval between corporal rupture, yet approximately two-thirds of surveyed
treatment cycles. Recently, several modified protocols have Sexual Medicine Society of North America members advo-
been reported. Abdel Raheem et al. administered a larger cated for surgical management.90 Notably, surgical planes
dose (0.9 mg) once every 4 weeks for a total of three injec- and tissue quality are altered, so surgeon expertise is manda-
tions combined with manual modeling at home and VT.85 tory if operative intervention is undertaken.91
They found a mean improvement in penile curvature of 17° In conclusion, many patients with PD, and, in particular,
or 34%. Adjunctive PTT might also increase treatment effi- those with mild-to-moderate penile deformity, are hesitant to
cacy. Alom et al. reported a mean 34° improvement in a undergo surgical straightening. ILI might provide modest
cohort of patients who utilized daily PTT (with the Restorex improvement in penile curvature, pain, and other types of
traction system) concurrently with CCH treatment.66 This deformity, such as girth loss. To date, no head-to-head com-
was significantly greater than those patients who elected to parisons between CCH and other intralesional therapies have
forego PTT (20°). Finally, recent reports suggest that CCH been published, and future work is necessary to elucidate
has a positive impact during the acute phase and in those those patients who are most likely to benefit from ILI, which
with ventral curvature.34,86 is particularly relevant given the real cost and time commit-
Despite the ongoing enthusiasm for CCH, it is worth not- ment with these treatments.
ing that even in the CCH arm of the phase III trials just 46%
of patients met the predefined criteria of “composite respon-
der,” which was defined as a ≥20% improvement in curvature
Surgery
and >1-point PDQ bother score reduction, or change from For the patient with bothersome penile curvature or severe
reporting no sexual activity at screening to sexual activity.7 indentation deformity that limits the ability to engage in
© 2020 The Japanese Urological Association 5
MJ ZIEGELMANN ET AL.
Peyronie’s Disease
Symptom Duration > 1 year Symptom Duration < 1 year
or
Deformity Stable > 3-6 months Deformity Stable > 3-6 months
“Chronic Phase” “Acute Phase”
No Treatment Options:
Does Patient Desire Surgery?
• Observation
Yes • Oral Therapy
• Traction
Erectile Function • Intralesional injections
Good Non-reponsive to PDE5 inhibitors
Penile Curvature > 60º? Penile Prosthesis Insertion
Indentation Deformity? +/- Straightening Maneuvers
• Notching • Manual Modelling
• Hourglass • Plication
• Hinge-effect • Incision & Grafting
• Length Restoration
No Yes
Yes
Penile Plication Procedure Risk Factors for ED Present
No
Tunical Incision/Excision and Grafting Procedure
(May consider if ED risk factors present, but must discuss risk of worsened ED)
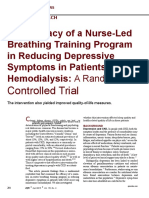
Fig. 1 General algorithm for PD treatment based
on symptom duration and stability.
satisfactory penetrative intercourse, surgery remains the most during an erection. This approach is indicated for those men
rapid and reliable treatment option. The majority of surgeons, with relatively mild-to-moderate curvature (<60–70°), satis-
even amongst those with expertise in sexual medicine, carry factory preoperative erections with or without oral therapy,
out <10 penile plications and penile grafting procedures per and the absence of penile instability (i.e. buckling when axial
year.92 This is due in part to referral patterns and practice pressure is applied to the penis such as during penetrative
centralization. Concerns regarding the risk for postoperative sexual intercourse).
complications and patient dissatisfaction might also drive Corporoplasty refers to full-thickness excision of tunical
some providers to alternative, less invasive (but also less tissue and subsequent closure with a non-absorbable suture.
definitive) treatment options, such as ILI. The surgical The original approach described by Nesbit involved excision
approach is dependent on a variety of factors including penile of an elliptical segment of the tunica albuginea along the cor-
deformity (curvature, indentation, hinge effect) and baseline pora opposite the area of maximal curvature, with the defect
erectile function (Fig. 1). It is generally agreed upon that sur- closed in a running fashion.94,95 Yachia modified this
gical straightening should be carried out only after the patient approach by making a longitudinal incision and that was
enters the chronic phase of the disease.92 closed horizontally.96 In contrast, true “corporal plication”
refers to suture placement with full-thickness tunical incision.
In 1985, Essed and Schroeder described their plication tech-
Penile plication or corporoplasty
nique using non-absorbable sutures to bunch or “plicate” the
Penile plication or corporoplasty, also referred to as “shorten- corporal tissue.97 Knispel et al. subsequently modified this
ing” procedures, are broadly categorized into incisional or technique by inverting the sutures to minimize palpabil-
excisional corporoplasty, and non-incisional plication.93 All ity.97,98
are based on the principle that shortening the convex-side TAP was adapted by Levine from the approach described
opposite the area of curvature will pull the penis straight first by Baskin and Duckett in 1994 to treat pediatric
6 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
(a) (b)
Fig. 2 TAP is carried out by excising a portion
of the outer longitudinal tunical fibers and
maintaining the inner circular fibers in the area
opposite to the point of maximum penile
curvature. (a) A 2-0 permanent suture is then
used to bring the edges of the excised tissue
together (b) in a manner that buries the suture
knot.
chordee.99,100 With this technique, partial thickness incisions by carrying out adjunctive maneuvers, such as preoperative
(0.5–2 cm in length and maximum distance 0.5–1 cm and postoperative PTT.99,106,107 To date, there is no strong
between incisions) are made transversely through the outer evidence to support one incisional/excisional corporoplasty or
longitudinal tunical fibers in the area opposite the curvature, plication technique over another with respect to optimizing
with care taken to preserve the inner circular fibers (Fig. 2). postoperative outcomes. Thus, based on expert opinion, the
The intervening longitudinal fibers are sharply excised so as operative approach should be left to the discretion of the sur-
to reduce tissue bulk between the incisions. The incisions are geon.18
then approximated with a permanent suture using a near-far,
far-near approach (inverting vertical mattress) to bury the
Plaque incision or partial excision with
knot. This suture is then reinforced using two adjacent
grafting
absorbable 3-0 PDS sutures (Johnson and Johnson, New
Brunswick, NJ, USA) in a Lembert fashion. The 16-dot plica- Plaque incision or partial excision with grafting is reserved
tion popularized by Lue involves placement of a non-ab- for men with excellent baseline erectile function, more severe
sorbable braided-suture along the tunica on the convex side curvature (>60–70°) and/or significant penile indentation or
of the penis in an extended Lembert fashion.101 In the setting hourglass deformity that creates a hinge effect.19 Grafting
of a broad “banana-type” curvature, more “dots” might be might also be considered for men who have significant con-
necessary to completely correct the curvature.93 Finally, cerns about penile shortening and more moderate deformities.
Morey reported excellent results with plication using non-ab- Patient selection is of the utmost importance with grafting
sorbable braided suture placement through a small 2-cm procedures. Because of the increased risk for postoperative
penoscrotal incision.102 ED, patients with severe deformity and baseline ED (such as
Success rates reported in the literature vary widely due in those with poor rigidity despite PDE5Is) should be encour-
part to significant variation in follow-up duration, the defini- aged to pursue penile prosthesis placement with concurrent
tion of success and the type of surgical approach. Successful straightening maneuvers. Notably, ventral grafting might pre-
straightening postoperatively ranges 29–100% with overall dispose patients to increased risk for postoperative ED, and
patient satisfaction ranging 65–96%.35 Palpable knots are some experts advocate against grafting procedures for sev-
reported in 50–100% of procedures, but significant bother ere ventral and ventrolateral curvature.110
associated with this palpability is substantially lower, ranging The decision to carry out plaque incision versus partial pla-
0–20%.35,93,103 Some authors have also reported satisfactory que excision is highly surgeon dependent. During plaque
success rates with absorbable sutures to further minimize knot incision, the surgeon creates a “modified-H” or “double-Y”
palpability while maintaining adequate straightening.14,105 tunical defect at the point of maximal curvature.111 In con-
Penile shortening is a major concern for most patients. trast, partial plaque excision involves the removal of a seg-
Subjective length loss is reported in up to 75% of patients ment of diseased tunic from the area of greatest deformity,
postoperatively, whereas objective loss, as determined by var- either as an elliptical or a rectangular segment.112,113 To date,
ious provider-performed assessments of penile length, is seen no head-to-head trial has compared outcomes between these
in 20–40% of patients.93 Shortening is more common in men two approaches. Advocates of plaque incision emphasize the
with ventral and ventrolateral penile curvature, and in those smaller defect size that can be created – small series have
with more severe curvature (>60°).99 This might be mitigated suggested that larger grafts (in excess of 2–4 9 5 cm) might
© 2020 The Japanese Urological Association 7
MJ ZIEGELMANN ET AL.
