You might also like
- The Good Enough Parent: How to raise contented, interesting, and resilient childrenFrom EverandThe Good Enough Parent: How to raise contented, interesting, and resilient childrenRating: 4.5 out of 5 stars4.5/5 (5)
- Concept Check 3 - JB PDFDocument2 pagesConcept Check 3 - JB PDFcdcdiver0% (1)
- SvaliDocument73 pagesSvalitaingsNo ratings yet
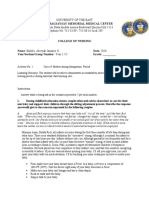
- Module 3 Act 1Document7 pagesModule 3 Act 1Aleeyah Jasmine EmbileNo ratings yet
- Ben Greenfield Bulletproof Your Knee PDFDocument25 pagesBen Greenfield Bulletproof Your Knee PDFhiggs1100% (1)
- The Parent's Guide to Birdnesting: A Child-Centered Solution to Co-Parenting During Separation and DivorceFrom EverandThe Parent's Guide to Birdnesting: A Child-Centered Solution to Co-Parenting During Separation and DivorceNo ratings yet
- Temple Grandin - Movie AnalysisDocument5 pagesTemple Grandin - Movie AnalysisMrinmayee KorgaonkarNo ratings yet
- Preparing Children For Funerals and Memorials: Should I Bring The Kids?Document13 pagesPreparing Children For Funerals and Memorials: Should I Bring The Kids?fabiolaNo ratings yet
- Top Poppin' And Master Mommin': Methods and Lore for ParentingFrom EverandTop Poppin' And Master Mommin': Methods and Lore for ParentingNo ratings yet
- Saying GoodbyeDocument2 pagesSaying GoodbyeJohn DeGarmoNo ratings yet
- Sibling RivalryDocument2 pagesSibling Rivalrycarlokim14No ratings yet
- Helping Children Cope With DeathDocument20 pagesHelping Children Cope With DeathOana CalnegruNo ratings yet
- How The Illuminati Program PeopleDocument5 pagesHow The Illuminati Program Peopleduschis2No ratings yet
- AsynchronousDocument6 pagesAsynchronousNicole Angela MoralesNo ratings yet
- Helping Children Cope With GriefDocument14 pagesHelping Children Cope With GriefjoNo ratings yet
- Grieving ChildrenDocument2 pagesGrieving Childrenapi-371885143No ratings yet
- Health Promotion For The Family With A ToddlerDocument11 pagesHealth Promotion For The Family With A ToddlerROSEVIE MAE ALINGNo ratings yet
- Discipline and Benign NeglectDocument5 pagesDiscipline and Benign NeglectJim GrippoNo ratings yet
- Trauma Series Workbook For WebsiteDocument36 pagesTrauma Series Workbook For WebsiteRafael Sanchez100% (2)
- Razing Your Parents: A Guidebook for Children from Birth to ThreeFrom EverandRazing Your Parents: A Guidebook for Children from Birth to ThreeNo ratings yet
- Helping Children Cope WithDocument25 pagesHelping Children Cope Withbellydanceafrica9540No ratings yet
- Giggle More, Worry Less: A Pediatrician's Thoughts for New ParentsFrom EverandGiggle More, Worry Less: A Pediatrician's Thoughts for New ParentsNo ratings yet
- Bonding, Rooming In-28.4.2020Document34 pagesBonding, Rooming In-28.4.2020santhanalakshmi100% (3)
- BF 01620477Document3 pagesBF 01620477Glăvan AncaNo ratings yet
- Klemp - RandomWalkDocument47 pagesKlemp - RandomWalkweijie908375100% (1)
- Raising A Secure Child SummaryDocument4 pagesRaising A Secure Child Summaryjohn male50% (2)
- Raising Sound Sleepers: Helping Children Use Their Senses to Rest and Self-SootheFrom EverandRaising Sound Sleepers: Helping Children Use Their Senses to Rest and Self-SootheNo ratings yet
- Familybonding en 20141Document14 pagesFamilybonding en 20141api-344569443No ratings yet
- Are Baby Carriers Good For MomsDocument4 pagesAre Baby Carriers Good For MomsGulkhanreaderNo ratings yet
