You might also like
- New Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)From EverandNew Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)No ratings yet
- Handbook of Autism and Pervasive Developmental Disorders, Assessment, Interventions, and PolicyFrom EverandHandbook of Autism and Pervasive Developmental Disorders, Assessment, Interventions, and PolicyNo ratings yet
- Children's Separation Anxiety Scale (CSAS) : Psychometric PropertiesDocument11 pagesChildren's Separation Anxiety Scale (CSAS) : Psychometric PropertiesYeremias EdwinNo ratings yet
- Escala PhobiaDocument16 pagesEscala PhobiaArshiyaNo ratings yet
- Q Never True Rarely True Sometimes True Often True Very Often True When I Was Growing UpDocument3 pagesQ Never True Rarely True Sometimes True Often True Very Often True When I Was Growing UpAnn Lee'sNo ratings yet
- Junior EpqDocument22 pagesJunior EpqsekiNo ratings yet
- CGAS Ratings GuideDocument9 pagesCGAS Ratings Guidekevin stefano100% (1)
- Personality Assessment ScreenerDocument11 pagesPersonality Assessment ScreenerMay-Anne VillamorNo ratings yet
- BFQ-C - Psychometric Properties of The Big Five Questionnaire-ChildrenDocument115 pagesBFQ-C - Psychometric Properties of The Big Five Questionnaire-ChildrenPantiru GianaNo ratings yet
- CGASDocument4 pagesCGASDinny Atin AmanahNo ratings yet
- Depression HandoutDocument1 pageDepression Handoutapi-290668891No ratings yet
- The Childhood Trauma Questionnaire in ADocument15 pagesThe Childhood Trauma Questionnaire in ATuấn KhangNo ratings yet
- Vol.5 - Midnight DawnDocument28 pagesVol.5 - Midnight DawnMa MelloNo ratings yet
- Pai Adolescent Sample1Document9 pagesPai Adolescent Sample1diablero999No ratings yet
- Anxiety DisorderDocument33 pagesAnxiety DisorderMahmoud SalehNo ratings yet
- Young's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsDocument35 pagesYoung's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsFiona DayNo ratings yet
- CBT Adolescents Participants Manual EngDocument74 pagesCBT Adolescents Participants Manual EngCarlos MoralesNo ratings yet
- Sample: M-Paci Millon Pre-Adolescent Clinical Inventory Interpretive ReportDocument7 pagesSample: M-Paci Millon Pre-Adolescent Clinical Inventory Interpretive ReportNana LoVeNo ratings yet
- A Normative Study of The Raven Coloured Progressive Matrices Test For Omani Children Aged 5-11 YearsDocument15 pagesA Normative Study of The Raven Coloured Progressive Matrices Test For Omani Children Aged 5-11 YearsCH KarimNo ratings yet
- Dass 21Document2 pagesDass 21Djennifer JacomelliNo ratings yet
- Marital Satisfaction Inventory, Revised (MSI-R)Document5 pagesMarital Satisfaction Inventory, Revised (MSI-R)unicorn1979No ratings yet
- Mathers Clinic Dysfunctional Attitude ScaleDocument6 pagesMathers Clinic Dysfunctional Attitude ScaleGraça Maria Ferreira CarvalhoNo ratings yet
- DASI EnglishDocument96 pagesDASI Englishfionachappell79100% (1)
- Shaywitz Et Al 2008 The Education of Dislexic Children PDFDocument30 pagesShaywitz Et Al 2008 The Education of Dislexic Children PDFCatyta123No ratings yet
- ODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14Document2 pagesODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14narcis2009No ratings yet
- MIPS Inventario Millon de Estilos de Personalidad: Institución AñoDocument18 pagesMIPS Inventario Millon de Estilos de Personalidad: Institución AñoDAYANANo ratings yet
- Handouts YBOC Symptom ChecklistDocument2 pagesHandouts YBOC Symptom ChecklistJoem cNo ratings yet
- Cattell CPQDocument98 pagesCattell CPQCarlos Ernesto Villeda Rivera50% (4)
- Pai en Ingles PDFDocument9 pagesPai en Ingles PDFAmelia Bueno SagraNo ratings yet
- A Reliability and Validity Study of The State-Trait Anxiety InventoryDocument5 pagesA Reliability and Validity Study of The State-Trait Anxiety InventoryYilin NgNo ratings yet
- Obsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsDocument6 pagesObsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsJorge VelardeNo ratings yet