be associated with a higher risk for postoperative ED, pre- greater expense, but allow for shorter operative times without
sumably as a result of veno-occlusive dysfunction.110,114 the risk for complications related to graft harvesting. Our pre-
Advocates of partial plaque excision emphasize the ability to ferred graft is the Tutoplast (Coloplast Corporation, Humle-
restore more uniform penile girth with indentation deformi- baek, Germany) processed human pericardium, because it is
ties, which in severe cases might result in penile instabil- readily available, thin yet strong and in our extensive experi-
ity.113 Furthermore, in the case of a more broad-based penile ence is less prone to contraction (Fig. 3). Recently, Hatzi-
curvature, plaque incision alone might not fully correct the christodoulou has popularized the use of an equine collagen
deformity, resulting in the need for plication sutures or even fleece known as TachoSil (Baxter, Deerfield, IL, USA).120
multiple tunical incisions (and thus multiple separate The purported benefit of this graft is the ability to apply the
grafts).115 material directly over the tunical defect without suturing it
Graft selection is an area of ongoing debate, and a compre- into place, saving significant time in the operating theater.
hensive description of the various graft types is beyond the Yet, there are concerns regarding the ability to assess penile
scope of the current review. To date, there are no strong straightness intraoperatively. Longer-term follow up and mul-
comparative data to support the superiority of one graft over ti-institution validation are necessary before this approach can
another. The exception to this statement is with synthetic be considered standard of care.
grafts, which are associated with marked inflammation, fibro- The majority of studies consist of single-institution retro-
sis and even graft infection.116,117 Therefore, synthetic grafts spective series focusing on single graft types, thereby limiting
are no longer advocated as first-line treatment. PD grafts can the reliability of results reported in the currently available lit-
be generally categorized into autologous and non-autologous erature. Successful penile straightening, defined by some
materials.35,118,119 Autologous grafts, such as dermis, saphe- authorities as a “functionally straight” penis with residual cur-
nous vein, oral mucosa, tunica vaginalis and fascia lata, are vature <20–30°, is often based on subjective reporting. Suc-
readily available and do not pose the theoretical risk for graft cess rates range from 55 to 100%, and this might actually
rejection. However, increased operative times, graft contrac- decrease over time.118,121 Patient satisfaction rates, which
tion and harvest site complications are a concern. In contrast, take into account not only straightness, but also other aspects,
non-autologous “off the shelf” xenografts and allografts add such as postoperative penile length and erectile function, are
similarly variable, ranging from 60 to 100%.35 Postoperative
complications that compromise patient satisfaction include
perceived penile shortening (0–90%) and penile sensory
changes (0–22%).35,118,122 Sensory changes are transient in
the majority of patients, and a recent report from Terrier
et al. found that, although 20% of men experienced some
degree of glans hypoesthesia at 1 month after grafting, just
3% had persistent deficits at 12 months postoperatively.122,123
Subjective and objective penile length loss can also be
allayed by postoperative penile rehabilitation with PTT or
VT.17,124
Arguably, the most feared postoperative complication is
ED, which is reported in 0–63% in modern series.35,118 Sug-
gested risk factors include greater penile curvature, older age
and larger graft size.110,125 In our extensive experience with
partial plaque excision, we did not identify any significant
Graft difference in the rate of postoperative ED based on graft size
or baseline medical comorbidities.126,127 In fact, the best pre-
dictor of postoperative erectile function is strong and reliable
preoperative erections.127 Ventral graft placement, which
requires urethral mobilization, has also been suggested as an
independent risk factor for postoperative ED.13,110 Therefore,
in the setting of severe ventral curvature, where plication
alone is unlikely to result in satisfactory curvature correction,
penile prosthesis placement with concurrent straightening
maneuvers should be strongly considered.
Penile prosthesis placement with
straightening maneuvers
Fig. 3 Complete straightening is achieved with partial plaque excision and
Penile prosthesis placement with straightening maneuvers
grafting using a Tutoplast human pericardium graft. This approach is indi- allows for satisfactory penile straightening along with reliable
cated for patients with more severe penile curvature (>60–70°, severe inden- penile rigidity.26,109 Prosthesis placement might also be con-
tation or “hinge effect,” or penile shortening). sidered in men with more severe penile curvature (>60–70°,
8 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
significant indentation deformity resulting in hinge effect) current of ≤30 Watts to prevent injury to the underlying
who would otherwise be candidates for grafting procedures, cylinders.140 Incision alone might be all that is necessary, but
but have significant baseline medical comorbidities known to placement of a graft is recommended if the defect is >2 cm
increase their risk for developing ED over time (i.e. hyperten- in greatest dimension, particularly if using an inflatable
sion, hyperlipidemia, diabetes, tobacco use etc.), or in those device – a larger defect might predispose to device aneur-
with severe ventral curvature as a result of the significant risk ysm.141 The graft itself also helps with hemostasis and
for postoperative ED posed by ventral grafting, as previously reduces bothersome cicatrix formation, without increased risk
noted.26,110,128 of device failure or infection.134 Any of the traditional autolo-
The IPP is favored for men with PD because of concerns gous and non-autologous grafts can be used, but because of
regarding persistent deformity, lack of girth enhancement, increased operative times and the risk for damage to the
limited concealment and even partner dissatisfaction, but underlying cylinders with suture placement, there is now a
recent work has found reported high patient satisfaction rates trend toward utilizing sutureless grafts or “patches,” such as
with malleable prostheses as well.129–131 This has important Tachosil or Evarrest (Ethicon, Somerville, NJ, USA), a cellu-
implications, as malleable devices are more accessible and lose mesh containing thrombin and fibrinogen (Fig. 4).142,143
less expensive in some regions of the world. A comparison These materials are hypothesized to provide structural support
between the Coloplast Titan (Coloplast Corporation) and and ingrowth of native tissue in the area of plaque incision.
AMS CX 700 (Boston Scientific, Marlborough, MA, USA) In a manner similar to grafting without a prosthesis, this
showed similar outcomes with respect to penile straightening approach requires mobilization of Buck’s fascia (for dorsal or
and patient satisfaction (nearly 80%).132 In contrast, because lateral curvatures) or the urethra (for ventral curvatures).
of the intrinsic properties that allow for girth and length Thus, patients should be counseled regarding the possibility
expansion, the AMS LGX IPP (Boston Scientific) might actu- of temporary or permanent (albeit rare) glans hypoesthe-
ally exacerbate penile deformity, and this model is not rec- sia.120,144
ommended for men with PD.133 Satisfaction rates with penile prosthesis placement in the
Penile prosthesis placement alone might correct the defor- modern literature often exceed 80–90% for patients and their
mity in relatively mild cases, but additional straightening
maneuvers are required in 30–95% of patients.134–136 Once
again, defining “successful” straightening is not straightfor-
ward. We found that >25% of all patients undergoing IPP
plus straightening maneuvers were dissatisfied with their
penile straightness postoperatively.134 This was despite
achieving a “functionally straight” result (<20° residual cur-
vature) in the operating room in all cases. It is therefore criti-
cal to discuss the patient’s acceptance of functional
straightness (within 20° of straight, as opposed to “arrow”
straightness) during preoperative counseling. When residual
curvature is present, a variety of intraoperative maneuvers are
utilized. Wilson and Delk were the first to describe manual
modeling for residual curvature beyond 20–30° after IPP.137
With this technique, the penis is forcefully bent in the direc-
tion opposite the curvature while the prosthesis cylinders are
maximally inflated. Several series have reported success rates
ranging from 80 to 100%, yet there is a known risk for ure-
thral injury (perforation of the fossa navicularis as a result of
excessive pressure on the distal cylinder tips).133–134,137
Penile plication sutures, placed before the cylinders, are
another approach to address moderate residual curvature.138.
If adequate curvature correction is achieved through prosthe-
sis placement alone, the sutures can simply be removed.
Notably, although plication might correct penile curvature,
this approach could result in further penile shortening, which
is already a significant concern for most men undergoing
penile prosthesis.139 Furthermore, plication will not address
severe indentation deformity and has the potential to actually
exacerbate penile instability, even with the added rigidity of
the prosthesis.
