You might also like
- Food Safety Training for Sanitation InspectorsDocument55 pagesFood Safety Training for Sanitation Inspectorsジョンナ メイ ハイミNo ratings yet
- How Much Cost To Start Wheat Flour Mill Factory? How To Make Budget?Document13 pagesHow Much Cost To Start Wheat Flour Mill Factory? How To Make Budget?EDEN2203100% (1)
- Ecophysiology of Pesticides: Interface between Pesticide Chemistry and Plant PhysiologyFrom EverandEcophysiology of Pesticides: Interface between Pesticide Chemistry and Plant PhysiologyNo ratings yet
- Food Safety NotesDocument57 pagesFood Safety NotesChing ChongNo ratings yet
- Bach Flowers CombinationsDocument20 pagesBach Flowers Combinationsraghavan remidicharla100% (3)
- Goat Raising Tips: Pre-Birth and Post-Birth CareDocument38 pagesGoat Raising Tips: Pre-Birth and Post-Birth CareTeodoro Arranguez Jr.100% (1)
- Antibiotics FruitDocument5 pagesAntibiotics FruitxprakashNo ratings yet
- Food Contamination Sources 2018Document9 pagesFood Contamination Sources 2018jorge_bustos_1No ratings yet
- CH04 Food SafetyDocument20 pagesCH04 Food SafetyRianne AuxerreNo ratings yet
- Probiotics in AquacultureDocument7 pagesProbiotics in AquaculturemoiNo ratings yet
- Food SpoilageDocument42 pagesFood Spoilagedrgunavet100% (6)
- Foodborne DiseasesFrom EverandFoodborne DiseasesChristine ER DoddNo ratings yet
- Review 133 PoisningTypesDocument9 pagesReview 133 PoisningTypesEllieNo ratings yet
- Review 133 PoisningTypesDocument9 pagesReview 133 PoisningTypesAldin AhmetovićNo ratings yet
- Journal of Tropical Diseases: A Review On Major Food Borne Bacterial IllnessesDocument7 pagesJournal of Tropical Diseases: A Review On Major Food Borne Bacterial IllnessesGabrielNo ratings yet
- Artigo NutriçãoDocument4 pagesArtigo Nutriçãoannakah18No ratings yet
- Articulo MicrobiologiaDocument13 pagesArticulo Microbiologiatalia XDNo ratings yet
- Food Spoilage PDFDocument42 pagesFood Spoilage PDFVinod KaleNo ratings yet
- Course: Food Safety: Department of Food and Bioresource TechnologyDocument34 pagesCourse: Food Safety: Department of Food and Bioresource TechnologyNgangjoh AlimaNo ratings yet
- Investigation of Alternative Biocidal Options Against Foodborne Multidrug Resistant Pathogens 2020 MayDocument10 pagesInvestigation of Alternative Biocidal Options Against Foodborne Multidrug Resistant Pathogens 2020 MayWill XiaNo ratings yet
- Food Safety in Hospitality Industry: JANUARY 2002Document7 pagesFood Safety in Hospitality Industry: JANUARY 2002Sơn TràNo ratings yet
- Microorganisms Essential For Human Life December 2020 9688126003 1001546Document4 pagesMicroorganisms Essential For Human Life December 2020 9688126003 1001546Obiabo victoriaNo ratings yet
- Antibiotic Use in Animal Feed and Its Impact On Human HealthDocument21 pagesAntibiotic Use in Animal Feed and Its Impact On Human HealthanisarizcaNo ratings yet
- Food Microbiology & ParasitologyDocument138 pagesFood Microbiology & ParasitologynkaitolestephenNo ratings yet
- Acfrogbdptmf56s1siyxu2og1 J8mpghw0xmlmenslfrleoetc66rt7stitnmyxvnbbl2rccbikgrlrtllqdlnljwt6y Adokixllnd6 Rj1cjewjiie7ee4ol1muvu0jof N6vysa79et2lzln7Document5 pagesAcfrogbdptmf56s1siyxu2og1 J8mpghw0xmlmenslfrleoetc66rt7stitnmyxvnbbl2rccbikgrlrtllqdlnljwt6y Adokixllnd6 Rj1cjewjiie7ee4ol1muvu0jof N6vysa79et2lzln7Komang Indra Kurnia TriatmajaNo ratings yet
- Food MicrobiologyDocument2 pagesFood MicrobiologyEditor IJTSRDNo ratings yet
- How Can Microbiology Help Improve Global Food Security?: June 2015Document8 pagesHow Can Microbiology Help Improve Global Food Security?: June 2015Duminda MadushankaNo ratings yet
- The Scourge of Antibiotic Resistance: The Important Role of The EnvironmentDocument7 pagesThe Scourge of Antibiotic Resistance: The Important Role of The EnvironmentMaulida 04No ratings yet
- Fvets 05 00166Document9 pagesFvets 05 00166Aira Jill PadernillaNo ratings yet