- 3 Helping SIblings CopeDocument6 pages3 Helping SIblings CopeKatherine FuentesNo ratings yet
- Adoption EbookDocument18 pagesAdoption EbookSahil PunjabiNo ratings yet
- The Secret Art of Being a Parent: Tips, tricks, and lifesavers you don't have to learn the hard wayFrom EverandThe Secret Art of Being a Parent: Tips, tricks, and lifesavers you don't have to learn the hard wayRating: 5 out of 5 stars5/5 (2)
- Desmond Morris - Baby WatchingDocument103 pagesDesmond Morris - Baby Watchingdeseixas100% (2)
- Eat, Sleep, Play, Love: A GP's evidence-based and non-judgemental guide to your child's first two yearsFrom EverandEat, Sleep, Play, Love: A GP's evidence-based and non-judgemental guide to your child's first two yearsNo ratings yet
- Some Information About HomesicknessDocument3 pagesSome Information About HomesicknessananaurafloresNo ratings yet
- Happy Kids: The Secrets to Raising Well-Behaved, Contented ChildrenFrom EverandHappy Kids: The Secrets to Raising Well-Behaved, Contented ChildrenRating: 3 out of 5 stars3/5 (1)
- Guardian, The Diabolical Genius of The Baby Advice IndustryDocument9 pagesGuardian, The Diabolical Genius of The Baby Advice IndustrydexthorNo ratings yet
- Module 6 - FILIPINO CULTURE, VALUES AND PRACTICES IN RELATION TO MATERNAL AND CHILD CAREDocument4 pagesModule 6 - FILIPINO CULTURE, VALUES AND PRACTICES IN RELATION TO MATERNAL AND CHILD CAREKatie Holmes0% (1)
- How to Have Happy Children: The little book of commandments for parents of toddlers to teensFrom EverandHow to Have Happy Children: The little book of commandments for parents of toddlers to teensNo ratings yet
- Six Ways of Parenting Under StressDocument33 pagesSix Ways of Parenting Under StressCute Aaliya100% (1)
- The Whole-Brain Child - 1Document8 pagesThe Whole-Brain Child - 1pmkp rsah0% (1)
- Does This Approach Affect Infant-Parent AttachmentDocument4 pagesDoes This Approach Affect Infant-Parent Attachmentsharon vaidesNo ratings yet
- Welcome To Parenthood: A Family GuideDocument66 pagesWelcome To Parenthood: A Family GuideLacatus OlimpiuNo ratings yet
- Child Mind Institute Helping Children Cope After A Traumatic Event 2.25.2022Document15 pagesChild Mind Institute Helping Children Cope After A Traumatic Event 2.25.2022Lim SturxyNo ratings yet
- The Forgotten VoicesDocument66 pagesThe Forgotten VoicesScribdTranslationsNo ratings yet
- HB English SBADocument21 pagesHB English SBAGratel Butcher100% (2)
- 20 Ways To Develop Your Child's CharacterDocument6 pages20 Ways To Develop Your Child's CharacterJesse JosephNo ratings yet
- Second Born ChildDocument2 pagesSecond Born ChildJulie JosephNo ratings yet
- There is No Moon at My House: Parenting Advice from a Veteran School TeacherFrom EverandThere is No Moon at My House: Parenting Advice from a Veteran School TeacherNo ratings yet
- PDF - DOCSrecipesPlaybook - 4-2 - 2013Document16 pagesPDF - DOCSrecipesPlaybook - 4-2 - 2013Eric HoNo ratings yet
- ECHO Parents Tip 2 - Setting Your Child Up For SuccessDocument2 pagesECHO Parents Tip 2 - Setting Your Child Up For SuccessconstantinenerissaNo ratings yet
- Food For Thoughtful Parenting: 12 must-have lists for new parents & young familiesFrom EverandFood For Thoughtful Parenting: 12 must-have lists for new parents & young familiesNo ratings yet
- Explaining To Young Children That Someone Has Died-1Document2 pagesExplaining To Young Children That Someone Has Died-1Emilija MinovaNo ratings yet