Fig. 4 Penile prosthesis placement followed by plaque incision and hemo-
Plaque incision with or without grafting should be consid- static patch placement in a patient with coincident severe ED and PD. When
ered when there is residual curvature >30° or severe indenta- penile prosthesis placement alone does not result in satisfactory straightening,
tion deformity. An incision is made in the tunic overlying the adjunctive straightening maneuvers, such as manual modeling, penile plication,
prosthesis at the area of greatest deformity using coagulation and plaque incision and grafting (shown here), might be required.
© 2020 The Japanese Urological Association 9
MJ ZIEGELMANN ET AL.
partners.145-148 In their multicenter prospective series, Khera 5 De Rose AF, Mantica G, Bocca B, Szpytko A, Van der Merwe A, Terrone
C. Supporting the role of penile trauma and micro-trauma in the etiology of
et al. found that >80% of PD patients reported feeling some-
Peyronie’s disease. Prospective observational study using the electronic
what or very satisfied with their IPP, and there was no signif- microscope to examine two types of plaques. Aging Male 2019; https://doi.
icant difference in the satisfaction rate when compared with org/10.1080/13685538.2019.1586870.
patients without PD.149 To date, there are no strong data to 6 Bjekic MD, Vlajinac HD, Sipetic SB, Marinkovic JM. Risk factors for Pey-
suggest that PD predisposes to adverse outcomes, such as ronie’s disease: a case-control study. BJU Int. 2006; 97: 570–4.
7 Gelbard M, Goldstein I, Hellstrom WJ et al. Clinical efficacy, safety and
infection or shortened device survival, even when modeling
tolerability of collagenase Clostridium histolyticum for the treatment of pey-
or grafting is carried out.134,150,151 However, prospective data ronie disease in 2 large double-blind, randomized, placebo controlled phase
comparing outcomes in men with and without PD are lacking 3 studies. J Urol. 2013; 190: 199–207.
and further study is required. 8 Del Carlo M, Cole AA, Levine LA. Differential calcium independent regu-
As a final note, the concept of penile length restoration lation of matrix metalloproteinases and tissue inhibitors of matrix metallo-
proteinases by interleukin-1beta and transforming growth factor-beta in
deserves special mention. Over the past decade, several tech-
Peyronie’s plaque fibroblasts. J Urol. 2008; 179: 2447–55.
niques have been developed and refined to optimize penile 9 Mateus M, Ilg MM, Stebbeds WJ et al. Understanding the role of adenosine
length in the setting of PD and prosthesis placement. Exam- receptors in the myofibroblast transformation in Peyronie’s disease. J. Sex.
ples include circumferential tunical grafting and the sliding Med. 2018; 15: 947–57.
technique, wherein hemicircular incisions are made along the 10 Bias WB, Nyberg LM Jr, Hochberg MC, Walsh PC. Peyronie’s disease: a
newly recognized autosomal-dominant trait. Am. J. Med. Genet. 1982; 12:
dorsal (proximal) and ventral (distal) corpora after elevation 227–35.
of the neurovascular bundle and urethra.152,153 These inci- 11 Al-Thakafi S, Al-Hathal N. Peyronie’s disease: a literature review on epi-
sions are then connected by bilateral longitudinal incisions demiology, genetics, pathophysiology, diagnosis and work-up. Transl.
with subsequent grafting, which might involve a substantial Androl. Urol. 2016; 5: 280–9.
12 Nehra A, Alterowitz R, Culkin DJ et al. Peyronie’s disease: AUA guideline.
amount of suturing if traditional graft materials are used.
J Urol. 2015; 194: 745–53.
Refinements to the sliding technique by Egydio et al. were 13 Tal R, Hall MS, Alex B, Choi J, Mulhall JP. Peyronie’s disease in teen-
developed to avoid the need for graft placement by utilizing agers. J. Sex. Med. 2012; 9: 302–8.
Buck’s fascia (MoST) or a smaller series of tunical defects 14 Mulhall JP, Creech SD, Boorjian SA et al. Subjective and objective analysis
(MuST).154,155 It must be emphasized that, although rare, of the prevalence of Peyronie’s disease in a population of men presenting
for prostate cancer screening. J. Urol. 2004; 171: 2350–3.
serious and irreversible side-effects, including glans necrosis,
15 Schwarzer U, Sommer F, Klotz T, Braun M, Reifenrath B, Engelmann U.
might occur with these approaches as a result of vascular The prevalence of Peyronie’s disease: results of a large survey. BJU Int.
compromise.156 Thus, length restoration procedures should 2001; 88: 727–30.
only be carried out by experienced surgeons after thorough 16 Tal R, Heck M, Teloken P, Siegrist T, Nelson CJ, Mulhall JP. Peyronie’s
patient counseling. disease following radical prostatectomy: incidence and predictors. J. Sex.
Med. 2010; 7: 1254–61.
17 Kadioglu A, Sanli O, Akman T et al. Factors affecting the degree of penile
deformity in Peyronie disease: an analysis of 1001 patients. J. Androl.
Conclusions 2011; 32: 502–8.
PD is a condition characterized by penile deformity, pain, 18 Shiraishi K, Shimabukuro T, Matsuyama H. The prevalence of Peyronie’s
disease in Japan: a study in men undergoing maintenance hemodialysis and
sexual dysfunction and psychological bother. The first step is routine health checks. J. Sex. Med. 2012; 9: 2716–23.
to characterize the presenting symptoms, disease duration and 19 Nelson CJ, Mulhall JP. Psychological impact of Peyronie’s disease: a
level of bother through a detailed history and examination. In review. J. Sex. Med. 2013; 10: 653–60.
a man who desires active treatment, a formal curvature 20 Davis SN, Ferrar S, Sadikaj G, Gerard M, Binik YM, Carrier S. Female
partners of men with Peyronie’s disease have impaired sexual function, sat-
assessment must be carried out to objectively characterize the
isfaction, and mood, while degree of sexual interference is associated with
penile deformity. Depending on the symptom severity, a vari- worse outcomes. J. Sex. Med. 2016; 13: 1095–103.
ety of treatment options, including PTT, ILI and surgical 21 Hellstrom WJ, Feldman R, Rosen RC, Smith T, Kaufman G, Tursi J.
straightening, are available with varying efficacy. Bother and distress associated with Peyronie’s disease: validation of the
Peyronie’s disease questionnaire. J. Urol. 2013; 190: 627–34.
22 Coyne KS, Currie BM, Thompson CL, Smith TM. Responsiveness of the
Conflict of interest Peyronie’s Disease Questionnaire (PDQ). J. Sex. Med. 2015; 12: 1072–9.
23 Mulhall JP, Schiff J, Guhring P. An analysis of the natural history of Pey-
Dr Laurence Levine is a consultant for Boston Scientific and ronie’s disease. J. Urol. 2006; 175: 2115–8.
Coloplast Corporation. The other authors declare no conflict 24 Burri A, Porst H. The relationship between penile deformity, age, psycho-
of interest. logical bother, and erectile dysfunction in a sample of men with Peyronie’s
disease (PD). Int. J. Impot. Res. 2018; 30: 171–8.
25 Burnett AL, Nehra A, Breau RH et al. Erectile dysfunction: AUA guideline.
References J. Urol. 2018; 200: 633–41.
26 Allen MS, Walter EE. Erectile dysfunction: an umbrella review of meta-
1 de la Peyronie F. Sur quelques obstacles qui s’ opposent a l’ejaculation nat- analyses of risk-factors, treatment, and prevalence outcomes. J. Sex. Med.
urelle de la semence. Mem. Acad. R. Chir. 1743; 1: 425–34. 2019; 16: 531–41.
2 Akkus E. Historical review of Peyronie’s disease. In: Levine LA (ed.). Pey- 27 Wiggins A, Farrell MR, Tsambarlis P, Levine LA. The penile sensitivity
ronie’s Disease. Humana Press, Totowa, 2007; 1–8. ratio: a novel application of biothesiometry to assess changes in penile sen-
3 Mohede DCJ, de Jong IJ, van Driel MF. Medical treatments of Peyronie’s sitivity. J. Sex. Med. 2019; 16: 447–51.
disease: past, present, and future. Urology 2019; 125: 1–5. 28 Ohebshalom M, Mulhall J, Guhring P, Parker M. Measurement of penile
4 Musitelli S, Bossi M, Jallous H. A brief historical survey of “Peyronie’s curvature in Peyronie’s disease patients: comparison of three methods. J.
disease.” J. Sex. Med. 2008; 5: 1737–46. Sex. Med. 2007; 4: 199–203.