- 2014 2 2 3 EnwaDocument10 pages2014 2 2 3 EnwaAdela Cynthia AltairaNo ratings yet
- The Effects of Vegetarian and Vegan Diets On Gut MicrobiotaDocument10 pagesThe Effects of Vegetarian and Vegan Diets On Gut MicrobiotaMARIA ROA FERREIRANo ratings yet
- Relation Between Use of Lincomycin and Outgrowth of YeastDocument62 pagesRelation Between Use of Lincomycin and Outgrowth of Yeastaksonarain1 23No ratings yet
- Foodborne Diseases in India - A Review: British Food Journal May 2012Document22 pagesFoodborne Diseases in India - A Review: British Food Journal May 2012Ayushi srivastavaNo ratings yet
- Food Safety and Hygiene Practices Among Food VendoDocument12 pagesFood Safety and Hygiene Practices Among Food VendodivineotuodichinmaNo ratings yet
- 59 170 1 PBDocument4 pages59 170 1 PBBaja HitamNo ratings yet
- Food Safety in Hospitality Industry: Hari PurnomoDocument6 pagesFood Safety in Hospitality Industry: Hari PurnomoYANNA INGKOHNo ratings yet
- Culinary-Art-Chapter-2Document19 pagesCulinary-Art-Chapter-2sachied1023No ratings yet
- Maam Rita SeminarDocument9 pagesMaam Rita SeminarSOMOSCONo ratings yet
- Food Science - Week 1-3 LessonsDocument64 pagesFood Science - Week 1-3 LessonsArt M. TorresNo ratings yet
- Microbiological SpecificationsDocument26 pagesMicrobiological SpecificationsMatthew MatawoNo ratings yet
- Chapter 3 - Microorganism in FoodDocument20 pagesChapter 3 - Microorganism in Foodnaa znlNo ratings yet
- Molecules 28 01154Document18 pagesMolecules 28 01154Stathis GiaourisNo ratings yet
- Yash Bhargava, Et AlDocument6 pagesYash Bhargava, Et Alamit vishenNo ratings yet
- Biological ContaminationDocument9 pagesBiological ContaminationKamlenduNo ratings yet
- 455 - FST 201 Lecture Note-Dr BabajideDocument18 pages455 - FST 201 Lecture Note-Dr BabajideRochiel ArranchadoNo ratings yet
- Insights Into Insecticide-Resistance Mechanisms in Invasive SpeciesDocument18 pagesInsights Into Insecticide-Resistance Mechanisms in Invasive SpeciesNg Kin HoongNo ratings yet
- Evaluation of Microbiological Safety of Organic and Conventionally Grown RiceDocument7 pagesEvaluation of Microbiological Safety of Organic and Conventionally Grown RiceAdinda MahardikaNo ratings yet
- Escherichia Coli Isolated From Vegans, Vegetarians and Omnivores: Antibiotic Resistance, Virulence Factors, Pathogenicity Islands and Phylogenetic ClassificationDocument11 pagesEscherichia Coli Isolated From Vegans, Vegetarians and Omnivores: Antibiotic Resistance, Virulence Factors, Pathogenicity Islands and Phylogenetic ClassificationJoão Gabriel SonciniNo ratings yet
- Unesco - Eolss Sample Chapters: Food MicrobiologyDocument9 pagesUnesco - Eolss Sample Chapters: Food MicrobiologySamantha SwiftNo ratings yet
- International Journal of Pharmacy and Pharmaceutical SciencesDocument6 pagesInternational Journal of Pharmacy and Pharmaceutical SciencesNurainiManda-MinozNo ratings yet
- Agriculture and Food Animals As A SourceDocument13 pagesAgriculture and Food Animals As A Sourcecata castroNo ratings yet
- Microbiological and Hygienic Quality of Meat and Meat ProductsDocument5 pagesMicrobiological and Hygienic Quality of Meat and Meat ProductsCalidad ElConchelNo ratings yet
- DKG 483Document25 pagesDKG 483Hepy DayanaNo ratings yet
- An Analysis of Microbial Spoilage in Household Food Items and Suggestion To Retard SpoilageDocument12 pagesAn Analysis of Microbial Spoilage in Household Food Items and Suggestion To Retard SpoilageSiti khaizatul minnahNo ratings yet
- Presented By: Sreeraj M. Sreeraj P. ManiDocument166 pagesPresented By: Sreeraj M. Sreeraj P. ManiSREERAJNo ratings yet
- Influence of Hurdle Technology On Foodborne PathogDocument19 pagesInfluence of Hurdle Technology On Foodborne PathogJOMAR HEBREWS REJANONo ratings yet
- European Commission Opinion on Safety Criteria for Micro-Organisms Resistant to AntibioticsDocument21 pagesEuropean Commission Opinion on Safety Criteria for Micro-Organisms Resistant to AntibioticsGatoNo ratings yet