- Foundations of Theory and Development - Davis AllisonDocument14 pagesFoundations of Theory and Development - Davis Allisonapi-609125940No ratings yet
- Staying Sane with Baby Brain: Life Lessons and Other Good Ideas for New MothersFrom EverandStaying Sane with Baby Brain: Life Lessons and Other Good Ideas for New MothersNo ratings yet
- Informed Consent For Nursing ProceduresDocument2 pagesInformed Consent For Nursing ProceduresZNo ratings yet
- A Tired BrainDocument3 pagesA Tired BrainSivasonNo ratings yet
- Respiratory Care Pocket Card English v2021.4 Pi58nnDocument2 pagesRespiratory Care Pocket Card English v2021.4 Pi58nnAdina BatajuNo ratings yet
- Soal Bahasa Inggris Try Out 2023Document12 pagesSoal Bahasa Inggris Try Out 2023Ahmddhikky PrasetyoNo ratings yet
- VKV - Kharsang Fitness WeekDocument7 pagesVKV - Kharsang Fitness WeekVivekananda Kendra Vidyalaya Arunachal Pradesh TrustNo ratings yet
- Chapter 3 - Noise PollutionDocument41 pagesChapter 3 - Noise PollutionBright KnightNo ratings yet
- Approach To Patient With Gastrointestinal SystemDocument23 pagesApproach To Patient With Gastrointestinal SystemMarshell TendeanNo ratings yet
- Form 6 Leave Application FormDocument1 pageForm 6 Leave Application FormNard Lastimosa0% (1)
- What Is This Professor Freud Like - KoellreuterDocument140 pagesWhat Is This Professor Freud Like - KoellreuterJose MuñozNo ratings yet
- Presentation On Eating DisordersDocument13 pagesPresentation On Eating Disordersnavjot singh SandhuNo ratings yet
- Process Alarm ManagementDocument123 pagesProcess Alarm ManagementSudarsan Prathipati100% (1)
- Mula Sigiro TmuDocument19 pagesMula Sigiro TmuMulaSigiroNo ratings yet
- Hands-On Experience: Accreditation of Pathology Laboratories According To ISO 15189 Alexandar Tzankova Luigi TornilloaDocument9 pagesHands-On Experience: Accreditation of Pathology Laboratories According To ISO 15189 Alexandar Tzankova Luigi TornilloaofusandeepNo ratings yet
- Behaviour Based Intervention For Occupational Safety - Case StudyDocument8 pagesBehaviour Based Intervention For Occupational Safety - Case StudyAmerico Arizaca AvalosNo ratings yet
- Carillo V PPLDocument9 pagesCarillo V PPLParis LisonNo ratings yet
- CP Discharge PlanDocument2 pagesCP Discharge PlanMike Royzkie RodriguezNo ratings yet
- Texas, Florida Walk Back Reopenings: AbcdeDocument50 pagesTexas, Florida Walk Back Reopenings: Abcdeenock-readersNo ratings yet
- Soal Kelas 12 SmaDocument5 pagesSoal Kelas 12 SmaDavid SyaifudinNo ratings yet
- Form 1.1 Self AssessmentDocument4 pagesForm 1.1 Self AssessmentIct GothongNo ratings yet
- Distal Radius FractureDocument1 pageDistal Radius FractureAlvin Da CostaNo ratings yet
- Letter To 1st SemesterDocument1 pageLetter To 1st Semesterapi-665037718No ratings yet
- Chapter14 Ob Physical and Physiological Changes During PregnancyDocument57 pagesChapter14 Ob Physical and Physiological Changes During Pregnancyth233No ratings yet
- History of Cell LinesDocument9 pagesHistory of Cell LinesSyafiqSidqi SaidiNo ratings yet
- Research Report Bangladesh National Urban Policies and City Profiles For Dhaka and KhulnaDocument156 pagesResearch Report Bangladesh National Urban Policies and City Profiles For Dhaka and KhulnaMehedi Hasan/UDP/BRACNo ratings yet
- Suspension ExamplesDocument6 pagesSuspension ExamplesDivaan Raj KarunakaranNo ratings yet
- 12 Science of EmbodimentDocument5 pages12 Science of EmbodimentfelipeNo ratings yet
- Aim of AyurvedaDocument5 pagesAim of Ayurvedaravisha7kNo ratings yet