10 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
29 Nascimento B, Cerqueira I, Miranda EP et al. Impact of camera deviation 53 Chung E, Wang J. A state-of-art review of low intensity extracorporeal
on penile curvature assessment using 2D pictures. J. Sex. Med. 2018; 15: shock wave therapy and lithotripter machines for the treatment of erectile
1638–44. dysfunction. Expert Rev. Med. Devices 2017; 14: 929–34.
30 Wymer K, Ziegelmann M, Savage J, Kohler T, Trost L. Plaque calcifica- 54 Gao L, Qian S, Tang Z, Li J, Yuan J. A meta-analysis of extracorporeal
tion: an important predictor of collagenase Clostridium histolyticum treat- shock wave therapy for Peyronie’s disease. Int. J. Impot. Res. 2016; 28:
ment outcomes for men with Peyronie’s disease. Urology 2018; 119: 109– 161–6.
14. 55 Krieger JR, Rizk PJ, Kohn TP, Pastuszak A. Shockwave therapy in the
31 Levine L, Rybak J, Corder C, Farrel MR. Peyronie’s disease plaque calcifi- treatment of Peyronie’s disease. Sex. Med. Rev. 2019; 7: 499–507.
cation–prevalence, time to identification, and development of a new grading 56 Brandes G, Messina A, Reale E. The palmar fascia after treatment by the
classification. J. Sex. Med. 2013; 10: 3121–8. continuous extension technique for Dupuytren’s contracture. J. Hand Surg.
32 Gelbard MK, Dorey F, James K. The natural history of Peyronie’s disease. 1994; 19: 528–33.
J. Urol. 1990; 144: 1376–9. 57 Chung E, De Young L, Solomon M, Brock GB. Peyronie’s disease and
33 Martinez-Salamanca JI, Egui A, Moncada I et al. Acute phase Peyronie’s mechanotransduction: an in vitro analysis of the cellular changes to Pey-
disease management with traction device: a nonrandomized prospective con- ronie’s disease in a cell-culture strain system. J. Sex. Med. 2013; 10: 1259–
trolled trial with ultrasound correlation. J. Sex. Med. 2014; 11: 506–15. 67.
34 El-Khatib FM, Towe M, Yafi FA. Management of Peyronie’s disease with 58 Lin H, Liu C, Wang R. Effect of penile traction and vacuum erectile device
collagenase Clostridium histolyticum in the acute phase. World J. Urol. for Peyronie’s disease in an animal model. J Sex Med. 2017; 14: 1270–6.
2020; 38: 299–304. 59 Levine LA, Newell M, Taylor FL. Penile traction therapy for treatment of
35 Levine LA, Larsen SM. Surgery for Peyronie’s disease. Asian J. Androl. Peyronie’s disease: a single-center pilot study. J Sex Med. 2008; 5: 1468–
2013; 15: 27–34. 73.
36 Bella AJ, Lee JC, Grober ED, Carrier S, Benard F, Brock GB. 2018 Cana- 60 Gontero P, Di Marco M, Giubilei G et al. Use of penile extender device in
dian Urological Association guideline for Peyronie’s disease and congenital the treatment of penile curvature as a result of Peyronie’s disease. Results
penile curvature. Can. Urol. Assoc. J. 2018; 12: E197–209. of a phase II prospective study. J Sex Med. 2009; 6: 558–66.
37 Tsambarlis P, Levine LA. Nonsurgical management of Peyronie’s disease. 61 Yafi FA, Pinsky MR, Stewart C et al. The effect of duration of penile trac-
Nat. Rev. Urol. 2019; 16: 172–86. tion therapy in patients undergoing intralesional injection therapy for Pey-
38 Porst H, Burri A. Current strategies in the management of Peyronie’s dis- ronie’s disease. J. Urol. 2015; 194: 754–8.
ease (PD)-results of a survey of 401 sexual medicine experts across Europe. 62 Ziegelmann MJ, Viers BR, Montgomery BD, Avant RA, Savage JB, Trost
J. Sex. Med. 2019; 16: 901–8. LW. Clinical experience with penile traction therapy among men undergo-
39 Chung E, Deyoung L, Brock GB. The role of PDE5 inhibitors in penile ing collagenase Clostridium histolyticum for Peyronie disease. Urology.
septal scar remodeling: assessment of clinical and radiological outcomes. J. 2017; 104: 102–9.
Sex. Med. 2011; 8: 1472–7. 63 Moncada I, Krishnappa P, Romero J et al. Penile traction therapy with the
40 Ferrini MG, Kovanecz I, Nolazco G, Rajfer J, Gonzalez-Cadavid NF. new device ’Penimaster PRO’ is effective and safe in the stable phase of
Effects of long-term vardenafil treatment on the development of fibrotic Peyronie’s disease: a controlled multicentre study. BJU Int. 2019; 123:
plaques in a rat model of Peyronie’s disease. BJU Int. 2006; 97: 625– 694–702.
33. 64 Ziegelmann M, Savage J, Toussi A et al. Outcomes of a novel penile trac-
41 Valente EG, Vernet D, Ferrini MG, Qian A, Rajfer J, Gonzalez-Cadavid tion device in men with Peyronie’s disease: A randomized, single-blind,
NF. L-arginine and phosphodiesterase (PDE) inhibitors counteract fibrosis controlled trial. J. Urol. 2019; 202: 599–610.
in the Peyronie’s fibrotic plaque and related fibroblast cultures. Nitric Oxide 65 Russo GI, Milenkovic U, Hellstrom W, Levine LA, Ralph D, Albersen M.
2003; 9: 229–44. Clinical efficacy of injection and mechanical therapy for Peyronie’s disease:
42 Abern MR, Larsen S, Levine LA. Combination of penile traction, intrale- a systematic review of the literature. Eur. Urol. 2018; 74: 767–81.
sional verapamil, and oral therapies for Peyronie’s disease. J. Sex. Med. 66 Alom M, Sharma KL, Toussi A, Kohler T, Trost L. Efficacy of combined
2012; 9: 288–95. collagenase Clostridium histolyticum and RestoreX penile traction therapy
43 Johnson SM, Mauritson DR, Willerson JT, Hillis LD. A controlled trial of in men with Peyronie’s disease. J. Sex. Med. 2019; 16: 891–900.
verapamil for Prinzmetal’s variant angina. N.. Engl. J. Med. 1981; 304: 67 Levine LA, Merrick PF, Lee RC. Intralesional verapamil injection for the
862–6. treatment of Peyronie’s disease. J. Urol. 1994; 151: 1522–4.
44 Leone M, Giustiniani A, Cecchini AP. Cluster headache: present and future 68 Levine LA, Goldman KE, Greenfield JM. Experience with intraplaque injec-
therapy. Neurol. Sci. 2017; 38: 45–50. tion of verapamil for Peyronie’s disease. J. Urol. 2002; 168: 621–5.
45 Lee RC, Ping JA. Calcium antagonists retard extracellular matrix production 69 Levine LA. Treatment of Peyronie’s disease with intralesional verapamil
in connective tissue equivalent. J. Surg. Res. 1990; 49: 463–6. injection. J. Urol. 1997; 158: 1395–9.
46 Aggeler J, Frisch SM, Werb Z. Changes in cell shape correlate with colla- 70 Bennett NE, Guhring P, Mulhall JP. Intralesional verapamil prevents the
genase gene expression in rabbit synovial fibroblasts. J. Cell Biol. 1984; 98: progression of Peyronie’s disease. Urology 2007; 69: 1181–4.
1662–71. 71 Shirazi M, Haghpanah AR, Badiee M, Afrasiabi MA, Haghpanah S. Effect
47 Fitch WP 3rd, Easterling WJ, Talbert RL, Bordovsky MJ, Mosier M. Topi- of intralesional verapamil for treatment of Peyronie’s disease: a randomized
cal verapamil HCl, topical trifluoperazine, and topical magnesium sulfate single-blind, placebo-controlled study. Int. Urol. Nephrol. 2009; 41: 467–
for the treatment of Peyronie’s disease–a placebo-controlled pilot study. J. 71.
Sex. Med. 2007; 4: 477–84. 72 Duncan MR, Berman B, Nseyo UO. Regulation of the proliferation and
48 Martin DJ, Badwan K, Parker M, Mulhall JP. Transdermal application of biosynthetic activities of cultured human Peyronie’s disease fibroblasts by
verapamil gel to the penile shaft fails to infiltrate the tunica albuginea. J. interferons-alpha, -beta and -gamma. Scand. J. Urol. Nephrol. 1991; 25:
Urol. 2002; 168: 2483–5. 89–94.
