You might also like
- Human Biology Lecture NotesDocument6 pagesHuman Biology Lecture NotesGrace Melissa ChoiNo ratings yet
- A Mortal Man’s Guide to Building a Better Upper ChestDocument101 pagesA Mortal Man’s Guide to Building a Better Upper ChestGianniNo ratings yet
- Fundamentals of Nursing: OxygenationDocument56 pagesFundamentals of Nursing: OxygenationFEVIE ANNE BANATAONo ratings yet
- Blair Upper CervicalDocument4 pagesBlair Upper Cervicallopezhectora100% (1)
- Lalpath Shruti ThrroidDocument2 pagesLalpath Shruti ThrroidSatish SrivastavaNo ratings yet
- Evidenced Based ExercisesDocument16 pagesEvidenced Based ExercisesJonalyn EtongNo ratings yet
- Nasm-Cpt Assessment Solutions Table Cpt6-Update PDFDocument1 pageNasm-Cpt Assessment Solutions Table Cpt6-Update PDFNguyễn Tài Đức100% (2)
- VOL 3 - Layout 1Document596 pagesVOL 3 - Layout 1Raluca Crina100% (1)
- Week 3Document7 pagesWeek 3Margarita Kotova100% (2)
- Nasogastric TubeDocument78 pagesNasogastric TubeQuia Benjch Uayan100% (1)
- Maternal Quiz 2Document24 pagesMaternal Quiz 2Aaron ConstantinoNo ratings yet
- Patient Positioning in Operating TheatreDocument52 pagesPatient Positioning in Operating TheatreFatkhul AdhiatmadjaNo ratings yet
- Anatomy of Nervous TissueDocument54 pagesAnatomy of Nervous TissueNand PrakashNo ratings yet
- Head and NeckDocument11 pagesHead and NeckdrsamnNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Understanding the Concept of Srotas in AyurvedaDocument112 pagesUnderstanding the Concept of Srotas in AyurvedaSanjana SajjanarNo ratings yet
- EMERGENCY DRUGSDocument7 pagesEMERGENCY DRUGSJohn Balgoa100% (2)
- Basic Body Mechanics Moving & Positioning: Nursing 114A Care of The Older AdultsDocument44 pagesBasic Body Mechanics Moving & Positioning: Nursing 114A Care of The Older AdultsJonalyn EtongNo ratings yet
- ThyroidDocument84 pagesThyroidMeLissa Pearl GuillermoNo ratings yet
- Cardiac MonitoringDocument19 pagesCardiac MonitoringYaska Musa100% (1)
- MCN II AntepartumDocument28 pagesMCN II AntepartumJharaNo ratings yet
- Naso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringDocument12 pagesNaso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringmeisygraniaNo ratings yet
- 8 Irrigating A ColostomyDocument5 pages8 Irrigating A ColostomyAnn Jalover PerezNo ratings yet
- Administering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESDocument14 pagesAdministering Enema POWERPOINT GIVING ENEMA TO PATIENT, FOR PATIENT WITH GASTROINTESTINAL DISORDERS .. LECTURES, PRINCIPLES AND PROCEDURESPb0% (1)
- Core Elements of Evidence-Bases Gerontological Nursing PracticeDocument15 pagesCore Elements of Evidence-Bases Gerontological Nursing PracticeGrape Juice67% (3)
- National Core Competency StandardsDocument89 pagesNational Core Competency Standardsverna100% (1)
- Republic Act No. 9994 - Expanded Senior Citizens ActDocument29 pagesRepublic Act No. 9994 - Expanded Senior Citizens ActJumen Gamaru TamayoNo ratings yet
- Excretory System NotesDocument10 pagesExcretory System Noteswama ojha100% (1)
- SuctioningDocument31 pagesSuctioningmelanie silvaNo ratings yet
- Tonsillectomy - ORDocument3 pagesTonsillectomy - ORRich John Mercene-NewNo ratings yet
- 11 Core CompetenciesDocument8 pages11 Core CompetenciesJune TorrionNo ratings yet
- Socio-Cultural Aspects of Maternal and Child NursingDocument14 pagesSocio-Cultural Aspects of Maternal and Child NursingShauie CayabyabNo ratings yet
- Colostomy Irrigation ProcedureDocument24 pagesColostomy Irrigation ProcedureJan Federick Bantay100% (1)
- 3.chronic IllnessesDocument51 pages3.chronic IllnessesJonalyn EtongNo ratings yet
- Complication During PregnancyDocument43 pagesComplication During PregnancyRizza Domalaon BalangitanNo ratings yet