- Tip Sheet 4 - The Clock Drawing Test (CDT) : Things To Be Aware of ScoringDocument2 pagesTip Sheet 4 - The Clock Drawing Test (CDT) : Things To Be Aware of ScoringPandu Bagus AllamNo ratings yet
- Norms CTMTDocument9 pagesNorms CTMTJulianaTeixeiraNo ratings yet
- Snap IV Instructions PDFDocument2 pagesSnap IV Instructions PDFCamila Andrea Bravo BugueñoNo ratings yet
- Social Interaction Anxiety ScaleDocument2 pagesSocial Interaction Anxiety ScaleReneah Krisha May MedianoNo ratings yet
- Millon OnlineDocument20 pagesMillon OnlineCristina SelNo ratings yet
- Trs-A: Teacher Rating Scales-Adolescent AgesDocument2 pagesTrs-A: Teacher Rating Scales-Adolescent AgesEspíritu Ciudadano100% (1)
- Wjschne@ilstu - Edu: Wais-IvDocument9 pagesWjschne@ilstu - Edu: Wais-IvJhannNo ratings yet
- Standard ScoringDocument21 pagesStandard Scoringlaureano leonNo ratings yet
- Mmpi 2 MujeresDocument34 pagesMmpi 2 MujeresArnold SantibañezNo ratings yet
- ADHD in The Classroom: Effective Intervention StrategiesDocument9 pagesADHD in The Classroom: Effective Intervention Strategiesblanca_dhNo ratings yet
- ADHD Self Rating Scale For Teenage Girls FullDocument4 pagesADHD Self Rating Scale For Teenage Girls FullManuel VegaNo ratings yet
- Mcmi III NºaDocument342 pagesMcmi III NºaCarolina Torres UllauriNo ratings yet
- Skala Conners Parent Rating ScaleDocument5 pagesSkala Conners Parent Rating ScaleAsri Dwi ChandraNo ratings yet
- CBSE Class 12 Psychology Boards Question Paper Solved 2018Document13 pagesCBSE Class 12 Psychology Boards Question Paper Solved 2018Ashish NarangNo ratings yet
- The Childhood Autism Spectrum Test (CAST) : Yes No Yes No Yes No Yes No Yes NoDocument4 pagesThe Childhood Autism Spectrum Test (CAST) : Yes No Yes No Yes No Yes No Yes NoZainub A KhanNo ratings yet
- HCA YBOCS EditableDocument9 pagesHCA YBOCS EditableSofiaNo ratings yet
- Med 9780190247591 Interactive PDF 009Document2 pagesMed 9780190247591 Interactive PDF 009EuNo ratings yet
- About TheDocument9 pagesAbout TheGabby CrystalNo ratings yet
- The Dyscalculia Checklist: A Checklist For Dyscalculia and Maths Learning DifficultiesDocument3 pagesThe Dyscalculia Checklist: A Checklist For Dyscalculia and Maths Learning DifficultiesCRISTIAN VICENTE CHAMBA CHAMBANo ratings yet
- Home Situations QuestionnaireDocument2 pagesHome Situations QuestionnaireMarina SwansonNo ratings yet
- The Minnesota Dexterity Test: Examiner's ManualDocument18 pagesThe Minnesota Dexterity Test: Examiner's ManualCarlos Andrés NeyraNo ratings yet
- Children and War Foundation The Children'S Impact of Event Scale (13) CRIES-13Document5 pagesChildren and War Foundation The Children'S Impact of Event Scale (13) CRIES-13Sarah GracyntiaNo ratings yet
- CAARS Patient EnglishDocument2 pagesCAARS Patient Englishramav99759No ratings yet
- The Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Document11 pagesThe Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Catalina NedelciuNo ratings yet
- Social Interaction Anxiety Scale (Sias) : NovopsychDocument4 pagesSocial Interaction Anxiety Scale (Sias) : NovopsychShariqaNo ratings yet
- Autism Physician Handbook: Dr. Wendy EdwardsDocument40 pagesAutism Physician Handbook: Dr. Wendy EdwardsAna Maria PaunNo ratings yet
- Pai 1Document6 pagesPai 1arieq bustamanNo ratings yet
- Assessment ToolsDocument74 pagesAssessment ToolsSharvari ShahNo ratings yet
- Yp Core PDFDocument2 pagesYp Core PDFPetra Moala ČipmankNo ratings yet
- Becoming Solution-Focused in Brief Therapy-Brunner - Mazel Inc. (1992)Document289 pagesBecoming Solution-Focused in Brief Therapy-Brunner - Mazel Inc. (1992)Adina RaduNo ratings yet
- Dana - Small@yale - Edu: A, B A, B, C A, B, C A, B A, B A, B A, B A, B A, B, C, DDocument28 pagesDana - Small@yale - Edu: A, B A, B, C A, B, C A, B A, B A, B A, B A, B A, B, C, DAdina RaduNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Liking BMI NutrixivDocument28 pagesLiking BMI NutrixivAdina RaduNo ratings yet
- Bhargav2015 Article SchizophreniaPatientOrSpirituaDocument18 pagesBhargav2015 Article SchizophreniaPatientOrSpirituaAdina RaduNo ratings yet
- Bottesi Millon PdQ4Document17 pagesBottesi Millon PdQ4Adina RaduNo ratings yet