49 Levine LA, Estrada CR, Shou W, Cole A. Tunica albuginea tissue analysis 73 Wegner HE, Andresen R, Knipsel HH, Miller K. Treatment of Peyronie’s
after electromotive drug administration. J. Urol. 2003; 169: 1775–8. disease with local interferon-alpha 2b. Eur. Urol. 1995; 28: 236–40.
50 Di Stasi SM, Giannantoni A, Stephen RL et al. A prospective, randomized 74 Ahuja S, Bivalacqua TJ, Case J, Vincent M, Sikka SC, Hellstrom WJ. A
study using transdermal electromotive administration of verapamil and dex- pilot study demonstrating clinical benefit from intralesional interferon alpha
amethasone for Peyronie’s disease. J. Urol. 2004; 171: 1605–8. 2B in the treatment of Peyronie’s disease. J. Androl. 1999; 20: 444–8.
51 Greenfield JM, Shah SJ, Levine LA. Verapamil versus saline in electromo- 75 Hellstrom WJ, Kendirci M, Matern R et al. Single-blind, multicenter, pla-
tive drug administration for Peyronie’s disease: a double-blind, placebo con- cebo controlled, parallel study to assess the safety and efficacy of intrale-
trolled trial. J. Urol. 2007; 177: 972–5. sional interferon alpha-2B for minimally invasive treatment for Peyronie’s
52 Twidwell J, Levine L. Topical treatment for acute phase Peyronie’s disease disease. J. Urol. 2006; 176: 394–8.
utilizing a new gel, H-100: a randomized, prospective, placebo-controlled 76 Kendirci M, Usta MF, Matern RV, Nowfar S, Sikka SC, Hellstrom WJ.
pilot study. Int. J. Impot. Res. 2016; 28: 41–5. The impact of intralesional interferon alpha-2b injection therapy on penile
© 2020 The Japanese Urological Association 11
MJ ZIEGELMANN ET AL.
hemodynamics in men with Peyronie’s disease. J. Sex. Med. 2005; 2: 709– 101 Gholami SS, Lue TF. Correction of penile curvature using the 16-dot plica-
15. tion technique: a review of 132 patients. J. Urol. 2002; 167: 2066–9.
77 Stewart CA, Yafi FA, Knoedler M et al. Intralesional Injection of Inter- 102 Dugi DD 3rd, Morey AF. Penoscrotal plication as a uniform approach to
feron-alpha2b improves penile curvature in men with Peyronie’s disease reconstruction of penile curvature. BJU Int. 2010; 105: 1440–4.
independent of plaque location. J. Urol. 2015; 194: 1704–7. 103 Papagiannopoulos D, Phelps J, Yura E, Levine LA. Surgical outcomes from
78 Nugteren HM, Nijman JM, de Jong IJ, van Driel MF. The association limiting the use of nonabsorbable suture in tunica albuginea plication for
between Peyronie’s and Dupuytren’s disease. Int. J. Impot. Res. 2011; 23: Peyronie’s disease. Int. J. Impot. Res. 2017; 29: 258–61.
142–5. 104 Schwarzer JU, Steinfatt H. Tunica albuginea underlap–a new modification
79 Mills SA, Gelbard MK. Sixty years in the making: collagenase Clostridium of the Nesbit procedure: description of the technique and preliminary
histolyticum, from benchtop to FDA approval and beyond. World J. Urol. results. J. Sex. Med. 2012; 9: 2970–4.
2020; 38: 269–77. 105 Basiri A, Sarhangnejad R, Ghahestani SM, Radfar MH. Comparing absorb-
80 Gelbard MK, Lindner A, Kaufman JJ. The use of collagenase in the treat- able and nonabsorbable sutures in corporeal plication for treatment of con-
ment of Peyronie’s disease. J. Urol. 1985; 134: 280–3. genital penile curvature. Urol. J. 2011; 8: 302–6.
81 Gelbard M, Walsh R, Kaufman JJ. Clostridial collagenase and Peyronie dis- 106 Reddy RS, McKibben MJ, Fuchs JS, Shakir N, Scott J, Morey AF. Plica-
ease. Urology 1980; 15: 536. tion for severe Peyronie’s deformities has similar long-term outcomes to
82 Gelbard M, Lipshultz LI, Tursi J, Smith T, Kaufman G, Levine LA. Phase milder cases. J. Sex. Med. 2018; 15: 1498–505.
2b study of the clinical efficacy and safety of collagenase Clostridium his- 107 Rybak J, Papagiannopoulos D, Levine L. A retrospective comparative study
tolyticum in patients with Peyronie disease. J. Urol. 2012; 187: 2268–74. of traction therapy vs. no traction following tunica albuginea plication or
83 Lipshultz LI, Goldstein I, Seftel AD et al. Clinical efficacy of collagenase partial excision and grafting for Peyronie’s disease: measured lengths and
Clostridium histolyticum in the treatment of Peyronie’s disease by subgroup: patient perceptions. J. Sex. Med. 2012; 9: 2396–403.
results from two large, double-blind, randomized, placebo-controlled, phase 108 Ralph D, Gonzalez-Cadavid N, Mirone V et al. The management of Pey-
III studies. BJU Int. 2015; 116: 650–6. ronie’s disease: evidence-based 2010 guidelines. J. Sex. Med. 2010; 7:
84 Ziegelmann MJ, Levine LA. A modern approach to the clinical evaluation 2359–74.
of Peyronie’s disease in the era of collagenase. J. Sex. Med. 2019; 16: 483– 109 Levine LA, Lenting EL. A surgical algorithm for the treatment of Pey-
8. ronie’s disease. J. Urol. 1997; 158: 2149–52.
85 Abdel Raheem A, Capece M, Kalejaiye O et al. Safety and effectiveness of 110 Leungwattanakij S, Bivalacqua TJ, Reddy S, Hellstrom WJ. Long-term fol-
collagenase Clostridium histolyticum in the treatment of Peyronie’s disease low-up on use of pericardial graft in the surgical management of Peyronie’s
using a new modified shortened protocol. BJU Int. 2017; 120: 717–23. disease. Int. J. Impot. Res. 2001; 13: 183–6.
86 Alom M, Meng Y, Sharma KL, Savage J, Kohler T, Trost L. Safety and 111 Kadioglu A, Kucukdurmaz F, Sanli O. Current status of the surgical man-
efficacy of collagenase Clostridium histolyticum in Peyronie’s disease men agement of Peyronie’s disease. Nat. Rev. Urol. 2011; 8: 95–106.
with ventral curvatures. Urology 2019; 129: 119–25. 112 Levine LA. Partial plaque excision and grafting (PEG) for Peyronie’s dis-
87 Tsambarlis PN, Yong R, Levine LA. Limited success with clostridium col- ease. J. Sex. Med. 2011; 8: 1842–5.
lagenase histolyticum following FDA approval for the treatment of Pey- 113 Hatzichristodoulou G, Tsambarlis P, Kubler H, Levine LA. Peyronie’s graft
ronie’s disease. Int. J. Impot. Res. 2019; 31: 15–9. surgery-tips and tricks from the masters in andrologic surgery. Transl.
88 Yafi FA, Diao L, DeLay KJ et al. Multi-institutional prospective analysis of Androl. Urol. 2017; 6: 645–56.
intralesional injection of collagenase Clostridium histolyticum, tunical plica- 114 Kozacioglu Z, Degirmenci T, Gunlusoy B et al. Effect of tunical defect size
tion, and partial plaque excision and grafting for the management of Pey- after Peyronie’s plaque excision on postoperative erectile function: do cen-
ronie’s disease. Urology 2018; 120: 138–42. timeters matter? Urology 2012; 80: 1051–5.
89 Carson CC 3rd, Sadeghi-Nejad H, Tursi JP et al. Analysis of the clinical 115 Chow AK, Sidelsky SA, Levine LA. Surgical outcomes of plaque excision
safety of intralesional injection of collagenase Clostridium histolyticum and grafting and supplemental tunica albuginea plication for treatment of
(CCH) for adults with Peyronie’s disease (PD). BJU Int. 2015; 116: 815– Peyronie’s disease with severe compound curvature. J. Sex. Med. 2018; 15:
22. 1021–9.
90 Yafi FA, Anaissie J, Zurawin J, Sikka SC, Hellstrom WJ. Results of 116 Lentz AC, Carson CC 3rd. Peyronie’s surgery: graft choices and outcomes.