- DocumentDocument19 pagesDocumentGowthami MarreddyNo ratings yet
- Microbial Safety of Dietary SupplementsDocument6 pagesMicrobial Safety of Dietary SupplementsluisaNo ratings yet
- 10 Iajps10062017 PDFDocument10 pages10 Iajps10062017 PDFBaru Chandrasekhar RaoNo ratings yet
- Urban Housing in Nigeria For Sustainable DevelopmeDocument15 pagesUrban Housing in Nigeria For Sustainable DevelopmeRay chijiokeNo ratings yet
- Text File 2Document1 pageText File 2Ray chijiokeNo ratings yet
- Advances in Research On The Carro As An Important Root Vegetable in The Apiaceae FamilyDocument16 pagesAdvances in Research On The Carro As An Important Root Vegetable in The Apiaceae FamilyNelsonNo ratings yet
- Meaning and Purpose in Life and Well-Being: A Life-Span PerspectiveDocument7 pagesMeaning and Purpose in Life and Well-Being: A Life-Span PerspectiveRay chijiokeNo ratings yet
- Sugarcane Growth and Development: International Sugar Journal November 2003Document12 pagesSugarcane Growth and Development: International Sugar Journal November 2003Ray chijiokeNo ratings yet
- Significance of Rural Development: Dr. Radhika KapurDocument16 pagesSignificance of Rural Development: Dr. Radhika KapurRay chijiokeNo ratings yet
- Dogs As Human Companions: A Review of The Relationship: January 1995Document28 pagesDogs As Human Companions: A Review of The Relationship: January 1995Vladut BratfaleanNo ratings yet
- This Is A Post-Print VersionDocument35 pagesThis Is A Post-Print VersionRay chijiokeNo ratings yet
- A Survey of Life Insurance Efficiency Papers MethoDocument34 pagesA Survey of Life Insurance Efficiency Papers MethoRay chijiokeNo ratings yet
- JPSS 18 2 Jan2010Document15 pagesJPSS 18 2 Jan2010Ray chijiokeNo ratings yet
- Ensuring Quality Education for All in Rural CommunitiesDocument5 pagesEnsuring Quality Education for All in Rural CommunitiesMaurício LealNo ratings yet
- Rural DevelopmentDocument7 pagesRural DevelopmentAlexandra UngureanuNo ratings yet
- DiabatesDocument10 pagesDiabatesMuhammad touseefNo ratings yet
- Importance of Urban Development Scenarios For Urban Water Infrastructure Planning and ManagementDocument9 pagesImportance of Urban Development Scenarios For Urban Water Infrastructure Planning and ManagementRay chijiokeNo ratings yet
- Intervention Strategies of Excessive MasturbationDocument12 pagesIntervention Strategies of Excessive MasturbationRay chijiokeNo ratings yet
- ExerciseDocument7 pagesExerciseAjay JethwaNo ratings yet
- The Effect of Sexual Arousal and Emotional ArousalDocument21 pagesThe Effect of Sexual Arousal and Emotional ArousalRay chijiokeNo ratings yet
- An Overview of Food Adulteration: Concept, Sources, Impact, Challenges and DetectionDocument11 pagesAn Overview of Food Adulteration: Concept, Sources, Impact, Challenges and DetectionTalhaNo ratings yet
- Population Africa EconomiaInternazionale PubDocument17 pagesPopulation Africa EconomiaInternazionale PubRay chijiokeNo ratings yet
- Impact of India's Population Growth On Economic Development: ArticleDocument3 pagesImpact of India's Population Growth On Economic Development: ArticleRay chijiokeNo ratings yet
- Proposal of An Implementation Methodology of ICT PDocument18 pagesProposal of An Implementation Methodology of ICT PRay chijiokeNo ratings yet
- The Impact of Population Growth On Economic Development in PakistanDocument10 pagesThe Impact of Population Growth On Economic Development in PakistanZara SajjadNo ratings yet
- Document Analysis BowenDocument15 pagesDocument Analysis BowenEren ŞenNo ratings yet
- Philippine Population Growth and Economic Development: Experience and OptionsDocument39 pagesPhilippine Population Growth and Economic Development: Experience and OptionsRay chijiokeNo ratings yet
- Smoking Research Paper Number 1Document2 pagesSmoking Research Paper Number 1KonchoNo ratings yet