- Emergency NursingDocument5 pagesEmergency NursingDerick RanaNo ratings yet
- Disaster Nursing NotesDocument19 pagesDisaster Nursing NotesRoscelin LumenNo ratings yet
- Colostomy CareDocument13 pagesColostomy CareLord Pozak MillerNo ratings yet
- Cardio and Hema - DR PueyoDocument161 pagesCardio and Hema - DR Pueyoapi-3735995100% (2)
- Essential CHN Bag ContentsDocument36 pagesEssential CHN Bag ContentsRomeo RiveraNo ratings yet
- EENT Instillation and IrrigationDocument13 pagesEENT Instillation and Irrigationplebur100% (1)
- ER Nurse ResponsibilitiesDocument2 pagesER Nurse Responsibilitiesjasnate84No ratings yet
- Singapore Nursing Board Review PointersDocument18 pagesSingapore Nursing Board Review PointersRubelyn Arriola Nioko100% (1)
- Evolution of Nursing Research and Role of The Nurse in ResearchDocument3 pagesEvolution of Nursing Research and Role of The Nurse in ResearchAlmer OstreaNo ratings yet
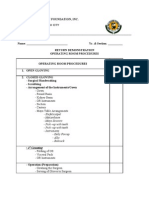
- Or Return Demo FinalDocument2 pagesOr Return Demo FinallemuelNo ratings yet
- Congenital GenitourinaryDocument93 pagesCongenital GenitourinaryEllen AngelNo ratings yet
- At LTC N Theories Models 1Document35 pagesAt LTC N Theories Models 1Darin BransonNo ratings yet
- Skill Performance Evaluation - Measuring Intake and OutputDocument2 pagesSkill Performance Evaluation - Measuring Intake and OutputLemuel Que100% (1)
- Esarean Ction: Cadalin, Fremelen Rose Cedamon, CarloDocument18 pagesEsarean Ction: Cadalin, Fremelen Rose Cedamon, CarloMonette Abalos MendovaNo ratings yet
- VerA Ok-Prelim Ncm104 (Autosaved) VeraDocument30 pagesVerA Ok-Prelim Ncm104 (Autosaved) Verajesperdomincilbayaua100% (1)
- MCN SF Chapter 18 QuizDocument4 pagesMCN SF Chapter 18 QuizKathleen AngNo ratings yet
- HandwashingDocument35 pagesHandwashingJoyce Catherine Buquing UysecoNo ratings yet
- Nursing Skills ChecklistDocument6 pagesNursing Skills Checklistapi-433883631No ratings yet
- Handling Instruments During The Surgical ProcedureDocument4 pagesHandling Instruments During The Surgical ProcedureR-o-N-n-e-l100% (1)
- Nursing Practice Standards2Document25 pagesNursing Practice Standards2sunielgowdaNo ratings yet
- Post Op Worksheet FinalDocument5 pagesPost Op Worksheet FinalRiza Angela BarazanNo ratings yet
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pages) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNo ratings yet
- Pentagon Review - Nursing ManagementDocument5 pagesPentagon Review - Nursing ManagementJay ReanoNo ratings yet
- Leopold'S Maneuver: DefinitionDocument3 pagesLeopold'S Maneuver: DefinitionJyra Mae TaganasNo ratings yet
- Nursing Interventions CHFDocument3 pagesNursing Interventions CHFbanyenye25100% (1)
- Pediatric Oncology Case StudyDocument12 pagesPediatric Oncology Case StudyromelynNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Assessing Uterine Contractions and Fetal Heart Rate During LaborDocument4 pagesAssessing Uterine Contractions and Fetal Heart Rate During LaborRegNo ratings yet
- Fluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementDocument32 pagesFluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementAcohCChaoNo ratings yet
- CHN Health Care Process PDFDocument9 pagesCHN Health Care Process PDFKathleen AngNo ratings yet
- Ctu CCMC Level 3 NCM 1Document15 pagesCtu CCMC Level 3 NCM 1Divina VillarinNo ratings yet
- Acute Respiratory InfectionsDocument18 pagesAcute Respiratory InfectionsEmilyRose17No ratings yet
- Intra-Abdominal Pressure: Causes, Symptoms and TreatmentDocument29 pagesIntra-Abdominal Pressure: Causes, Symptoms and TreatmentRoshin Mae E. TejeroNo ratings yet
- NCM 107 LAB: Catheterization Factors and ProceduresDocument4 pagesNCM 107 LAB: Catheterization Factors and ProceduresCatherine PradoNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen Therapymarie100% (3)