SMSNA survey regarding complications following intralesional injection Curr. Urol. Rep. 2009; 10: 460–7.
therapy with collagenase Clostridium histolyticum for Peyronie’s disease. J. 117 Brannigan RE, Kim ED, Oyasu R, McVary KT. Comparison of tunica
Sex. Med. 2016; 13: 684–9. albuginea substitutes for the treatment of Peyronie’s disease. J. Urol. 1998;
91 Levine LA, Larsen SM. Surgical correction of persistent Peyronie’s disease 159: 1064–8.
following collagenase Clostridium histolyticum treatment. J. Sex. Med. 118 Garcia-Gomez B, Ralph D, Levine L et al. Grafts for Peyronie’s disease: a
2015; 12: 259–64. comprehensive review. Andrology 2018; 6: 117–26.
92 Chung E, Wang R, Ralph D, Levine L, Brock G. A worldwide survey on 119 Hatzichristodoulou G, Osmonov D, Kubler H, Hellstrom WJG, Yafi FA.
Peyronie’s disease surgical practice patterns among surgeons. J. Sex. Med. Contemporary review of grafting techniques for the surgical treatment of
2018; 15: 568–75. Peyronie’s disease. Sex. Med. Rev. 2017; 5: 544–52.
93 Mobley EM, Fuchs ME, Myers JB, Brant WO. Update on plication proce- 120 Hatzichristodoulou G. Evolution of the surgical sealing patch TachoSil((R))
dures for Peyronie’s disease and other penile deformities. Ther. Adv. Urol. in Peyronie’s disease reconstructive surgery: technique and contemporary
2012; 4: 335–46. literature review. World J. Urol. 2020; 38: 315–21.
94 Pryor JP, Fitzpatrick JM. A new approach to the correction of the penile 121 Chung E, Clendinning E, Lessard L, Brock G. Five-year follow-up of Pey-
deformity in Peyronie’s disease. J. Urol. 1979; 122: 622–3. ronie’s graft surgery: outcomes and patient satisfaction. J. Sex. Med. 2011;
95 Nesbit RM. Congenital curvature of the phallus: report of three cases with 8: 594–600.
description of corrective operation. J. Urol. 1965; 93: 230–2. 122 Rice PG, Somani BK, Rees RW. Twenty years of plaque incision and graft-
96 Yachia D. Modified corporoplasty for the treatment of penile curvature. J. ing for Peyronie’s disease: a review of literature. Sex. Med. 2019; 7: 115–
Urol. 1990; 143: 80–2. 28.
97 Essed E, Schroeder FH. New surgical treatment for Peyronie disease. Urol- 123 Terrier JE, Tal R, Nelson CJ, Mulhall JP. Penile sensory changes after pla-
ogy 1985; 25: 582–7. que incision and grafting surgery for Peyronie’s disease. J. Sex. Med. 2018;
98 Knispel HH, Gonnermann D, Huland H. Modified surgical technique to cor- 15: 1491–7.
rect congenital and acquired penile curvature. Eur. Urol. 1991; 20: 107–12. 124 Lue TF, El-Sakka AI. Lengthening shortened penis caused by Peyronie’s
99 Greenfield JM, Lucas S, Levine LA. Factors affecting the loss of length disease using circular venous grafting and daily stretching with a vacuum
associated with tunica albuginea plication for correction of penile curvature. erection device. J. Urol. 1999; 161: 1141–4.
J. Urol. 2006; 175: 238–41. 125 Flores S, Choi J, Alex B, Mulhall JP. Erectile dysfunction after plaque inci-
100 Baskin LS, Duckett JW. Dorsal tunica albuginea plication for hypospadias sion and grafting: short-term assessment of incidence and predictors. J. Sex.
curvature. J. Urol. 1994; 151: 1668–71. Med. 2011; 8: 2031–7.
12 © 2020 The Japanese Urological Association
Contemporary Peyronie’s disease management
126 Levine LA, Estrada CR. Human cadaveric pericardial graft for the surgical Peyronie’s disease with penile prosthesis and plaque incision. Urology
correction of Peyronie’s disease. J. Urol. 2003; 170: 2359–62. 2019; 129: 113–8.
127 Taylor FL, Abern MR, Levine LA. Predicting erectile dysfunction following 143 Falcone M, Preto M, Ceruti C et al. A Comparative study between 2 differ-
surgical correction of Peyronie’s disease without inflatable penile prosthesis ent grafts used as patches after plaque incision and inflatable penile prosthe-
placement: vascular assessment and preoperative risk factors. J. Sex. Med. sis implantation for end-stage Peyronie’s disease. J. Sex. Med. 2018; 15:
2012; 9: 296–301. 848–52.
128 Papagiannopoulos D, Yura E, Levine L. Examining postoperative outcomes 144 Hatzichristodoulou G. The PICS technique: a novel approach for residual
after employing a surgical algorithm for management of Peyronie’s disease: curvature correction during penile prosthesis implantation in patients with
a single-institution retrospective review. J. Sex. Med. 2015; 12: 1474–80. severe Peyronie’s disease using the collagen fleece TachoSil. J. Sex. Med.
129 Montorsi F, Guazzoni G, Bergamaschi F, Rigatti P. Patient-partner satisfac- 2018; 15: 416–21.
tion with semirigid penile prostheses for Peyronie’s disease: a 5-year fol- 145 Bernal RM, Henry GD. Contemporary patient satisfaction rates for three-
lowup study. J. Urol. 1993; 150: 1819–21. piece inflatable penile prostheses. Adv. Urol. 2012; 2012: 707321.
130 Ghanem HM, Fahmy I, El-Meliegy A. Malleable penile implants without 146 Barton GJ, Carlos EC, Lentz AC. Sexual quality of life and satisfaction
plaque surgery in the treatment of Peyronie’s disease. Int. J. Impot. Res. with penile prostheses. Sex. Med. Rev. 2019; 7: 178–88.
1998; 10: 171–3. 147 Pillay B, Moon D, Love C et al. Quality of life, psychological functioning,
131 Habous M, Tealab A, Farag M et al. Malleable penile implant is an effec- and treatment satisfaction of men who have undergone penile prosthesis sur-
tive therapeutic option in men with Peyronie’s disease and erectile dysfunc- gery following robot-assisted radical prostatectomy. J. Sex. Med. 2017; 14:
tion. Sex. Med. 2018; 6: 24–9. 1612–20.
132 Chung E, Solomon M, DeYoung L, Brock GB. Comparison between AMS 148 Vakalopoulos I, Kampantais S, Ioannidis S et al. High patient satisfaction
700 CX and Coloplast Titan inflatable penile prosthesis for Peyronie’s dis- after inflatable penile prostheses implantation correlates with female partner
ease treatment and remodeling: clinical outcomes and patient satisfaction. J. satisfaction. J. Sex. Med. 2013; 10: 2774–81.
Sex. Med. 2013; 10: 2855–60. 149 Khera M, Bella A, Karpman E et al. Penile prosthesis implantation in
133 Montague DK, Angermeier KW, Lakin MM, Ingleright BJ. AMS 3-piece patients with Peyronie’s disease: results of the PROPPER study demon-
inflatable penile prosthesis implantation in men with Peyronie’s disease: strates a decrease in patient-reported depression. J. Sex. Med. 2018; 15:
comparison of CX and Ultrex cylinders. J. Urol. 1996; 156: 1633–5. 786–8.
134 Levine LA, Benson J, Hoover C. Inflatable penile prosthesis placement in 150 Segal RL, Cabrini MR, Bivalacqua TJ, Burnett AL. Penile straightening
men with Peyronie’s disease and drug-resistant erectile dysfunction: a sin- maneuvers employed during penile prosthesis surgery: technical options and
gle-center study. J. Sex. Med. 2010; 7: 3775–83. outcomes. Int. J. Impot. Res. 2014; 26: 182–5.
135 Mulhall J, Ahmed A, Anderson M. Penile prosthetic surgery for Peyronie’s 151 Wilson SK, Cleves MA, Delk JR 2nd. Long-term followup of treatment for
disease: defining the need for intraoperative adjuvant maneuvers. J. Sex. Peyronie’s disease: modeling the penis over an inflatable penile prosthesis.
Med. 2004; 1: 318–21. J. Urol. 2001; 165: 825–9.