- Oham Sylvia OndaDocument2 pagesOham Sylvia OndaRay chijiokeNo ratings yet
- Journal of Building Construction and Planning ReseDocument2 pagesJournal of Building Construction and Planning Resefadi warthNo ratings yet
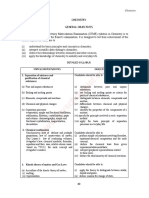
- Chemistry General Objectives: 1. Separation of Mixtures and Purification of Chemical SubstancesDocument13 pagesChemistry General Objectives: 1. Separation of Mixtures and Purification of Chemical SubstancesSara alnaserNo ratings yet
- Biology General ObjectivesDocument12 pagesBiology General ObjectivesRay chijiokeNo ratings yet
- Measurements and Units: PhysicsDocument20 pagesMeasurements and Units: PhysicsSara alnaserNo ratings yet
- An Assessment of Poverty Reduction Strategies in Nigeria (1983 - 2002)Document183 pagesAn Assessment of Poverty Reduction Strategies in Nigeria (1983 - 2002)Padila EphraimNo ratings yet
- History IVC Part 2Document8 pagesHistory IVC Part 2Rohit KumarNo ratings yet
- Call For ProposalDocument26 pagesCall For ProposalNega TewoldeNo ratings yet
- Thesis - Stefano CrispinoDocument45 pagesThesis - Stefano CrispinoStefano CrispinoNo ratings yet
- Price List SKB MT 2023Document2 pagesPrice List SKB MT 2023Syalalal LalalaNo ratings yet
- Malloreddus With Lamb Ragu (Sardinian Gnocchi With Lamb) - The Pasta ProjectDocument2 pagesMalloreddus With Lamb Ragu (Sardinian Gnocchi With Lamb) - The Pasta Projectfrog :pNo ratings yet
- New Methods of Food PreservationDocument18 pagesNew Methods of Food Preservationvasanthi GNo ratings yet
- Group 17Document18 pagesGroup 17Abdul WahabNo ratings yet
- San Francisco ItineraryDocument5 pagesSan Francisco ItineraryAndrew BarrNo ratings yet
- The Lost Rivers of The Forbidden CityDocument6 pagesThe Lost Rivers of The Forbidden CityProbeInternationalNo ratings yet
- Student Caffeine Consumption and FocusDocument2 pagesStudent Caffeine Consumption and FocusPatricia Belle LorenzoNo ratings yet
- MST MCQ U1Document8 pagesMST MCQ U1AyrenNo ratings yet
- Bcom 2 Sem English Compulsory Language 5449 Summer 2019Document3 pagesBcom 2 Sem English Compulsory Language 5449 Summer 2019Adesh SoniNo ratings yet
- New Microsoft Excel WorksheetDocument2,563 pagesNew Microsoft Excel WorksheetBahad IsmayilovNo ratings yet
- Classic Lemon Meringue Pie - Sally's Baking AddictionDocument3 pagesClassic Lemon Meringue Pie - Sally's Baking AddictionGregNo ratings yet
- Fpls 12 630122Document18 pagesFpls 12 630122ValentinaNo ratings yet
- Reading BãDocument42 pagesReading BãNhuỵNo ratings yet
- Restaurant Report Card: July 6, 2023Document7 pagesRestaurant Report Card: July 6, 2023KBTXNo ratings yet
- Easy Homemade Machaca Burritos RecipeDocument1 pageEasy Homemade Machaca Burritos RecipeMichelle Ibarra AmaoNo ratings yet
- Comprehension Practice Tayyab BilalDocument8 pagesComprehension Practice Tayyab BilalTayyab BilalNo ratings yet
- Soal PAS Bhs - Inggris Kelas IXDocument8 pagesSoal PAS Bhs - Inggris Kelas IXsangayu pramiNo ratings yet
- Carapace: A Girl's Difficult ChoiceDocument7 pagesCarapace: A Girl's Difficult ChoiceAnanya SarkarNo ratings yet
- Determining The Optimal Mode of Ordering in Mcdonald'S Between Kiosk Machines and Traditional Cashiers Using Analytical Hierarchy Process (Ahp)Document11 pagesDetermining The Optimal Mode of Ordering in Mcdonald'S Between Kiosk Machines and Traditional Cashiers Using Analytical Hierarchy Process (Ahp)Espinosa, JeikyNo ratings yet
- IBSDocument1 pageIBSIris MambuayNo ratings yet
- A2 EasterDocument97 pagesA2 EasterOlga ZayatsNo ratings yet
- Fedral Urdu University Arts Science and Technology: Assigments of Different TopicsDocument35 pagesFedral Urdu University Arts Science and Technology: Assigments of Different TopicsRida ZehraNo ratings yet
- English Paper 1 Year 4Document13 pagesEnglish Paper 1 Year 4Govin RocketzNo ratings yet