- High-Risk Pregnancy Factors & CareDocument19 pagesHigh-Risk Pregnancy Factors & CareRoger Jr PumarenNo ratings yet
- Nso AbdurasadDocument4 pagesNso AbdurasadNader AbdurasadNo ratings yet
- Pathophysiology of ArrhythmiasDocument15 pagesPathophysiology of ArrhythmiasJonathan MontecilloNo ratings yet
- Perioperative Nursing CareDocument84 pagesPerioperative Nursing CaremarkyboiNo ratings yet
- CHN RVW 2Document51 pagesCHN RVW 2Michael UrrutiaNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- WEEK 2-3 Mod.Document21 pagesWEEK 2-3 Mod.Jonalyn EtongNo ratings yet
- Step 2 of 4: Sources Ofinformatlon Formr. B'S Comprehensive AssessmentDocument3 pagesStep 2 of 4: Sources Ofinformatlon Formr. B'S Comprehensive AssessmentJonalyn EtongNo ratings yet
- Suction Equipment For Airway Clearance InstructionsDocument12 pagesSuction Equipment For Airway Clearance InstructionsJonalyn EtongNo ratings yet
- Understanding The Implications of Birth Weight: 28 DaysDocument5 pagesUnderstanding The Implications of Birth Weight: 28 DaysAdib FraNo ratings yet
- Hmole Case ReviewDocument5 pagesHmole Case ReviewJonalyn EtongNo ratings yet
- Hemodialysis TemplateDocument7 pagesHemodialysis TemplateJonalyn EtongNo ratings yet
- Hmole Case ReviewDocument5 pagesHmole Case ReviewJonalyn EtongNo ratings yet
- Abnormal Breathing PatternsDocument5 pagesAbnormal Breathing PatternsJonalyn EtongNo ratings yet
- Assessing Community Health NeedsDocument6 pagesAssessing Community Health NeedsJonalyn Etong0% (1)
- Epidemiology Public-Health-Key-TermsDocument1 pageEpidemiology Public-Health-Key-TermsJonalyn EtongNo ratings yet
- 7.1 Human Endocrine System - MEMO - ONE PAGER 2020Document1 page7.1 Human Endocrine System - MEMO - ONE PAGER 2020Rudzi UdziNo ratings yet
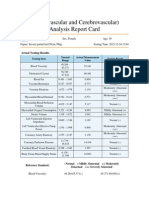
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Most Common CPT CodesDocument5 pagesMost Common CPT CodesKrishna KumarNo ratings yet
- Autonomic Nervous System (ANS)Document11 pagesAutonomic Nervous System (ANS)Prathmesh vetalNo ratings yet
- Stages of Mitosis under MicroscopeDocument21 pagesStages of Mitosis under MicroscopeOM CHAVANNo ratings yet
- Alternativas A TotalesDocument12 pagesAlternativas A TotalesJuan Jose Stuven RodriguezNo ratings yet
- HLTAAP001 Recognise Healthy Body System SAB v3.0 - THEORYDocument41 pagesHLTAAP001 Recognise Healthy Body System SAB v3.0 - THEORYSujan AdhikariNo ratings yet
- The MidbrainDocument3 pagesThe MidbrainAshly Kate AbarientosNo ratings yet
- CT of The Paranasal Sinuses Normal Anatomyvariants and PathologyDocument10 pagesCT of The Paranasal Sinuses Normal Anatomyvariants and PathologyAndi FirdaNo ratings yet
- Operative Otolaryngology Head and Neck SurgeryDocument7 pagesOperative Otolaryngology Head and Neck SurgeryTugce InceNo ratings yet
- Hierarchy of Organization: Associated SLODocument10 pagesHierarchy of Organization: Associated SLOZainne Sarip BandingNo ratings yet
- Lab Report 4 - Cardiovascular Physiology and Blood AgglutinationDocument17 pagesLab Report 4 - Cardiovascular Physiology and Blood AgglutinationHarith HaikalNo ratings yet
- Class 2 EVS (Lesson - 2) TermsDocument7 pagesClass 2 EVS (Lesson - 2) TermsRittwik MandalNo ratings yet
- Boney LandmarksDocument39 pagesBoney LandmarksStefanie Kiss-PlucasNo ratings yet
- Phono TEST 1Document2 pagesPhono TEST 1Thị Anh Thư LêNo ratings yet
- The Slump Test: Examining Spinal Pain and Range of MotionDocument5 pagesThe Slump Test: Examining Spinal Pain and Range of MotionNahu SteinmannNo ratings yet
- Week 3Document10 pagesWeek 3John Chris Villanueva100% (1)
- Physiology of Nerve Fibers: Dr. Zara BatoolDocument30 pagesPhysiology of Nerve Fibers: Dr. Zara BatoolZuhaib AhmedNo ratings yet