136 Garaffa G, Minervini A, Christopher NA, Minhas S, Ralph DJ. The man- 152 Sansalone S, Garaffa G, Djinovic R et al. Simultaneous penile lengthening
agement of residual curvature after penile prosthesis implantation in men and penile prosthesis implantation in patients with Peyronie’s disease,
with Peyronie’s disease. BJU Int. 2011; 108: 1152–6. refractory erectile dysfunction, and severe penile shortening. J. Sex. Med.
137 Wilson SK, Delk JR 2nd. A new treatment for Peyronie’s disease: modeling 2012; 9: 316–21.
the penis over an inflatable penile prosthesis. J. Urol. 1994; 152: 1121–3. 153 Rolle L, Falcone M, Ceruti C et al. A prospective multicentric international
138 Chung PH, Scott JF, Morey AF. High patient satisfaction of inflatable study on the surgical outcomes and patients’ satisfaction rates of the ’slid-
penile prosthesis insertion with synchronous penile plication for erectile ing’ technique for end-stage Peyronie’s disease with severe shortening of
dysfunction and Peyronie’s disease. J. Sex. Med. 2014; 11: 1593–8. the penis and erectile dysfunction. BJU Int. 2016; 117: 814–20.
139 Shaeer O, Shaeer K, AbdelRahman IFS, Raheem A. Dorsal phalloplasty 154 Egydio PH, Kuehhas FE. The multiple-slit technique (MUST) for penile
accompanying penile prosthesis implantation minimizes penile shortening length and girth restoration. J. Sex. Med. 2018; 15: 261–9.
and improves patient satisfaction. Int. J. Impot. Res. 2019; 31: 276–81. 155 Egydio PH, Kuehhas FE, Valenzuela RJ. Modified sliding technique
140 Hakim LS, Kulaksizoglu H, Hamill BK, Udelson D, Goldstein I. A guide (MoST) for penile lengthening with insertion of inflatable penile prosthesis.
to safe corporotomy incisions in the presence of underlying inflatable penile J. Sex. Med. 2015; 12: 1100–4.
cylinders: results of in vitro and in vivo studies. J. Urol. 1996; 155: 918– 156 Wilson SK, Mora-Estaves C, Egydio P et al. Glans necrosis following
23. penile prosthesis implantation: prevention and treatment suggestions. Urol-
141 Carson CC, Levine LA. Outcomes of surgical treatment of Peyronie’s dis- ogy 2017; 107: 144–8.
ease. BJU Int. 2014; 113: 704–13. 157 Rehman J, Benet A, Melman A. Use of intralesional verapamil to dissolve
142 Farrell MR, Abdelsayed GA, Ziegelmann MJ, Levine LA. A comparison of Peyronie’s disease plaque: a long-term single-blind study. Urology 1998;
hemostatic patches versus pericardium allograft for the treatment of complex 51: 620–6.
© 2020 The Japanese Urological Association 13
You might also like
- Distillation IDocument57 pagesDistillation IOsan ThorpeNo ratings yet
- Surgical Therapies For Parkinson DiseaseDocument13 pagesSurgical Therapies For Parkinson DiseaseAnali Durán CorderoNo ratings yet
- New Insights On Premature EjaculationDocument8 pagesNew Insights On Premature EjaculationTata VioNo ratings yet
- BlastingDocument138 pagesBlastingcklconNo ratings yet
- IGEM-UP-1C Draft For Comment - 2nd Consultation (IGEM-TSP-10-122)Document54 pagesIGEM-UP-1C Draft For Comment - 2nd Consultation (IGEM-TSP-10-122)eastway98100% (2)
- ESRD Case Analysis - Group 4Document34 pagesESRD Case Analysis - Group 4Sean Jeffrey J. FentressNo ratings yet
- Diagnosis and Management of Adoslecent PCOS 2020Document11 pagesDiagnosis and Management of Adoslecent PCOS 2020Awan AndrawinuNo ratings yet
- Nonepileptic Seizures - An Updated ReviewDocument9 pagesNonepileptic Seizures - An Updated ReviewCecilia FRNo ratings yet
- CC Assignments CurrentDocument53 pagesCC Assignments Currentranjeet100% (3)
- S. No Name and Address Form 25 Dated Validupto Form 28 Dated Validupto 1 List of Pharmaceuticals Manufacturing CompaniesDocument58 pagesS. No Name and Address Form 25 Dated Validupto Form 28 Dated Validupto 1 List of Pharmaceuticals Manufacturing CompaniesCampaign Media0% (1)
- Acute PyelonephritisDocument24 pagesAcute Pyelonephritismayey22100% (4)
- Int J of Urology - 2020 - Ziegelmann - Peyronie S Disease Contemporary Evaluation and ManagementDocument13 pagesInt J of Urology - 2020 - Ziegelmann - Peyronie S Disease Contemporary Evaluation and ManagementXisco Lozano SalvaNo ratings yet
- Banno 2017Document2 pagesBanno 2017Amr Amin RagabNo ratings yet
- Parkinson Diseases in The 2020s and Beyond: Replacing Clinico-Pathologic Convergence With Systems Biology DivergenceDocument6 pagesParkinson Diseases in The 2020s and Beyond: Replacing Clinico-Pathologic Convergence With Systems Biology DivergenceAngélicaNo ratings yet
- Articulo Tercer Parcial.Document16 pagesArticulo Tercer Parcial.michaelNo ratings yet
- 6 Brain-Based DyspepsiaDocument9 pages6 Brain-Based Dyspepsiajaswant bhadaneNo ratings yet
- Accepted Manuscript: Clinical Neurology and NeurosurgeryDocument24 pagesAccepted Manuscript: Clinical Neurology and NeurosurgeryEstefani Romero ArriagadaNo ratings yet
- Original Article: Yong June Yang, Jun Sung Koh, Hyo Jung Ko, Kang Joon Cho, Joon Chul Kim, Soo-Jung Lee, and Chi-Un PaeDocument7 pagesOriginal Article: Yong June Yang, Jun Sung Koh, Hyo Jung Ko, Kang Joon Cho, Joon Chul Kim, Soo-Jung Lee, and Chi-Un PaedrilaydacayNo ratings yet
- Peyronie's Disease: A Literature Review On Epidemiology, Genetics, Pathophysiology, Diagnosis and Work-UpDocument10 pagesPeyronie's Disease: A Literature Review On Epidemiology, Genetics, Pathophysiology, Diagnosis and Work-UpAdil BarutNo ratings yet
- PBD in Pediatric AchalasiaDocument6 pagesPBD in Pediatric AchalasiamuhammadfahmanNo ratings yet
- Purpura Trombocitopenica ImunaDocument8 pagesPurpura Trombocitopenica ImunaDenisa Carmen ColiofNo ratings yet
- Huizinga DAN PELTIER 2007Document10 pagesHuizinga DAN PELTIER 2007TriNo ratings yet
- Emergency Delirium in PediatricDocument15 pagesEmergency Delirium in PediatricUzZySusFabregasNo ratings yet
- Brief Resolved Unexplained Event: Child Health UpdateDocument3 pagesBrief Resolved Unexplained Event: Child Health UpdateNATALIA LEMOS CALLENo ratings yet
- 311-Article Text-307-1-10-20140612Document6 pages311-Article Text-307-1-10-20140612Shaun TylerNo ratings yet
- Browse by Topic and Related ItemsDocument12 pagesBrowse by Topic and Related ItemsTony HermawanNo ratings yet
- Postoperative Cognitive Dysfunction and Dementia: What We Need To Know and DoDocument11 pagesPostoperative Cognitive Dysfunction and Dementia: What We Need To Know and Dofulgentius juliNo ratings yet
- Edwards Mark J Why Functional Neurological Disorder IsDocument11 pagesEdwards Mark J Why Functional Neurological Disorder IsSiddika PanjwaniNo ratings yet
- STEP: Simplified Treatment of The Enlarged Prostate: Abstract and IntroductionDocument16 pagesSTEP: Simplified Treatment of The Enlarged Prostate: Abstract and IntroductionDediretz DiyansaNo ratings yet
- Non-Pharmacological Approach in The Management of Functional DyspepsiaDocument10 pagesNon-Pharmacological Approach in The Management of Functional DyspepsiaMarsya Yulinesia LoppiesNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptRobi Khoerul AkbarNo ratings yet
- 1 s2.0 S002234681100933X MainDocument8 pages1 s2.0 S002234681100933X Mainzahoor ul haqNo ratings yet