- J L Armentrout PDFDocument480 pagesJ L Armentrout PDFAdina RaduNo ratings yet
- New Text DocumentDocument1 pageNew Text DocumentAdina RaduNo ratings yet
- K DramasDocument1 pageK DramasAdina RaduNo ratings yet
- Miller - The Drama of The Gifted ChildDocument3 pagesMiller - The Drama of The Gifted ChildTopan Setiadi83% (6)
- Saoud 2016Document9 pagesSaoud 2016Yessica ChiuNo ratings yet
- Lee 2021 2Document10 pagesLee 2021 2Aaron BNo ratings yet
- Incident Command System (Ics)Document3 pagesIncident Command System (Ics)Al VinNo ratings yet
- Weekly-Home-Learning-Plan Q1 Week 1Document2 pagesWeekly-Home-Learning-Plan Q1 Week 1Cla RisaNo ratings yet
- Newmicrosoftofficepowerpointpresentation 160410175058 PDFDocument37 pagesNewmicrosoftofficepowerpointpresentation 160410175058 PDFDevrathNo ratings yet
- View Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverDocument8 pagesView Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverMaisa BassiniNo ratings yet
- Erikson's Psycho-Social Theory of DevelopmentDocument10 pagesErikson's Psycho-Social Theory of DevelopmentCielo DasalNo ratings yet
- Tle Grade8 2ndDocument5 pagesTle Grade8 2ndJessaRicoNo ratings yet
- Growth Performance of Broilers Fed Different Levels of PrebioticsDocument7 pagesGrowth Performance of Broilers Fed Different Levels of PrebioticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ch8-Sekaran N BogieDocument61 pagesCh8-Sekaran N BogieSunardi NurcahyonoNo ratings yet
- n703 Chronic Soap NoteDocument3 pagesn703 Chronic Soap NoteJeffrey ViernesNo ratings yet
- Winnicott ch1 PDFDocument18 pagesWinnicott ch1 PDFAlsabila NcisNo ratings yet
- Emergency and Terminal ContraceptionDocument57 pagesEmergency and Terminal ContraceptionKailash NagarNo ratings yet
- Leopolds-Maneuver StudentsDocument40 pagesLeopolds-Maneuver StudentsCarlo GacadNo ratings yet
- Taproots Underlying Principles of Milton Erickson's Therapy and Hypnosis - William Hudson O'HanlonDocument100 pagesTaproots Underlying Principles of Milton Erickson's Therapy and Hypnosis - William Hudson O'HanlonPuruf Puf80% (5)
- ORGANIZATIONAL BEHAVIOUR - The InternDocument4 pagesORGANIZATIONAL BEHAVIOUR - The InternVandanaNo ratings yet
- Text Information and MediaDocument41 pagesText Information and MediaRegine GuavezNo ratings yet
- Hirarc & Aspect ImpactDocument21 pagesHirarc & Aspect ImpactHazru NazriNo ratings yet
- Full Download Reflect and Relate An Introduction To Interpersonal Communication 3rd Edition Mccornack Solutions ManualDocument24 pagesFull Download Reflect and Relate An Introduction To Interpersonal Communication 3rd Edition Mccornack Solutions Manualmauzynessa553100% (36)
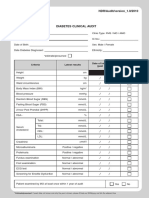
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Housing Colorado in Conjunction With University of Colorado Denver College of Architecture and PlanningDocument7 pagesHousing Colorado in Conjunction With University of Colorado Denver College of Architecture and PlanningAmy NguyenNo ratings yet
- Guideline Perkeni 2019Document29 pagesGuideline Perkeni 2019Tiens MonisaNo ratings yet
- Pig Personality Test Executive SummaryDocument2 pagesPig Personality Test Executive SummaryJanine MagnayeNo ratings yet
- Uncertain Beginnings Learning To Teach Paradoxically PDFDocument6 pagesUncertain Beginnings Learning To Teach Paradoxically PDFBrenda Loiacono CabralNo ratings yet
- DXN ArjunaDocument9 pagesDXN ArjunaABHISHEK PATELNo ratings yet
- Investigation The Effective of The Hazard Identification, Risk Assessment and Determining Control (HIRADC) in Manufacturing ProcessDocument6 pagesInvestigation The Effective of The Hazard Identification, Risk Assessment and Determining Control (HIRADC) in Manufacturing ProcessJames Laurence RavizNo ratings yet
- What Is DehydrationDocument7 pagesWhat Is DehydrationMarwan WijayaNo ratings yet
- Treatment of Insomnia Through The Use of ElectrosleepDocument13 pagesTreatment of Insomnia Through The Use of ElectrosleepEnricoNo ratings yet
- MCQ Test-9 (Module-12)Document5 pagesMCQ Test-9 (Module-12)RH. LIKHON100% (1)