- Effectiveness of Physiotherapy On Freezing of Gait in Parkinson 'S Disease: A Systematic Review and Meta-AnalysesDocument14 pagesEffectiveness of Physiotherapy On Freezing of Gait in Parkinson 'S Disease: A Systematic Review and Meta-AnalysesAfnes AstrianiNo ratings yet
- PBL 1-1 CFSDocument54 pagesPBL 1-1 CFSsylvia haryantoNo ratings yet
- Kasar Pkmrs BBBDocument5 pagesKasar Pkmrs BBBIriamana Liasyarah MarudinNo ratings yet
- Current Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsDocument6 pagesCurrent Controversies in The Management of Patent Ductus Arteriosus in Preterm InfantsManju KumariNo ratings yet
- Treatment ParkinsonDocument3 pagesTreatment ParkinsonElisabethNo ratings yet
- Critical Care Issues of TheDocument11 pagesCritical Care Issues of TheJEFFERSON MUÑOZNo ratings yet
- Critical Care Issues of TheDocument11 pagesCritical Care Issues of TheJEFFERSON MUÑOZNo ratings yet
- Dyspepsia Management Guidelines For The MillenniumDocument7 pagesDyspepsia Management Guidelines For The MillenniumAlia ZuhriNo ratings yet
- Equilibrio y Movilidad en Pacientes Con Enfermedad de Parkinson Recién Diagnosticada Seguimiento de Cinco Años de Una Cohorte en El Norte de SueciaDocument10 pagesEquilibrio y Movilidad en Pacientes Con Enfermedad de Parkinson Recién Diagnosticada Seguimiento de Cinco Años de Una Cohorte en El Norte de SueciacamilaNo ratings yet
- 88 535 2 PBDocument8 pages88 535 2 PBHellyatill HasanahNo ratings yet
- HD 1Document9 pagesHD 1Muhammad Fajar SodiqNo ratings yet
- Week 5: Case Analysis Addison'S Disease: Omeprazole (Prilosec) 20 MG ODDocument23 pagesWeek 5: Case Analysis Addison'S Disease: Omeprazole (Prilosec) 20 MG ODMaica LectanaNo ratings yet
- World Journal Of: Clinical CasesDocument9 pagesWorld Journal Of: Clinical CasesSahil ANo ratings yet
- Epidemiology of ParkinsonismDocument26 pagesEpidemiology of Parkinsonismelenac67No ratings yet
- Analfissure: Daniel O. Herzig,, Kim C. LuDocument12 pagesAnalfissure: Daniel O. Herzig,, Kim C. LuThomas KlebNo ratings yet
- TMP 34 DADocument5 pagesTMP 34 DAFrontiersNo ratings yet
- Zhao, 2021 PDFDocument10 pagesZhao, 2021 PDFiaw iawNo ratings yet
- Proteinuria en Pacientes Geriatricos Sin ErcDocument9 pagesProteinuria en Pacientes Geriatricos Sin ErcOdaly ReyesNo ratings yet
- 9 PeyronieDocument15 pages9 PeyronieAdil BarutNo ratings yet
- 186-Book Chapter-902-2-10-20210323Document24 pages186-Book Chapter-902-2-10-20210323Yelaena AbrauNo ratings yet
- PPPD Is On A Spectrum in The General PopulationDocument11 pagesPPPD Is On A Spectrum in The General PopulationJuan Hernández GarcíaNo ratings yet
- The Diagnostic and Treatment of Eating DisordersDocument10 pagesThe Diagnostic and Treatment of Eating DisordersCAMILA OSPINA AYALANo ratings yet
- Ard 2009 116053Document6 pagesArd 2009 116053tahirahaniyaNo ratings yet
- Babeo en El ParkinsonDocument3 pagesBabeo en El Parkinsonfernanda cespedesNo ratings yet
- Disfagia y Parkinso2015Document9 pagesDisfagia y Parkinso2015Jose Alfonso Szabo CalvoNo ratings yet
- Symptoms of Depression and Quality of Life in Functional Dyspepsia PatientsDocument6 pagesSymptoms of Depression and Quality of Life in Functional Dyspepsia PatientsReza Ridho PahleviNo ratings yet
- Current Diagnosis and Management of ErectileDocument8 pagesCurrent Diagnosis and Management of ErectileurozerpaNo ratings yet
- Treatment Options For Patellar Tendinopathy: A Systematic ReviewDocument12 pagesTreatment Options For Patellar Tendinopathy: A Systematic ReviewEstefa Roldan RoldanNo ratings yet
- In Uence of A Removable Prosthesis On Oral Health-Related Quality of Life and Mastication in Elders With Parkinson DiseaseDocument6 pagesIn Uence of A Removable Prosthesis On Oral Health-Related Quality of Life and Mastication in Elders With Parkinson DiseaseSantiago ParedesNo ratings yet
- Medical and Surgical Management of Chronic Pelvic Pain: ReviewDocument8 pagesMedical and Surgical Management of Chronic Pelvic Pain: ReviewRafael De Jesus Briceño CarreroNo ratings yet
- Diabetic Neuropathy PDFDocument10 pagesDiabetic Neuropathy PDFMellody YudhashintaNo ratings yet
- Acute Hypotonia in An Infant (2017)Document3 pagesAcute Hypotonia in An Infant (2017)nikos.alexandrNo ratings yet
- Fast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceFrom EverandFast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceNo ratings yet
- (GHS SDS-en) - TAT - SOL-32 - 201901Document5 pages(GHS SDS-en) - TAT - SOL-32 - 201901Ian PrabowoNo ratings yet
- Para Jumbles Test-1Document4 pagesPara Jumbles Test-1vennelaNo ratings yet
- IEE EIA Introduction and ProcessDocument27 pagesIEE EIA Introduction and ProcessHari PyakurelNo ratings yet
- Critec Transient Discriminating MOVTEC: FeaturesDocument2 pagesCritec Transient Discriminating MOVTEC: Featuresphu pham quocNo ratings yet
- Recombinant DNA MCQDocument6 pagesRecombinant DNA MCQChaze WaldenNo ratings yet
- Lesson 1 EBBADocument161 pagesLesson 1 EBBADo Huyen TrangNo ratings yet
- In-Situ AbstDocument5 pagesIn-Situ AbstFahim MunawarNo ratings yet
- OriginalDocument19 pagesOriginalGoma SelvaraniNo ratings yet
- Tacticity, Geometric IsomerismDocument7 pagesTacticity, Geometric IsomerismbornxNo ratings yet
- Analysis of The Components in Moxa Smoke by GC-MS and Preliminary Discussion On Its Toxicity and Side EffectsDocument13 pagesAnalysis of The Components in Moxa Smoke by GC-MS and Preliminary Discussion On Its Toxicity and Side EffectsMariana CanabarroNo ratings yet
- Caced Set2Document19 pagesCaced Set2Anonymous SEDun6PWNo ratings yet
- Science - Grade 5 - Test QuestionsDocument6 pagesScience - Grade 5 - Test QuestionsJeric MaribaoNo ratings yet
- Dungeon Gits: Very Small RoleplayingDocument6 pagesDungeon Gits: Very Small RoleplayingjedvardNo ratings yet
- The Beauty of HolinessDocument5 pagesThe Beauty of HolinessGrace Church Modesto100% (1)
- (Practical Exam) Back Row NotesDocument16 pages(Practical Exam) Back Row NotesKeesha RiveraNo ratings yet
- Assessment in PerDev Modules 3 and 4Document2 pagesAssessment in PerDev Modules 3 and 4Naddy RetxedNo ratings yet
- 2 PerformanceofflowingwellsDocument16 pages2 PerformanceofflowingwellsnciriNo ratings yet
- Types of ProductionDocument2 pagesTypes of ProductionromwamaNo ratings yet
- Digital Photography in OrthodonDocument48 pagesDigital Photography in OrthodonSrinivasan BoovaraghavanNo ratings yet
- Special Project ReportDocument9 pagesSpecial Project ReportSangam PatariNo ratings yet
- Conference Tool Setup - RuckusDocument11 pagesConference Tool Setup - RuckusJohn MontuyaNo ratings yet
- Monobond Etch&PrimeDocument23 pagesMonobond Etch&Primehot_teethNo ratings yet
- TA202A - Manufacturing Processes II Machining Processes and MachinesDocument16 pagesTA202A - Manufacturing Processes II Machining Processes and Machinesprashant vermaNo ratings yet
- Sourcing Report - Iffco Olive OilDocument13 pagesSourcing Report - Iffco Olive OilMatheusNo ratings yet
- The 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsDocument51 pagesThe 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsAmAnDeepSingh100% (1)